Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
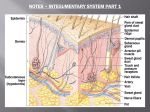
NUR2447 Notes 1. Review anatomy of skin Largest organ Situated externally Covers all internal structures of the body and is the body’s first line of defense Nurses usually observe changes first via and nails Colour: • Note bruising or discolorations or rashes • Skin colour is dependant on melanin, carotene, oxyhaemoglobin and reduced haemoglobin present. • Activity, emotions, smoking, oedemea, respiratory, renal and hepatic disorders can directly affect the colour of skin • • • • Red Colour: o An increase in blood flow to arteries and capillaries causes skin to redden – oxyhemoglobin is a bright red pigment. o Common causes: § Hypertension § Allergies § Dermatitis § Eczema White Pallor: o Decrease in blood flow to capillaries causes whitening o Patient could be cold Blue – cyanosis: o As blood passes through the capillary bed, oxyhemoglobin loses its oxygen to the tissues and becomes dexoxyhemoglobin – a darker and somewhat bluer pigment = cyanosis § Cyanosis may be peripheral or central ú Central = low oxygen levels ú Peripheral = maybe normal response to increase oxygen demands, anxiety, cold or peripheral diseases. Yellow – Jaundice: o High levels of carotene o Predominantly break down of hemoglobin o Causes – hepatitis, cirrhosis, drug induced cholestasis, gall stones, pancreatic carcinoma NUR2447 Notes Consists of two primary layers: • Epidermis: o 5 layers: § Stratum corneum § Stratum lucidum § Stratum granulosum § Stratum spinosum § Stratum basale or germinatum o Other specialized cells include: - Langerhans cells - Melanocytes - Meissner’s corpuscles - Pacinian corpuscles • Dermis: o 2 layers: § Superficial/ Papillary Dermis: ú Connective tissue ú ECM: • Collagen NUR2447 Notes ú ú • • Elastin • Ground substances Fibroblasts: • Fibronectin • Hyaluronic acid (HA) Deep/ Reticular Dermis: • Well vascularized o Larger vessel networks • Larger collagen fibres o Strength • Fibroelastic tissue • Fibroblasts Contains appendages: o Hair follicles o Sebaceous and sweat glands o Finger and toe nails - Subcutaneous tissue: ú Attaches dermis to underlying structures ú Ensures ongoing blood supply to dermis ú Consists primarily of adipose tissue § Cushioning between skin layers and muscle/bone ú Promotes skin mobility ú Provides body contour ú Insulation 2. Review functions of skin Protection: • Keratin: o Ensures moisture balance o Reduces invasion of irritants • Immune cells: - Assist in fighting infection • pH: o Acid mantle on surface of skin § Barrier against bacterial/ fungal infections • Thermoregulation: o Hypothalamus responds to changes in temperature ú Core body temperature ú Surface skin temperature Sensation: • Correct identification of objects through touch • Pleasurable touch • Itch NUR2447 Notes • • Pain Pressure Immune response: • Langerhans cells • Melanocytes • Macrophages • Mast cells Metabolism: • Important in the synthesis of Vitamin D Communication: • Expression • Mood • Cultural differences • Age related changes: • Slowing of overall function of skin • Flattening of epidermal/dermal junction • Decrease in size of Langerhans and melanocyte cells • Decrease in vascular response • Decrease production excess sebum and sweat • Decrease subcutaneous tissue • Decline in general physical condition • Decline in reproduction of the stratum corneum • More susceptible to multiple skin conditions: o “Normal” aging process o Incontinence o Reduced mobility o Increased dependence Any breach to the skin will have consequences: • Disruption to protective barrier NUR2447 Notes • • • • • Increased risk of infection Increases risk of fluid imbalance Increases risk of electrolyte imbalance Impedes normal function May impact on “normal” ADL functioning 3. Develop understanding of phases of wound healing A wound is: A wound may be defined as a defect or break in the skin that results from physical, mechanical or thermal damage or that develops as a result of the presence of an underlying medical or physiological disorder. • It can involve one or all layers of the skin as well as involving deeper damage to muscles, tendons, bones, nerves and blood vessels. Types of wounds: • Contused • Abrasion • Incised • Lacerated • Penetrating • Perforating • Burns • Fracture • Tumour • Ulcer • Acute: o Crush, knife, burn, surgery • Chronic: o Persist beyond normal healing time • Open: o Break present in skin, tissue damage • Closed: o No break, but soft tissue damage is evident Wound healing: 3 stages: • Inflammation: o Immediate response to tissue injury within 2-5 days o Main goals: § Hemostasis § Breakdown debris § Removal of cellular and pathogen debris § Provision of clean wound site o Platelet aggregation o Thromboplastin makes clots NUR2447 Notes o Fibrinolysis o Inflammatory process: § Vasodilation § Increased fluid § Complement system activated § Phagocytosis o Classic features: § Redness § Pain § Heat § Oedema/swelling Reconstruction: • Angiogenesis: o Restore vascularity of wound o Permeable o Oedematous o Supply nutrients and O2 o Granular o Fragile • Collagen synthesis: - Fibroblastic activity - Forms the ECM - Allows keratinocyte migration • Cross linking: o Organisation of collagen fibrils o Increasing tensile strength • Epithelialization: - Migration of cells - Activation of keratinocytes § Cease differentiation - Horizontal movement - Contact inhibition - Deactivation of keratinocytes § Differentiation re-established • Wound contraction: o Pulling wound edges together o Reducing open area o Reducing scar formation o More beneficial in certain areas o Must be balanced • Maturation: § About 3 weeks post injury § 1-2 years § Ongoing remodeling of collagen