Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
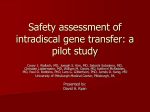
Jpn J Clin Oncol 2009;39(10)625 – 631 doi:10.1093/jjco/hyp094 Original Articles Expression Pattern and Clinical Prognostic Relevance of Bone Morphogenetic Protein-2 in Human Gliomas Ce Liu1,†, Gang Tian2,†, Yanyang Tu3, Jianfang Fu4, Chuan Lan2 and Nan Wu2 1 Department of Neurosurgery, The Second Affiliated Hospital of the General Hospital of the People’s Liberation Army, Beijing, 2Department of Neurosurgery, Southwest Hospital, The Third Military Medical University, Chongqing, 3 Department of Neurosurgery, 63870 Hospital of the People’s Liberation Army and 4Department of Endocrine Secretion, Xijing Hospital of the Fourth Military Medical University, Shanxi, PR China Received April 27, 2009; accepted July 13, 2009 Objective: Bone morphogenetic protein-2 (BMP-2) is normally expressed in the embryo promoting the development of several organs. Aberrant expression of BMP-2 occurs in various tumors. However, a correlation between BMP-2 expression in human gliomas and patients’ prognosis has not been reported. To address this question, this study was to investigate the BMP-2 expression pattern in human gliomas and to evaluate its prognostic relevance. Methods: We analyzed the expression of the BMP-2 antigen in a series of 98 gliomas of various grade and histology by immunohistochemistry on paraffin-embedded sections. Then, the correlation of BMP-2 expression pattern with clinical–pathological features of patients and its prognostic relevance were determined. Results: Immunohistochemical analysis with anti-BMP-2 antibody revealed dense and spotty staining in the tumor cells and its expression levels became significantly higher as the gliomas’ grade advanced (P , 0.001). The median survival of patients with intensively positive BMP-2 expression was significantly shorter than that with negative expression (318 vs. 1197 days, P , 0.0001). The Kaplan – Meier survival curves showed that the BMP-2 expression was not only a significant predictor of survival in high-grade gliomas (grade IV, P ¼ 0.02), but also in lower-grade gliomas (grades II and III, P , 0.001). Conclusions: These results indicate that BMP-2 is a highly sensitive marker for gliomas prognosis and suggest that the expression level of BMP-2 may be a potent tool for the clinical prognosis of gliomas patients. Key words: bone morphogenetic protein-2 – glioma – prognosis INTRODUCTION Gliomas, the most common primary malignant brain tumors, comprise approximately one-third of intrinsic neoplasms of the central nervous system (CNS) in both adults and children (1). Gliomas are divided into four stages, or grades, in increasing level of malignancy according to the World Health Organization (WHO) classification scheme (2). For reprints and all correspondence: Nan Wu, Department of Neurosurgery, Southwest Hospital, The Third Military Medical University, Chongqing 400038, PR China. E-mail: [email protected] † Contribute equally to this work. Grades I and II are the least malignant phenotypes, whereas grades III (anaplastic astrocytoma, anaplastic oligoastrocytoma and anaplastic oligodendroglioma) and IV (glioblastoma multiforme, GBM) constitute the most malignant as well as the most reported glioma histologies. The survival of patients with gliomas is closely related to WHO tumor grade. GBM is the most aggressive gliomas in adults (3). Unfortunately, advances in surgery, radiotherapy and chemotherapy do only have a minor effect on the natural course of this tumor with a mean overall survival time of only 9 – 15 months from the time of diagnosis (4). Therefore, there is an urgent need for more effective therapeutic approaches # The Author (2009). Published by Oxford University Press. All rights reserved. 626 Over-expression of BMP-2 in human gliomas based on a better understanding of the pathophysiologic and molecular properties of gliomas. Bone morphogenetic proteins (BMPs), members of the transforming growth factor-b (TGF-b) superfamily, play an important role in embryonic development events, such as neurogenesis, apoptosis, gastrulation and hematopoiesis (5). It has been demonstrated that some BMPs are implicated in the development of several cancers (6 – 8). BMP-2 was originally described because it induces the entire cascade of endochondral bone formation (9). It is required for normal embryonic development. BMP-2 function as morphogens required for the development of the lung, heart, digits, limbs, CNS and epidermis (10). It enhances cell proliferation, stimulates cell survival pathways and induces self-renewal of stem cells during the development. Interestingly, BMP-2 has been demonstrated to play different roles on cancer cells dependent on the tissue and environment where it is expressed. For example (11), BMP-2 has been shown to stimulate the growth of pancreatic carcinoma cells and prostate cancer cells in the absence of androgen. On the other hand, BMP-2 clearly inhibits the growth of tumor cells of many origins including cancers arising from thyroid, androgen-dependent prostate in the presence of androgen, myeloma, gastric and pancreatic cells. It has also been reported that BMP-2 is over-expressed in 98% of lung carcinomas (12). However, the biological role of BMP-2 in human gliomas has not been elucidated. To address this question, this study was to investigate the BMP-2 expression pattern in human gliomas and to evaluate its prognostic relevance. PATIENTS AND METHODS PATIENTS AND TISSUE SAMPLES Our study was approved by the Ethics Committee of the second affiliated hospital of the General Hospital of the People’s Liberation Army, Beijing, PR China. Ninety-eight Chinese patients with glioma, whose detailed clinical and pathological information was available, were selected from the second affiliated hospital of the General Hospital of the People’s Liberation Army from 11th January 1996 to 7th July 2005. There were 68 males and 30 females (2.267:1), with a mean age of 48.17 years (range from 9 to 76 years). The clinical characteristics of these patients are listed in Table 1. All lesions were classified as primary glioma because the onset of disease was ,3 months before diagnosis and there was no prior history of malignant astrocytoma. Patient characteristics, including the Karnofsky performance scale (KPS) score, were collected before initial surgery. Surgical resection, chemotherapy and radiotherapy were attempted in all patients. Surgically resected tissues were paraffin-embedded, sectioned at 4 mm thickness and used for histochemical and immunohistochemical staining. Two or more pathologists and neurosurgeons classified their grades according to the WHO guidelines. Ten normal brain tissues were used as control samples for the immunohistochemical analysis. All patients were given a follow-up investigation. Total survival time was defined as the time interval between initial craniotomy and the day of the patient’s death. All the patients died of other diseases but not gliomas or unexpected events were excluded from the case collection. IMMUNOHISTOCHEMICAL STAINING The expression levels of BMP-2 in glioma tissues were analyzed by immunohistochemical staining. Tissues were fixed in 10% buffered formalin and embedded in paraffin. Commercially available monoclonal antibody to BMP-2 (Santa CruzTM , USA) was used. Immunohistochemical staining was carried out using the avidin – biotin method and a commercially available kit (Vectastain Elite ABC kit, Vector Laboratories, Burlingame, CA, USA). Deparaffinized Table 1. Clinical characteristics of 98 patients with gliomas included in the population-based immunohistochemical staining WHO grades No. of patients Gender Histology No. of patients Mean age (years) Tumor location Male Female Grade II 17 10 7 Frontal Non-frontal Grade IV Total 35 46 98 20 38 68 15 8 30 Median survival (days) 70 ,70 A 4 45.21 3 1 3 1 1292 (240– 2002) OA 7 47.98 4 3 6 1 1287 (241– 1998) O Grade III KPS 6 46.19 3 3 6 0 1298 (240– 2003) AA 13 49.75 6 7 11 2 372 (33–1538) AOA 11 50.99 4 7 9 2 370 (35–1539) AO 11 50.02 5 6 10 1 375 (33–1531) pGBM 40 48.86 16 24 15 25 330 (32–1890) sGBM 6 49.08 2 4 4 2 327 (29–1886) 98 48.98 43 55 64 34 396 (39–1927) KPS, Karnofsky performance scale; A, astrocytoma; OA, oligoastrocytoma; O, oligodendroglioma; AA, anaplastic astrocytoma; AOA, anaplastic oligoastrocytoma; AO, anaplastic oligodendroglioma; pGBM, primary glioblastoma; sGBM, secondary glioblastoma. Jpn J Clin Oncol 2009;39(10) sections were treated with methanol containing 3% hydrogen peroxide for 10 min before conducting antigen retrieval using a microwave oven at 958C for 5 min and cooling at 258C for 2 h. After washing with phosphate-buffered saline (PBS), blocking serum was applied for 10 min. The sections were incubated with an anti-BMP-2 monoclonal antibody (1:500) overnight at 48C. Negative control sections were incubated with PBS instead of the primary antibody. Then, the section was incubated with a secondary biotinylated antibody (DakoCytomation Inc.) followed by incubation with a streptavidin – peroxidase complex (DakoCytomation Inc.) for 10 min at room temperature. Reaction products were developed using diaminobenzidine containing 0.3% H 2 O 2 as a substrate for peroxidase and nuclei were counterstained with diluted hematoxylin. Positive and negative immunohistochemistry controls were routinely used. Reproducibility of staining was confirmed by reimmunostaining via the same method in multiple, randomly selected specimens. The score of BMP-2 immunoreactivitiy in tissue sections was evaluated according to the intensity of staining (value of 0 for absence, 1 for weak, 2 for moderate, 3 for high and 4 for very high intensity). Each section was independently analyzed in a blind study by two independent observers. STATISTICAL ANALYSIS The software of SPSS version 13.0 for Windows (SPSS Inc., IL, USA) and SAS 9.1 (SAS Institute, Cary, NC, USA) was used for statistical analysis. Continuous variables were expressed as X̄ + s. Statistical analysis were performed with Fisher’s exact test for any 2 2 tables’ Pearson x 2 test for non-2 2 tables, x 2 trend test for ordinal datum, Kaplan – Meier and the Cox regression analysis for the question of survival analysis. A difference between means was considered significant if the P value was ,0.05. RESULTS EXPRESSION OF BMP-2 IN HUMAN GLIOMA TISSUE The expression and location of BMP-2 in 98 patients of primary gliomas were examined using immunostaining analysis. The positive expression rate of BMP-2 (83/98, 84.7%) in patients with gliomas were higher than those in normal brain tissues (both 1/10, 10%) significantly (P , 0.001, Table 2). BMP-2 expression occurred mainly on the cytoplasm, which is similar to the results from previous Table 2. Expression of bone morphogenetic protein-2 (BMP-2) in human gliomas and normal brain tissues Groups No. of patients 0 (n, %) 1þ to 2þ (%) 3þ to 4þ (%) P value Gliomas 98 Normal 10 15 (15.3) 56 (57.1) 9 (90.0) 1 (10%) 27 (27.6) 0 (0) ,0.001 627 studies (13,14). Representative pictures of immunohistochemistry staining of BMP-2 are shown in Fig. 1. CORRELATION OF BMP-2 EXPRESSION WITH GRADING OF HUMAN GLIOMAS THE CLINICAL Table 3 summarizes the substantial differences in BMP-2 expression between tumors of different histologic classifications. In the majority of low-grade tumors (WHO grade II), BMP-2 was either not detectable (5 of 17, 33.3%) or expressed only in 1þ to 2þ intensity (12 of 17, 66.7%). With progression to anaplastic gliomas (WHO grade III) and GBM (WHO grade IV), the percentage of BMP-2-negative tumors were only 22.9% (8 of 35) and 4.4% (2 of 46), whereas the proportion of tumors in which BMP-2 was detectable in 3þ to 4þ intensity were 14.3% (5 of 35, WHO grade III) and 47.8% (22 of 46, WHO grade IV). However, there was no significant difference in BMP-2 expression between tumors of different histologic classifications in the same WHO grade (Grade II – IV: P ¼ 0.32, 0.39 and 0.16, respectively). Fisher’s exact test or x 2 test (Table 4) showed no significant statistical association of BMP-2 expression pattern with age, gender and tumor location (all P . 0.05), indicating that these features might not affect the expression of BMP-2. A significant association of BMP-2 expression pattern with histologic grade and KPS score was observed (P , 0.001 and P ¼ 0.006, respectively). This indicated that patients with GBM (grade IV) and a lower KPS score tend to express a high level of BMP-2. PROGNOSTIC RELEVANCE GLIOMAS OF BMP-2 EXPRESSION IN HUMAN Univariate analyses of each factor with the Cox log-rank analysis (Table 5) show that the histologic grade, KPS score and BMP-2 expression were significantly associated with prognosis. Among them, BMP-2 expression was the most significant (P , 0.0001). The median survival of patients with a high BMP-2 expression level was significantly shorter than those with a low BMP-2 expression level (318 vs. 1197 days, P , 0.0001, Table 5 and Fig. 2A), whereas the BMP-2 expression pattern varied widely in each grade as shown in Table 4. The Kaplan – Meier survival curves (Fig. 2B and C) showed that the BMP-2 expression was not only a significant predictor of survival in high-grade glioma (grade IV, P ¼ 0.0002), but also in lower-grade glioma (grades II and III, P ¼ 0.003). In multivariate analysis, the histologic grade, KPS score and BMP-2 expression were significant predictors of survival (Table 6). These results are consistent with the previous research on other tumors and suggest that the BMP-2 expression, which is inversely correlated with the survival of patients with gliomas, will be a powerful tool for clinical prognosis. 628 Over-expression of BMP-2 in human gliomas Figure 1. Immunohistochemical analysis for anti-human bone morphogenetic protein-2 (BMP-2) antibody. Paraffin-embedded sections of representative gliomas and normal brain tissues were stained with the antibody against human BMP-2. The photograph (A) is a normal brain tissue which showed negative or weak staining for BMP-2. In contrast, the gliomas that have moderate and high expression levels of BMP-2 with dense and spotty staining are shown in (B) and (C), respectively. The photograph (D) shows the negative staining for non-specific antibody. Table 3. BMP-2 expression in human glioma tissues with histologic classification WHO grades No. of patients Histology No. of patients BMP-2 (n, %) 0 Grade II 17 Grade IV 35 46 1þ to 2þ 3þ to 4þ A 4 1 (25.0) 3 (75.0) 0 (0) OA 7 2 (28.6) 5 (72.4) 0 (0) O Grade III P value 6 2 (33.3) 5 (67.7) 0 (0) AA 13 4 (30.8) 8 (61.5) 1 (7.7) AOA 11 2 (18.2) 7 (63.6) 2 (18.2) AO 11 2 (18.2) 7 (63.6) 2 (18.2) pGBM 40 2 (5.0) 20 (50.0) 18 (45.0) sGBM 6 2 (33.3) 4 (66.7) 0 (0) 0.32 0.39 0.16 BMP-2, bone morphogenetic protein-2. DISCUSSION Because patients with similar stages of glioma showed a marked discrepancy in survival, the standard histological methods do not precisely predict which tumors will undergo rapid malignant progression and are difficult to give an accurate prognosis to patients. Several new molecular prognostic factors are being evaluated in the hope that they may contribute to better assessment of the survival probability and, consequently, the tailoring of treatment for each individual patient. In this study, we attempted to clarify the role of BMP-2 in human gliomas. We found that many cells in all grades of glioma stained positive for BMP-2 (Table 2 and Fig. 1). The immunohistological determination of BMP-2 expression alone was strongly associated with the prognosis Jpn J Clin Oncol 2009;39(10) 629 Table 4. BMP-2 expression in human glioma tissues with different clinical–pathological features Clinical– pathological features No. of patients BMP-2 (n, %) 0 P value 1þ to 2þ 3þ to 4þ Histologic classification (WHO) Grade II 17 5 (33.3) 12 (66.7) 0 (0) Grade III 35 8 (22.9) 22 (62.9) 5 (14.3) Grade IV 46 2 (4.4) 22 (47.8) 22 (47.8) ,55 40 6 (15.0) 23 (57.5) 11 (27.5) 55 58 9 (15.5) 33 (56.9) 16 (27.6) Male 68 10 (14.7) 40 (58.8) 18 (26.5) Female 30 5 (16.7) 16 (53.3) 9 (30.0) 70 64 10 (15.6) 42 (65.6) 12 (18.8) ,70 34 5 (14.7) 14 (41.2) 15 (44.1) Frontal 43 6 (14.0) 23 (53.5) 14 (32.6) Non-frontal 55 9 (16.4) 33 (60.0) 13 (23.6) ,0.001 Age 0.32 Gender 0.28 KPS 0.006 Tumor location 0.030 Table 5. Univariate analyses with the Cox log-rank test of the effect on median survival Factors No. of patients Median survival P value 0 15 1197 ,0.0001 1þ to 2þ 56 469 3þ to 4þ 27 318 BMP-2 Histologic classification (WHO) Grade II 17 1269 Grade III 35 371 Grade IV 46 328 ,55 40 728 55 58 307 Male 68 397 Female 30 418 70 64 895 ,70 34 277 Frontal 43 438 Non-frontal 55 392 0.0012 Age 0.1601 Gender 0.2035 KPS 0.0092 Tumor location 0.3196 Figure 2. Kaplan – Meier survival curves defined by the BMP-2 expression of patients with histologic grades II – IV (A) or with grades II and III (B), and IV (C). In each grade, glioma patients with the negative (0) or low (1þ to 2þ) BMP-2 expression survived for significantly longer than those with the high (3þ to 4þ) BMP-2 expression. of glioma patients (Tables 3 – 5 and Fig. 2). The BMP-2 expression pattern was predictive, especially in higher-grade gliomas. In our small series of cases, BMP-2 expression was associated with a poor prognosis and correlated better with clinical course than with the histological grading. Although the prognostic significance of the histological diagnosis strongly depends on the experience of the respective 630 Over-expression of BMP-2 in human gliomas Table 6. Multivariate analyses with the Cox regression model Factors Type P value Relative risk 95% CI for relative risk BMP-2 3þ to 4þ 0.0138 1.887 1.069 3.398 Histologic classification (WHO) Grade IV 0.0302 1.633 1.052 2.823 Age 55 0.2156 1.189 0.733 1.954 Gender Male 0.1933 0.906 0.717 1.851 KPS ,70 0.0208 0.298 0.123 0.592 Tumor location Non-frontal 0.3827 1.372 0.791 2.108 Lower Upper CI, confidence interval. neuropathologist, analysis of both available data sets revealed that BMP-2 expression was superior in predicting the patient’s survival. During normal brain development, stem cells are regulated by BMPs, which signal through the canonical proteins Smad1, Smad5 and Smad8 (15). BMPs are well-characterized inducers of CNS stem cell differentiation, astroglial fate, mitotic arrest and apoptosis; in contrast, the endogenously secreted BMP antagonist Noggin limits glial differentiation and redirects normal post-natal stem cells to generate neurons (16,17). Consistent with this role, BMPs promote the differentiation of glioma-derived precursors; however, BMP application during tumor cell engraftment slowed but did not stop the growth of brain tumors or eventual animal death (18). This suggests that the brain microenvironment counteracts the actions of BMPs in ways not present under culture conditions. Indeed, the continued widespread expression of BMPs in the brain after birth begs the question of how newly forming tumors escape their differentiating effects (19,20). In the present study, we chose BMP-2 from among the other BMPs as our research target because it plays important roles in glial development and it interacts with TGF-b in human glioma to antagonize TGF-b-induced inhibition of multidrug transport (21). The aberrant expression of embryonic proteins in cancer has highlighted the importance of this class of genes in the development of cancer. This is of particular interest since the activities of these embryonic proteins have been shown to be associated with those of BMP-2 during development (22). Recent studies have suggested that tumor growth and metastasis originates from a small subset of cancer cells, which can self-renew to form daughter cells. These studies suggest that tumor growth is dependent on ‘stem cell-like’ tumor cells. It will be of interest to see if BMP-2 regulates stem cell-like cancer cells (23 – 25). We believe that BMP-2 may be a good target for diagnosis and therapy in human gliomas for several reasons. (i) BMP-2 is expressed in the majority of human gliomas. (ii) BMP-2 expression in gliomas is high and there is little to no expression in normal brain tissue, implying that anti-BMP-2 therapy would have minimal toxicity. (iii) BMP-2 expression itself showed a significant correlation with prognosis in patients with gliomas; furthermore, it is not only a significant predictor of survival in high-grade gliomas, but also in lower-grade gliomas. In conclusion, BMP-2 is a highly sensitive marker for gliomas prognosis, suggesting that the expression level of BMP-2 may be a potent tool for the clinical prognosis of gliomas patients. Our findings will not only be useful for understanding glioma, but for effective clinical diagnosis and therapy. Additional studies of in vivo molecular signaling and mechanism to induce a high expression of BMP-2 in glioma are likely to further highlight the advantage of diagnosis with BMP-2. Acknowledgement C.L., G.T. and N.W. carried out the experiment of this manuscript and drafted the manuscript; Y.T. and J.F. participated in the experiment and revised the manuscript, C.L. participated in the design of the study and approved the final manuscript. Conflict of interest statement None declared. References 1. Sun B, Chu D, Li W, Chu X, Li Y, Wei D, et al. Decreased expression of NDRG1 in glioma is related to tumor progression and survival of patients. J Neurooncol doi:10.1007/s11060-009-9859-7. 2. Kleihues P, Sobin LH. World Health Organization classification of tumors. Cancer 2000;88:2887. 3. Ohgaki H, Kleihues P. Epidemiology and etiology of gliomas. Acta Neuropathol 2005;109:93–108. 4. DeAngelis LM. Brain tumors. N Engl J Med 2001;344:114–23. 5. Botchkarev VA, Botchkareva NV, Sharov AA, Funa K, Huber O, Gilchrest BA. Modulation of BMP signaling by noggin is required for induction of the secondary (nontylotrich) hair follicles. J Invest Dermatol 2002;118:3– 10. 6. Hsu MY, Rovinsky S, Penmatcha S, Herlyn M, Muirhead D. Bone morphogenetic proteins in melanoma: angel or devil? Cancer Metastasis Rev 2005;24:251–63. 7. Ye L, Lewis-Russell JM, Kyanaston HG, Jiang WG. Bone morphogenetic proteins and their receptor signaling in prostate cancer. Histol Histopathol 2007;22:1129 –47. 8. Chen D, Zhao M, Mundy GR. Bone morphogenetic proteins. Growth Factors 2004;22:233– 41. 9. Clement JH, Raida M, Sanger J, Bicknell R, Liu J, Naumann A, et al. Bone morphogenetic protein 2 (BMP-2) induces in vitro invasion and in vivo hormone independent growth of breast carcinoma cells. Int J Oncol 2005;27:401– 7. 10. Wen XZ, Miyake S, Akiyama Y, Yuasa Y. BMP-2 modulates the proliferation and differentiation of normal and cancerous gastric cells. Biochem Biophys Res Commun 2004;316:100 –6. 11. Raida M, Clement JH, Ameri K, Han C, Leek RD, Harris AL. Expression of bone morphogenetic protein 2 in breast cancer cells inhibits hypoxic cell death. Int J Oncol 2005;26:1465– 70. Jpn J Clin Oncol 2009;39(10) 12. Langenfeld EM, Bojnowski J, Perone J, Langenfeld J. Expression of bone morphogenetic proteins in human lung carcinomas. Ann Thorac Surg 2005;80:1028 –32. 13. Sugimori K, Matsui K, Motomura H, Tokoro T, Wang J, Higa S, et al. BMP-2 prevents apoptosis of the N1511 chondrocytic cell line through PI3K/Akt-mediated NF-kappaB activation. J Bone Miner Metab 2005;23:411– 9. 14. Le Page C, Puiffe M-L, Meunier L, Zietarska M, de Ladurantaye M, Tonin PN, et al. BMP-2 signaling in ovarian cancer and its association with poor prognosis. J Ovarian Res 2009;2:4. 15. Chen HL, Panchision DM. Concise review: bone morphogenetic protein pleiotropism in neural stem cells and their derivatives – alternative pathways, convergent signals. Stem Cells 2007;25:63 –8. 16. Piccirillo SG, Reynolds BA, Zanetti N. Bone morphogenetic proteins inhibit the tumorigenic potential of human brain tumour-initiating cells. Nature 2006;444:761– 5. 17. Lee J, Son MJ, Woolard K. Epigenetic-mediated dysfunction of the bone morphogenetic protein pathway inhibits differentiation of glioblastoma-initiating cells. Cancer Cell 2008;13:69– 80. 18. Angley C, Kumar M, Dinsio KJ. Signaling by bone morphogenetic proteins and Smad1 modulates the postnatal differentiation of cerebellar cells. J Neurosci 2003;23:260–8. 631 19. Peretto P, Dati C, De Marchis S. Expression of the secreted factors noggin and bone morphogenetic proteins in the subependymal layer and olfactory bulb of the adult mouse brain. Neuroscience 2004;128:685 –96. 20. Lim DA, Tramontin AD, Trevejo JM. Noggin antagonizes BMP signaling to create a niche for adult neurogenesis. Neuron 2000;28:713–26. 21. Chattopadhyay N, T-Felt Hansen J, Godbole MM, Brown EM. Transforming growth factor b receptor family ligands inhibit hepatocyte growth factor synthesis and secretion from astrocytoma cells. Mol Brain Res 2004;121:146 –50. 22. Bhardwaj G, Murdoch B, Wu D. Sonic hedgehog induces the proliferation of primitive human hematopoietic cells via BMP regulation. Nat Immunol 2001;2:172 –80. 23. Shimogori T, Banuchi V, Strauss JB. Embryonic signaling centers expressing BMP, WNT and FGF proteins interact to pattern the cerebral cortex. Development 2004;131:5639–47. 24. de Jong DS, Steegenga WT, Hendriks JM. Regulation of Notch signaling genes during BMP2-induced differentiation of osteoblast precursor cells. Biochem Biophys Res Commun 2004;320:100– 7. 25. Nakayama N, Lee J, Chiu L. Vascular endothelial growth factor synergistically enhances bone morphogenetic protein-4-dependent lymphohematopoietic cell generation from embryonic stem cells in vitro. Blood 2000;95:2275– 83.