Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
TECHNIQUES AND PROCEDURES
Accurate Placement of Central Venous Catheters
Using a 16-cm Catheter
William T. McGee , MD*,
and Kevin P. Moria rty, MDt
McGee \'(IT, Moriarty KP. Accura te placeme nt of central veno us
catheters using a 16-cm Catheter. J Intensive Care Med 1996;
11:19-22 .
We determine ifuse of 16-cm central venous catheter s (Cv'C)
minimizes dangero us intracardiac cathe te r placem e nt s. We
conducted a prospec tive study in a large communi ty teach ing
hosp ltal. Co nsec ut ive pa tients (n = 127) w ho req uired a
eve via ei ther th e internal jug ular (IJV) or th e su bclav ian
vein (SeV) were assessed using 16 (n = 102) or 20-cm (n
= 25) cathe te rs. The ma in outcome measurem en ts were
(1) intracardiac placement of ce nt ral ve nous catheters, and
(2) relationship of right- or left-sided internal jugular o r su b
clavian vein in se rt ion s to int racardi ac ca th e te r placem e nt .
Use of a 20-cm eve resulted in 14 of 25 (56%) intracard iac
p lacements compared wi th [I of [0 2 (1 1%) using a 16-c m
ca th eter (p < 0 .000 1). Al l intracardiac p lacements with the
[6-cm e ve were from right -sided ap p roaches: IJV 7 of 38
(16%), s ev 4 of 18 ( 18%). Use of a l o-cm e v e to access the
cen tral circ ulation fro m either th e sev o r th e I]V resul ts in
a signiJ1cant ly grea te r p rop ortio n of sa fe cathete r placements
than usi ng longer eves, and it sh ou ld becom e the standard
of care .
We re cently reported the high incidence of intr aca r
dia c central ven ou s cathe te r (CVC) placemen ts
using 20- o r 30-cm ce ntral venou s catheter s [1).
CVCs are freq ue ntly placed an d the n left w ith in the
heart desp ite po stp rocedure films that revea l tip
malpositio n [1,21. Extraca rdiac CVC tip p lace ment
co uld e limina te the major mecha nica l caus e of mor
tality related to this p rocedur e : right atrial pe rfo ra
tion an d su bseq ue nt tamponad e [3- 91. A sim ple
way to achieve this resu lt w ithou t mat erially cha ng
ing the way mo st physician s pe rfor m this p rocedure
w ould enhance pati ent safe ty.
We previously d eterm ined that the average sa fe
(i.e ., cathe te r tip above the right atrium ) insertion
di stance for CVCs p laced via the interna l jugu lar or
su bclavian ve in w as 16.5 ern [1). We hyp othesized
that by using 16-cm CVCs p lace d into the interna l
jug ular or su bcl avian ve ins to their full le ngth , we
would substantia lly re du ce the incidence of intra
ca rd ia c catheter tip placement. To test this hyp othe
sis , w e co ndu cted a p rospective trial using 16-cm
CVCs to deter min e the incide nce o f intracardi ac tip
p lacement.
Materials and Met hods
From the Depa rtments of 'Me dicine and "'t Surgcly , Baystare
Medical Center, Springfield, MA.
Received Feb 1,1995, and in revised form Apr 18. Accepted for
publi cation May 9, 1995.
Address corres po ndence to Dr McGee , Baystate Medical Cente r,
759 Chestnut Str, Springfield, MA 01199.
Thi s study was approved by the Instituti onal Re
view Board at Baystate Medi ca l Center. A total o f
127 patients were prospective ly eva luate d fo r the
lo cat ion of CVC (Arro w International, Inc, Reading,
PA) tips p laced by eit her the internal jugular or
su bclavian vei ns. The incid ence of malposition ed
catheters, using our stand ard 20-cm CVC, was d eter
m ine d pro spectively in a to tal of 25 patients. These
cat he te rs w ere pl aced using the accep ted technique
o f es timating appro ximate d istance of insertion by
me asuring the cathete r o n the patients' chest or by
usin g an opera tor-deter min ed prese t dis tance from
an ana tomical inserti on location . The se cat heters
were not rou tine ly pla ce d to thei r en tire le ngt h; 102
16-cm CVCs were placed to their entire length. All
cathe ters were placed by medical, surgical, or anes
the sia res iden ts under the su pervision of the at
tending int en sivist. Im mediate po stprocedure films
w ere evaluated fo r the location of ca theter tip s by
Copy right © 1996 Blackwell Science, Inc.
19
20 Journal of Intensive Care Medicin e Vol 11 No 1 January-Fe bru ary 1996
a radi o logist. The cav al-atrial jun ct ion was dete r
mine d to be at the jun ction of the vertical edg e
and the lo we r convexity of the right mediastinal
co n to ur. The ca theter tip w as deter mined to be in
either a dangerous locatio n (w ithin the heart) or a
sa fe loca tio n (above the su pe rior vena cava-righ t
atria l junction).
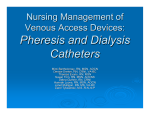
% 16cm
eve in RA
%
20
15
10
Statistics
5
Com pariso ns of th e p ropo rtion of ca the ters p laced
in the heart w ere do ne using Fisher's exact meth od
L1JV
(0/20)
(10].
RIJV
(7/45)
LSCV
(0/15)
RSCV
(4/22)
Fig 2. Of the 16-cm ca theters, no cat he te rs placed from
le ft-sided appro ach es ter m inated with in the heart. The
relative frequ en cies o f right atrial tip locatio n are sh own
for ea ch an atomica l inse rtion locatio n.
Results
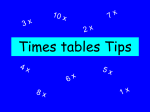
Usin g 20-cm CVCs, 14 (56%) of 25 cathe ters we re
placed w ithin the righ t atriu m (RA); 11 of 102 (11%)
of the 16-cm CVCs had ca theter tip locations w ithin
the RA (p < 0.0001) (Fig 1). The majo rity of the 16
ern catheters were placed in the supe rio r vena ca va
(SCV) ou tside the heart. Thirty five (34%) an d 67
(66%) cath eters w ere place d from left o r right sid e
approaches, respectively. The 11 16-cm catheters
w ithin the heart were all placed from the right side ;
16% (7/ 45) by the int ernal jugu lar vein OJV) and
18% (4/ 22) by the SCV (Fig 2). The dis ta nce with in
the hea rt, beyond the SVC- rig ht atrial junctio n,
ranged from 0.5 to 4.5 em for the right UV and from
1.0 to 2.5 cm for the rig ht SCV approaches . By
location , no ca theter tips placed via left-sid ed ap
proache s w ere w ithin th e hear t (see Fig 2).
16cm vs 20cm: % in RA
Discuss ion
It is widely accepted that CVC tips s ho u ld not be
placed in or allow ed to migrate into the heart ll J.].
A Food and Dru g Administration (FDA) Task For ce
ha s e ven recommended periodic radiographs to
ensure safe ca thete r tip location outside the heart
[12]. Catheter manufac tur ers now routinely include
a warning not ice w ith th e insertio n materials s peci
fying that the tip be placed in an extracardiac loca
tion [13]. Regardless, mo st catheters so ld in the
Uni te d State s are longer than ne cessary (Fig 3)
(Stuckert DH. Pers o nal co mmu n icatio n , 1994) . De-
Estimated U.S.
eve len
eve Market
th in em
%
60
60
50
50
40
40
Ii!IlI% of total market I
30
30
20
20
10
OL-- - - - - - -
- - - -
16cm
20c m
p<O.0001
-./
Fig 1. Use of a I6-cm CVC minim izes right atrial ca the ter
tip placement : 11 vs 56% (p < 0.0001).
12 cm
15 cm
16cm
20cm
30cm
tot al market approx. 2.1 million, total " 100% be cause of small # of many
other size eve
Fig 3. Estimated ma rket for var io us size cathete rs so ld
in the United States as a percent of tot al; 20- and 30-cm
ca theters conti nue to dom inate the mark et share .
McGee and Moriarty: 16-C111 Central Venous Catheters 2 1
spite these warnings and the FDA task force rec om
mendations, ou r curre nt and p rior study using
longer ca theters s how ed that between 47 and 56%
o f a ll ca theter tips ter minated w ithin the RA w he n
using conventiona l place ment tech niq ues Hl. Locat
ing a CVC tip w ithin the he art on a postp rocedu re
film rare ly results in catheter rep o sitio ning [1,2].
Repositio ning takes time and requires the fur ther
expense of an additional radiograp h . An elec trocar
dio gram -guid ed technique usin g the ca the ter tip
as an electrode ide ntifies the sinoatrial node an d
facilitates cathe te r tip p laceme nt in the dista l Sv'C.
Once the SA node is located e lectrocardiograp hi
ca lly, the cathete r is wit hdrawn to the dis ta l SVc.
In our pr ior study using this te chn iq ue , we elimi
nated tip malp osi tion; however, acc eptan ce and ap
plication of this te chnique are not kn own [1]. Wider
dissemination of safe insertion distan ces w ill hope
fully resu lt in clos er a ttention to this aspec t of ce n
tral venous cannu lation . Th e simp les t and th e most
cos t-effective me tho d to avoid intracard iac ca the te r
tip placeme nt may be to choose an a p pro p riate
cathe ter len gth .
No ca theters place d from the left side in our study
terminated w ithin the heart. Th e distance to the RA
from a left-sided appro ach is great er than fro m the
right side. A standa rd inserti on depth o f 13.5 and
11.5 cm from the right subclavian and rig ht IJV,
respectively, would have e lim inated intracard iac
p lace me nt in the 11 pa tient s w hose ca the te rs
(place d from the righ t side) ter min ated within the
heart. Appreciatio n of the shorter d ista nce required
to safely place CVCs by right-Sided ap proache s may
lead to fur ther refine ment of this technique . Other
factor s, including body size, sex, length o f the neck,
and specific insert ion site , all requ ire furthe r study .
Altho ug h catheter tips ca n be safely p laced ou t
side the heart usin g shor ter ca theters , complica tions
related to ca theter angulatio n relativ e to the SVC
should be formally inves tigated . SVC perfo ration by
CVCs does occu r an d carries signific an t mo rbidity
[14-18]. Th is complication seems to be related to
an acute angu lation be twe en the CVC and the SVC
wall [14,15], Dista l tip location in the SVC ab ove
the RAis asso ciated w ith less ac u te angu lation of the
ca the ter compared w ith more p rox ima l locations
within the SVC fo r all approache s other than the
R1] [18- 20]. CVCs placed via the righ t 1] typica lly
end pa rallel to the SVC wall an d min imize ca theter
tip to vein angles (Fig 4). These aspects of central
venous cannu lation related to the use of shor ter
catheter s will need furt her study .
Id eal ca the ter p lacement w ill no t totally eliminate
mechani cal complications related to this procedur e .
Catheter posi tio n is not fixe d, a nd toni city o r o ther
~
I. innominate v.
svc+
RIGHT ATRIUM
Fig 4. Catheter positions relative to the SVC based on
insertion site and proximity to the right atrium. Catheter
angulation relative to the SVC is minimized when the
catheter tip is in the distal SVC near the right atrium for
all insertion locations other than the RIj Y. RIJV insertions
tend to be parallel to the vessel wall regardless of location
within the Sv'C ,
scle ros ing propert ies of intravenous sol u tions can
have a rol e in vessel damage .
Conclusions
Use o f 16-cm CVCs for acc ess to the central circu la
tion from eithe r the intern al jug ular or the subcl a
vian vei n approache s resu lts in a significant ly
greate r proportion of sa fe cathete r place me nts than
when 20-cm evcs are used, and it sho uld become
the stan dard of care . Cath e ters longer tha n 16-cm
sh ould be reserved for spec ial anatomical co nsider
a tions related to patie nt size or more peripheral
insert ion locations. Further studies should be initi
ated wit h shorter ca theters to mak e sure there is
n o increa se in comp licati on s related to SVC perfora
tio n. Use of even shorte r catheters has the pote ntia l
22
Journal of Intensive Care Medi cin e Vol 11 No 1 January-February 1996
to eliminate intracardiac placem ents when using
right -sid ed approaches.
References
1. McGee WT, Ackerman BL, Reu ben LI\, et a l. Accurate p lace
me nt ofcentral venous cath eters: a prosp ective , rand om ized ,
multicenter trial. Crit Care Med 1993;21:1118-11 23
2. Rutherford ]S, Merry AF, Oc clesh aw C.J. De pth of ce ntra l
ve no us catheterization: an audit o f prac tice in a cardiac
surgical unit. Anaestb Intensive Care 1994;22:267-271
3. Edwards H, King TC. Cardia c tamponad e fro m ce ntral ve
nous cat he ters. Arch SUI~~ 1982;1 17:965- 967
4. Delfalque RJ , Camp bell C. Cardiac tam pon ade from central
ve no us cat he ters. A nesthe si ology 1979 ;50:249-252
5. Maschk e SP, Rogove H.J. Cardia c tampo nade associa ted with
a multilumen ce ntra l ven o us ca the ter. Crit Ca re M ed
1984;12:611--613
6. Bar-Joseph G. Ga lvis AG. Perfo ration of the h eart by ce ntra l
veno us catheters in infants: g uide lines to diagnosis a nd man
ageme nt. .f Pediatr Surg 1983;18:284- 287
7. Brandt I(L, Floey WJ, f ink GH , e r al. Mechanis m o f perfor a
tion o f the heart with prod uction of hydrop ericardium by
a venous catheter and its preve ntio n. A ni] Su rg 1970 ;
119:311-316
8. Collie r PE, Ryan JJ, Diam ond DL. Cardiac tampo nade from
central venous catheters- report o f a case and review of
the English literature. Angiolog y 1984;35:595- 600
9. Scott WL. Com plications assoc iated w ith central venou s
ca theters. Ches I 1988 ;94:122 1- 1224
10. Dixon \'{I}, Massey FJ. Introd uction to statistical an alysis .
Ne w Yor k: McGraw-Hili, 1969;242-243
11. Se neff M. Cen tral veno us ca the ters. In: Ripp e JM. Irwin RS,
eds, Inten sive ca re medi cine , ed 2. Bost on , Little , Brown ,
1991;17- 37
12. Fo od a nd Drug Adm inistra tion , Precauti on s necessary w ith
central ve no us catheters, FDA Task Force . In: FDA Drug
Bulletin , Jul y 1989;15-16
13. Arrow ed ucational adv iso ry and ca utions include d as a pack
age insert wit h all CVC kits , Arrow International Inc , Re<ICI
ing , PA, 1989
14. Tocino 1M , Watana be A, Impe nd ing catheter perforation of
superior ven a cava: Radi ograp hic recognition. Am] Roel1/
genoI1986;146:487--490
15 Iberti TT, Katz LB, Reiner MA, er al. Hydrothorax as a later
comp lication of ce nt ral ve no us indwelling catheters. Surgery
1983;94:842-846
16. Vanhe rweghem JL, Cabo let P, Dha e ne M, et al. Compli ca
tions related to subclavian ca theters for he modi alys is. AI/1
.! Nep brol ]986 ;6:539- 345
17. Ellis LM, Voge l 5B, Cope land EM. Centra l veno us cathe te r
vascular erosions, Ann Su rl; 1989 ;209:47 5--478
18. Ka padi a CB, Heard SO, Yesto n NS. Delayed re cogniti on o f
vascular co mp lications cause d by ce ntra l veno us catheters.
J Clin Moni r 1988;4:267-27 1
19. Peres P\\I . POSition ing central ve no us catheters -a prosp ec
tive stud)', A tiaes tb Int e n sive Care 1990;18 :536-539
20. Mallory DL, McGee \\IT, Haake RE, et al. A multi cent er study
evalua tes safety and techn ical aspects of central vascu lar
cannulatio n. A bstr Che st 1989;2(suppl):295