Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Antihypertensive drug wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Coronary artery disease wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
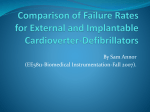
CONTROVERSIES IN CARDIOVASCULAR MEDICINE Should everyone with an ejection fraction less than or equal to 30% receive an implantable cardioverter-defibrillator? Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 Not Everyone With an Ejection Fraction <30% Should Receive an Implantable Cardioverter-Defibrillator Alfred E. Buxton, MD A lthough the total number of deaths attributed to cardiovascular disease has decreased during recent decades, an increase in the percentage of cardiac deaths occurring suddenly (from 56% in 1989 to 63% in 1998) has actually resulted in an increase in the total number of sudden deaths in the United States.1 The problem of sudden death spans all racial and cultural groups and is equally important in men and women. It is now 40 years since continuous ECG monitoring revealed that ventricular tachycardia and ventricular fibrillation (VT/VF) are responsible for the majority of sudden deaths. Dissemination of this information resulted in a marked change in practice. Until the 1970s, physicians treated only symptomatic VTs. Therapeutic options were limited to a few antiarrhythmic drugs, administered empirically. With the advent of telemetric ECG monitoring and continuous ambulatory (Holter) ECG monitoring came the recognition that frequent and multiform ventricular ectopy often preceded episodes of VF in the acute phase of myocardial infarction (MI). Ventricular ectopy and nonsustained VT was documented 1 to 2 weeks after MI in many patients. The presence of frequent ventricular premature complexes and runs of nonsustained VT in patients with significant left ventricular dysfunction were then demonstrated to be an independent predictor of sudden cardiac death late after MI. This information then led to the practice of administering antiarrhythmic drugs to suppress ventricular ectopy under the presumption that suppression of asymptomatic ectopy would prevent sudden death. This fashion lasted almost 20 years, until the results of the Cardiac Arrhythmia Suppression Trial (CAST) trial demonstrated the harm caused by this approach.2 Thus, a sea change in the practice of cardiology had occurred, from treating only symptomatic patients to therapy aimed at primary prevention of sudden death. The initial efforts using antiarrhythmic drugs failed to reduce mortality. While many physicians in the 1970s were administering prophylactic drugs to survivors of MI, Michel Mirowski was developing the implantable cardioverter-defibrillator (ICD), introduced to clinical medicine in 1980.3 It took more than a decade before randomized, controlled trials evaluating the ability of ICDs to reduce mortality in survivors of cardiac arrest or sustained VT appeared in print. These studies demonstrated the superiority of ICDs over amiodarone and other pharmacological agents for secondary prevention of sudden death in survivors of cardiac arrest.4 –7 After publication of the secondary-prevention studies, 3 trials were published demonstrating that ICDs could reduce mortality in patients with chronic coronary disease and The opinions expressed in this article are not necessarily those of the editors or of the American Heart Association. From the Cardiology Division, Brown Medical School, Providence, RI (A.E.B.), and the Cardiology Unit, Department of Medicine, University of Rochester Medical Center, Rochester, New York (A.J.M.). Correspondence to Alfred E. Buxton, MD, Professor of Medicine, Brown University Medical School, 2 Dudley St, Suite 360, Providence, RI 02905 (e-mail [email protected]) or Arthur J. Moss, MD, Heart Research Follow-up Program, Box 653, University of Rochester Medical Center, Rochester, NY 14642 (e-mail [email protected]). (Circulation. 2005;111:2537-2549.) © 2005 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org DOI: 10.1161/01.CIR.0000165057.88551.2C 2537 2538 Circulation May 17, 2005 Relationship of 1-year mortality to EF after MI. The black columns represent mortality reported by the Multicenter Postinfarction Research Group in 198311; the gray columns represent mortality documented by CIMS in 1996.12 Reprinted from Reference 12, Copyright 1996, with permission from the American College of Cardiology Foundation. Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 abnormal left ventricular systolic function that had not yet developed spontaneous sustained VT or VF.8 –10 The first 2 of these trials, the Multicenter Automatic Defibrillator Implantation Trial (MADIT) and Multicenter Unsustained Tachycardia Trial (MUSTT), in addition to requiring that participants have chronic coronary artery disease and abnormal left ventricular function, stipulated that patients have documented nonsustained VT, as well as sustained VT/VF inducible by programmed ventricular stimulation (electrophysiological testing).8,9 The MUSTT trial required patients to have an ejection fraction (EF) ⱕ40% because it is at an EF of 40% that trials in both the pre- and the post-thrombolytic era have shown the break point separating patients at relatively low, versus higher, mortality risk (Figure).11,12 The MADIT investigators required an EF of 35% for entry into that trial.8 These investigators subsequently published a substudy demonstrating that MADIT patients with an EF of 26% to 35% did not have improved survival with an ICD in comparison with those randomized to conventional therapy, whereas patients with an EF ⬍26% did have significantly improved survival with an ICD.13 These findings presumably influenced the design of the MADIT-II trial, in which the major entry requirements were occurrence of MI at least 1 month prior to entry and an EF ⱕ30%.10 It should be noted that although none of these trials required patients to have heart failure, approximately two thirds of patients enrolled in each did have symptomatic heart failure, of New York Heart Association (NYHA) functional class II or III at entry (in MADIT-II, 5% of patients were NYHA functional class IV). Thus, patients enrolled into these trials had advanced coronary disease, marked not only by low EF but also by a high percentage with symptomatic heart failure. More recently, the potential role of ICDs in patients with symptomatic heart failure resulting from both coronary as well as noncoronary disease has been studied.14 –16 These 3 studies all have been marked by relatively low mortality rates in the untreated control arms, and as a result, the first 2 appear to have been somewhat underpowered.14,15 The German Cardiomyopathy Trial enrolled 104 patients with nonischemic dilated cardiomyopathy diagnosed within 9 months, NYHA functional class II or II heart failure symptoms, and an EF ⱕ30%. Patients were randomized to therapy with or without an ICD.14 Although the average EF was 24%, 2-year mortality was ⬍10% in both treatment groups, and no benefit was demonstrated with ICD therapy. The DEFibrillators In Non-Ischemic cardiomyopathy Treatment Evaluation (DEFINITE) trial enrolled 458 patients with nonischemic dilated cardiomyopathy, EF ⱕ35%, a history of symptomatic heart failure, and spontaneous nonsustained VT or frequent ventricular ectopy.15 Patients were randomized to therapy with or without an ICD. The average duration of heart failure at the time of entry into the trial was 2.8 years. The 2-year mortality in the control group was 14.1%. Although the 2-year mortality in the ICD-treated group was 7.9%, the survival difference was not statistically significant. The Sudden Cardiac Death in Heart Failure Trial (SCDHeFT), published earlier this year, enrolled 2521 patients with heart failure resulting from coronary disease or nonischemic dilated cardiomyopathy, NYHA class II or III symptoms for at least 3 months, and EF ⱕ35%. Patients were randomized to 1 of 3 treatments: Placebo, amiodarone, or ICD. Nearly equal numbers of patients with coronary disease and nonischemic cardiomyopathy were enrolled, and the average EF was 25%. The average duration of heart failure symptoms was 2.5 years before enrollment into the trial. The 2-year mortality in the control group was ⬇14%, and mortality in patients randomized to ICD therapy was 23% lower than that of patients randomized to placebo over an average follow-up of almost 4 years (P⫽0.007). Patients with heart failure from nonischemic disease derived a similar amount of benefit from ICD therapy as did patients with coronary disease. Treatment with amiodarone conferred no survival benefit. To summarize briefly, multiple studies completed within the past decade have demonstrated that ICDs can improve survival in patients with coronary artery disease and abnormal left ventricular systolic function, reflected by a variety of EF cutoffs. The most marked ICD survival benefits have been demonstrated in trials that required markers for mortality risk beyond just a reduced EF (such as spontaneous and inducible ventricular arrhythmias). The present mortality of patients with symptomatic heart failure and abnormal left ventricular function resulting from nonischemic cardiomyopathies appears to be lower than that of patients with similar degrees of ventricular dysfunction from coronary disease. It appears that ICD therapy does reduce mortality in the latter patients, but the mortality benefit may be more difficult to demonstrate. Does the demonstration of reduced mortality with ICD therapy in the study populations mean that the entry criteria for the clinical trials should be adapted as our practice guidelines? Also, to address the question at hand, should we base the decision to implant ICDs for primary prevention of sudden death solely on a certain EF value? If we were to implant ICDs in all patients with an EF ⱕ30%, what would be the impact on the overall occurrence of sudden death? If we could demonstrate a causal relationship between a certain critical left ventricular EF and the occurrence of Ejection Fraction and ICD Therapy Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 potentially lethal ventricular tachyarrhythmias, then it would seem rational to base implantation decisions on this factor. Unfortunately, the mechanisms responsible for sudden death are complex. They vary with both the presence and the type of underlying heart disease. In addition, mechanisms underlying arrhythmias may depend on the stage of disease. For example, in patients with coronary artery disease but no previous MI, the most common mechanism responsible for sudden death seems to be ventricular fibrillation induced by acute ischemia. Most of these patients do not have markedly abnormal ventricular function. In fact, in a prospective registry of cardiac arrest in the Netherlands, ⬎50% of the deaths in patients with coronary artery disease occurred in patients whose EF was ⬎30%, and one fifth occurred in patients with an EF ⬎50%.17,18 Once a patient with coronary disease experiences MI, multiple additional mechanisms leading to VT/VF may enter the picture. Intramyocardial reentry resulting from nonuniform anisotropy and other electrophysiological abnormalities created by fibrous tissue formed during the healing process after infarction may result in VT. Such reentry circuits do not require ischemia to become activated. Compensatory hypertrophy in noninfarcted myocardium may predispose to VF.19 Furthermore, occurrence of infarction does not offer protection from recurrent ischemia as a cause of potentially lethal arrhythmias. Progressive ventricular remodeling after infarction may lead to the syndrome of congestive heart failure, with its attendant neural and hormonal abnormalities. In addition, structural and functional abnormalities resulting from remodeling of the left ventricle may by themselves result in ventricular arrhythmias differing in mechanism from reentry or ischemia. Thus, patients with coronary disease are subject to a spectrum of mechanisms that may cause sudden death. These mechanisms do not remain constant; they evolve over the course of the disease. These observations have several implications when trying to develop and apply tests for risk stratification, such as the measurement of ventricular function. That multiple mechanisms may contribute to the occurrence of VT/VF implies that no single test is likely to accurately predict risk of sudden death for all patients. That coronary disease is an evolutionary process suggests that the results of individual tests will not remain stable throughout the course of the disease, and will require repetition. For example, a decreasing EF that does not fall below 30% may carry equal prognostic significance as a markedly reduced (⬍30%), but stable EF; however, I am not aware of any data to substantiate this hypothesis. In addition to the evolutionary nature of both coronary and noncoronary disease, the risk of sudden death is nonlinear over time. Previous analyses have demonstrated a clustering of sudden death events. The period of highest risk is the first 6 to 12 months after infarction, and recurrence of cardiac arrest is highest within the first year after an initial event.20 The current therapies of acute MI, such as thrombolytic therapy and primary angioplasty, as well as the use of -adrenergic blocking agents may be changing this natural 2539 history. A recent prospective survey in Finland showed that total mortality and the occurrence of nonsudden deaths remain highest within the first 18 months after infarction.21 The occurrence of sudden death was delayed, with a majority of events occurring 20 to 40 months after infarction, however. The average EF of patients who died suddenly was 41%, whereas the average EF of patients who experienced nonsudden death was 37%. Importantly, the average EF of patients who died suddenly did not differ significantly from the EF of survivors. The Maastricht Circulatory Arrest Registry in the Netherlands has recently documented that the average time from first infarction to sudden death is 9 years.18 What are the implications if the timing of sudden death after MI is changing? It seems likely that these events result either from a reentrant VT circuit that remained quiescent for years until activated or from anatomic change, such as progressive ventricular remodeling. Could such changes be discovered by periodic remeasurement of EF? Perhaps, but this remains to be proven. Of note, the MADIT-II investigators observed an effect of time from infarction to enrollment in the study on the observed ICD benefit. Patients who entered the trial between 1 and 17 months after the most recent infarction experienced similar survival, whether randomized to ICD or conventional therapy. In contrast, maximal ICD benefit was observed in patients enrolled ⬎10 years after infarction because mortality in the control group was highest in that time period.22 This seems counterintuitive and suggests the possibility of selection bias for enrollment into the trial. Furthermore, the recently reported Defibrillator IN Acute Myocardial Infarction Trial (DINAMIT; a study of prophylactic ICD implantation in patients sustaining an acute MI within the previous 40 days, with EF ⬍35%) also failed to demonstrate improved survival with ICD therapy.23,24 In any case, these observations suggest that EF alone is not sufficient to identify appropriate candidates for ICD therapy. Rather, other clinical factors should influence this decision, possibly including time interval after infarction. If EF were an ideal risk stratification test, then both its sensitivity and specificity would approach 100%, with its predictive accuracy remaining stable over time. If EF warranted consideration as the sole test on which to determine ICD placement, then it would identify patients specifically at risk for sudden death and exclude those likely to die from nonarrhythmic causes. This would be the case if EF directly reflected the pathophysiology underlying sudden death. How close does EF approach these ideals? What is the sensitivity of EF in patients with coronary disease for prediction of sudden death or cardiac arrest? Several lines of evidence suggest EF lacks sufficient sensitivity to be useful by itself. The most recent report from the Maastricht prospective registry found that only 19% of patients with known coronary disease who experienced cardiac arrest had an EF ⱕ30% before the event.18 An earlier report from the same registry demonstrated that the EF was 2540 Circulation May 17, 2005 Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 ⬎30% in 56.5% of patients with a documented infarction who subsequently experienced cardiac arrest.17 The limited sensitivity of EF to predict risk of sudden death also is illustrated by the European Autonomic Tone and Reflexes After Myocardial Infarction (ATRAMI) study (1284 patients enrolled within 1 month of acute MI who underwent multiple risk stratification tests).25 In this study, the mean EF was 49%.25 After an average follow-up of 21 months, a total of 49 deaths occurred. In only 22 of those experiencing cardiac arrest after infarction was the EF ⬍35% when measured early after MI. We also can examine the EF in survivors of cardiac arrest. The average value of EF measured in the Antiarrhythmics Versus Implantable Defibrillators trial, the Canadian Implantable Defibrillator Study, and the Cardiac Arrest Study Hamburg (AVID, CIDS, CASH) was 32%, 34%, and 45%, respectively.4 – 6 Thus, most patients in these trials had an EF ⬎30%. These data are even more compelling with the knowledge that the measurements of EF were made soon after resuscitation from arrest, when ventricular function is depressed.26 It seems likely that the EF before the cardiac arrest would have been higher in most cases. Thus, EF lacks useful sensitivity as a risk-stratification tool. How does EF perform with regard to specificity for prediction of sudden death? This question is difficult to answer because it requires accurate determination of mode of death (sudden versus nonsudden, with the presumption that sudden deaths are mediated by arrhythmia). Other authors have noted the potential errors when attempting to assign mechanisms to fatal events in clinical trials.27,28 It is clear that not all sudden deaths are the result of primary arrhythmic events. Nevertheless, the majority of instantaneous deaths in patients with coronary disease who do not have end-stage heart failure appear to be attributable to VTs. Were this not the case, the percentage of reduction in sudden death in ICD-treated patients would be expected to be similar to the reduction in total mortality. In fact, in the primary-prevention trials of patients with coronary disease, the percentage of reduction in sudden death markedly exceeded the reduction in total mortality in patients treated with ICDs.8,9,29 In an effort to assess the specificity of EF as a predictor of sudden death, the MUSTT investigators noted no significant difference in the percentage of deaths attributed to arrhythmia in patients whose EF was ⬍30% versus those whose EF was 30% to 40%.30 If there were a causal relationship between EF and occurrence of sudden death, then we would expect to find a significantly higher percentage of patients whose EF was ⬍30% to have deaths attributed to arrhythmia. Further evidence suggesting low specificity of EF taken in isolation for risk prediction can be obtained from examining the ATRAMI study.31 In this analysis, EF ⬍35% alone did not confer significantly increased mortality risk. Only when EF ⬍35% was combined with other factors, such as nonsustained VT or abnormal baroreflex sensitivity, were patients at significantly increased mortality risk. Another way to examine the utility of EF alone and its interaction with other factors may be seen from analysis of the MUSTT study data.30 In that analysis, total mortality was affected independently by EF as well as inducibility of VT. The total mortality of patients whose EF was ⱕ30%, regardless of the presence or absence of inducible sustained VT, was higher than that of patients whose EF was ⬎30%. Patients whose EF was ⱕ30% without inducible sustained VT, however, had a similar risk of arrhythmic death or cardiac arrest as patients with EF ⬎30% and inducible sustained VT. Thus, EF alone cannot predict the mode of death or the likelihood of responding to ICD therapy. In addition, this observation demonstrates that subgroups of patients whose EF exceeds 30% (eg, those with inducible sustained VT) may be at equal risk for sudden death as many patients whose EF is ⱕ30%. Thus, by focusing only on patients whose EF is ⱕ30%, there is the danger of missing a significant population of patients that may benefit from ICD therapy. Although EF combined with spontaneous and inducible ventricular tachyarrhythmias has been proven to identify patients at low versus higher mortality risk, a number of other less well-appreciated factors have been shown to modify risk and influence event rates observed in randomized trials. For example, studies of cardiac arrest survivors have documented that mortality is related to the site of cardiac arrest.32 Patients who experience in-hospital cardiac arrest have significantly higher mortalities than do patients experiencing out-ofhospital cardiac arrest.32 It also appears that in-hospital versus out-of-hospital location at the time of recruitment into primary prevention of sudden death trials affects mortality. In the MUSTT trial, outpatients at the time of enrollment had significantly better (by ⬇33%) survival than did those who were identified as inpatients.33 A multivariate analysis of these factors showed that EF was not associated with patient location. In contrast, outpatients were significantly younger, had multivessel coronary disease less often, had a history of heart failure less often, and had less advanced NYHA functional class. In addition, outpatients were significantly less likely to have inducible sustained VT than inpatients at the time of recruitment into the trial. The realization that sudden death and total mortality risk are influenced by numerous factors in addition to EF led the MUSTT investigators to develop a predictive model based on multiple parameters.34 Factors having the highest utility for prediction of total mortality included digitalis therapy, EF ⱕ30%, left bundle-branch block or nonspecific intraventricular conduction delay, discovery of nonsustained VT while an inpatient, and age ⬎65 years. With this model, patients whose only risk factor was EF ⱕ30% had a 2-year total mortality risk of only 6.2% and a 2-year risk for arrhythmic death or cardiac arrest of only 3.5%. The reason that the risk predicted by this model is less than one third that observed in the control arm of the MADIT-II study (19.8% total mortality at the average follow-up of 20 months)10 is because the majority of patients enrolled into the MADIT-II study had other risk Ejection Fraction and ICD Therapy Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 factors: Two thirds of patients had symptomatic heart failure (NYHA class ⱖII), almost 50% of the study patients had left bundle-branch block or a nonspecific intraventricular conduction delay on the ECG at the time of enrollment, and ⬎50% were receiving digitalis. Another example of the degree to which patient selection influenced observed mortality in the MADIT-II trial is illustrated by comparing the 2-year mortality of MADIT-II control patients (21%) with that observed in placebo-treated patients with coronary disease in the SCD-HeFT trial (19%). Because patients enrolled in the SCD-HeFT trial were required to have symptomatic heart failure their mortality would be expected to exceed that of patients enrolled in the MADIT-II study, which did not require the presence of heart failure. The fact that the observed mortality in these 2 studies is similar suggests that enrollment into MADIT-II was biased toward a group of patients with advanced illness. Thus, not all patients whose EF is ⱕ30% are at equal mortality risk. I suspect that physicians’ motivation to implant prophylactic ICDs is different for patients with a predicted 2-year mortality risk of 6% versus 20%, especially if it is taken into consideration that arrhythmic deaths account for ⬇50% the total mortality. Patients enrolled in the MUSTT trial shared a number of characteristics with those enrolled in MADIT-II: 63% had symptomatic heart failure (NYHA class II or III), one-quarter of patients had left bundle-branch block or a nonspecific intraventricular conduction delay,35 and ⬎50% were receiving digitalis. Three quarters of patients in the MUSTT study were identified as inpatients.33 The point of this analysis is that the characteristics of patients enrolled in these clinical trials profoundly influence observed outcomes, and the results may not be generalizable to all patients meeting the entry criteria specified in the protocols. If the conduct of a clinical trial inadvertently results in a study population at significantly higher risk than that of the universe of patients meeting the entry criteria specified by the protocol, then the results may have misleading implications for clinical practice. Stated another way, clinical trial design, including entry and exclusion criteria as well as protocol conduct, is influenced by a number of considerations. These considerations include the desirability of choosing a study population at high risk for developing the end point that an intervention (such as ICD therapy) seeks to modify to enhance the likelihood of obtaining a positive treatment effect. Ideally, it would be nice to be able to apply trial results directly to clinical practice. Practice guidelines must be based on objective evidence, including clinical trial results; however, common sense would dictate that practice guidelines be influenced by broader considerations, including the need to place trial results in context. In summary, EF is far from an ideal risk-stratification test on which to base prophylactic ICD therapy. Multiple factors interact with EF to influence the mortality of patients with similar degrees of left ventricular dysfunction. Thus, we need combinations of tests based on individual patient characteristics if we are to use ICD therapy most efficiently for 2541 primary prevention of sudden death. In essence, not everyone with an EF ⱕ30% should receive an ICD. Other riskstratification tools are needed in patients whose EF is ⬍30%, as well as in those having an EF ⬎30% if the number of patients likely to benefit from ICDs is to be maximized. Disclosure Dr Buxton was supported in part by grants No. UO1 HL45700 and UO1 HL45726 from the National Heart, Lung, and Blood Institute, National Institutes of Health. References 1. Zheng Z-J, Croft JB, Giles WH, Mensah GA. Sudden cardiac death in the United States, 1989 to 1998. Circulation. 2001;104:2158 –2163. 2. Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, Barker AH, Arensberg D, Baker A, Friedman L, Greene HL. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial. N Engl J Med. 1991;324:781–788. 3. Mirowski M, Reid P, Mower M. Termination of malignant ventricular arrhythmias with an implanted automatic defibrillator in human beings. N Engl J Med. 1980;303:322–324. 4. The Antiarrhythmics Versus Implantable Defibrillators (AVID) Investigators. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. N Engl J Med. 1997;337:1576 –1583. 5. Connolly S, Gent M, Roberts R, Dorian P, Roy D, Sheldon R, Mitchell L, Green M, Klein G, O’Brien B. Canadian Implantable Defibrillator Study (CIDS): a randomized trial of the implantable cardioverter defibrillator against amiodarone. Circulation. 2000;101:1297–1302. 6. Kuck K-H, Cappato R, Siebels J, Ruppel R. Randomized comparison of antiarrhythmic drug therapy with implantable defibrillators in patients resuscitated from cardiac arrest: the Cardiac Arrest Study Hamburg (CASH). Circulation. 2000;102:748 –754. 7. Connolly SJ, Hallstrom AP, Cappato R, Schron EB, Kuck K-H, Zipes DP, Greene HL, Boczor S, Domanski M, Follmann D, Gent M, Roberts RS. Meta-analysis of the implantable cardioverter defibrillator secondary prevention trials. AVID, CASH and CIDS studies. Antiarrhythmics vs Implantable Defibrillator study. Cardiac Arrest Study Hamburg . Canadian Implantable Defibrillator Study. Eur Heart J. 2000;21: 2071–2078. 8. Moss AJ, Hall WJ, Cannom DS, Daubert JP, Higgins SL, Klein H, Levine JH, Saksena S, Waldo AL, Wilber D, Brown MW, Heo M. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter Automatic Defibrillator Implantation Trial Investigators. N Engl J Med. 1996;335: 1933–1940. 9. Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G; the Multicenter Unsustained Tachycardia Trial Investigators. A randomized study of the prevention of sudden death in patients with coronary artery disease. N Engl J Med. 1999;341:1882–1890. 10. Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, Daubert JP, Higgins SL, Brown MW, Andrews ML; the Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877– 883. 11. The Multicenter Postinfarction Research Group. Risk stratification and survival after myocardial infarction. N Engl J Med. 1983;309:331–336. 12. Rouleau JL, Talajic M, Sussex B, Potvin L, Warnica W, Davies RF, Gardner M, Stewart D, Plante S, Dupuis R, Lauzon C, Ferguson J, Mikes E, Balnozan V, Savard P. Myocardial infarction patients in the 1990s—their risk factors, stratification and survival in Canada: the Canadian Assessment of Myocardial Infarction (CAMI) Study. J Am Coll Cardiol. 1996;27:1119 –1127. 13. Moss AJ, Fadl Y, Zareba W, Cannom DS, Hall WJ; the Multicenter Automatic Defibrillator Implantation Trial Research Group. Survival benefit with an implanted defibrillator in relation to mortality risk in chronic coronary heart disease. Am J Cardiol. 2001;88:516 –520. 2542 Circulation May 17, 2005 Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 14. Bansch D, Antz M, Boczor S, Volkmer M, Tebbenjohanns J, Seidl K, Block M, Gietzen F, Berger J, Kuck KH. Primary prevention of sudden cardiac death in idiopathic dilated cardiomyopathy: the Cardiomyopathy Trial (CAT). Circulation. 2002;105:1453–1458. 15. Kadish A, Dyer A, Daubert J, Quigg R, Estes NA, Anderson K, Calkins H, Hoch D, Goldberger J, Shalaby A, Sanders W, Schaechter A, Levine J; Defibrillators in Non-Ischemic Cardiomyopathy Treatment Evaluation (DEFINITE) Investigators. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med. 2004; 350:2151–2158. 16. Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, McNulty SE, ClappChanning N, Davidson-Ray LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH; Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–237. 17. de Vreede-Swagemakers JJ, Gorgels AP, Dubois-Arbouw WI, van Ree JW, Daemen MJ, Houben LG, Wellens HJ. Out-of-hospital cardiac arrest in the 1990’s: a population-based study in the Maastricht area on incidence, characteristics and survival. J Am Coll Cardiol. 1997;30: 1500 –1505. 18. Gorgels AP, Gijsbers C, de Vreede-Swagemakers J, Lousberg A, Wellens HJ. Out-of-hospital cardiac arrest-the relevance of heart failure. The Maastricht Circulatory Arrest Registry. Eur Heart J. 2003;24: 1204 –1209. 19. Misier AR, Opthof T, van Hemel NM, Vermeulen JT, de Bakker JM, Defauw JJ, van Capelle FJ, Janse MJ. Dispersion of “refractoriness” in noninfarcted myocardium of patients with ventricular tachycardia or ventricular fibrillation after myocardial infarction. Circulation. 1995;91:2566–2572. 20. Myerburg RJ, Kessler KM, Castellanos A. Sudden cardiac death: structure, function, and time-dependence of risk. Circulation. 1992;85: I2–I10. 21. Huikuri HV, Tapanainen JM, Lindgren K, Raatikainen P, Makikallio TH, Juhani Airaksinen KE, Myerburg RJ. Prediction of sudden cardiac death after myocardial infarction in the beta-blocking era. J Am Coll Cardiol. 2003;42:652– 658. 22. Wilbur D, Zareba W, Hall W, Brown M, Lin A, Andrews M, Burke M, Moss AJ. Time dependence of mortality risk and defibrillator benefit after myocardial infarction. Circulation. 2004;109:1082–1084. 23. Hohnloser SH, Connolly SJ, Kuck K-H, Dorian P, Fain E, Hampton JR, Hatala R, Pauly AC, Roberts RS, Themeles E, Gent M. The defibrillator in acute myocardial infarction trial (DINAMIT): study protocol. Am Heart J. 2000;140:735–739. 24. Hohnloser SH. DINAMIT-Defibrillator in acute myocardial infarction trial. Paper presented at: Annual Meeting of the American College of Cardiology; March 7 to 10, 2004; New Orleans, La. 25. La Rovere MT, Bigger JT Jr, Marcus FI, Mortara A, Schwartz PJ. Baroreflex sensitivity and heart rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) Investigators. Lancet. 1998; 351:478 – 484. 26. Laurent I, Monchi M, Chiche J-D, Joly L-M, Spaulding C, Bourgeois B, Cariou A, Roszeberg A, Carli P, Weber S, Dhainaut J-F. Reversible myocardial dysfunction in survivors of out-of-hospital cardiac arrest. J Am Coll Cardiol. 2002;40:2110 –2116. 27. Greene HL, Richardson DW, Barker AH, Roden DM, Capone RJ, Echt DS, Friedman LM, Gillespie MJ, Hallstrom AP, Verter J. Classification of deaths after myocardial infarction as arrhythmic or nonarrhythmic (the Cardiac Arrhythmia Pilot Study). Am J Cardiol. 1989;63:1– 6. 28. Pratt CM, Greenway PS, Schoenfeld MH, Hibben ML, Reiffel JA. Exploration of the precision of classifying sudden cardia death. Implications for the interpretation of clinical trials. Circulation. 1996;93:519 –524. 29. Greenberg H, Case RB, Moss AJ, Brown MW, Carroll ER, Andrews ML. Analysis of mortality events in the multicenter automatic defibrillator implantation trial (MADIT-II). J Am Coll Cardiol. 2004;43:1459 –1465. 30. Buxton AE, Lee KL, Hafley GE, Wyse DG, Fisher JD, Lehmann MH, Pires LA, Gold MR, Packer DL, Josephson ME, Prystowsky EN, Talajic MR; MUSTT Investigators. Relation of ejection fraction and inducible ventricular tachycardia to mode of death in patients with coronary artery disease: an analysis of patients enrolled in the multicenter unsustained tachycardia trial. Circulation. 2002;106:2466 –2472. 31. La Rovere MT, Pinna GD, Hohnloser SH, Marcus FI, Mortara A, Nohara R, Bigger JT Jr, Camm AJ, Schwartz PJ. Baroreflex sensitivity and heart rate variability in the identification of patients at risk for life-threatening arrhythmias: implications for clinical trials. Circulation. 2001;103: 2072–2077. 32. Epstein AE, Powell J, Yao Q, Ocampo C, Lancaster S, Rosenberg Y, Cannom DS, Herre JM, Greene HL. In-hospital versus out-of-hospital presentation of life-threatening ventricular arrhythmias predicts survival. Results from the AVID Registry. J Am Coll Cardiol. 1999;34:1111–1116. 33. Pires LA, Lehmann MH, Buxton AE, Hafley G, Lee KL; the Multicenter Unsustained Tachycardia Trial Investigators. Differences in inducibility and prognosis of in-hospital versus out-of-hospital identified nonsustained ventricular tachycardia in patients with coronary artery disease: clinical and trial design implications. J Am Coll Cardiol. 2001;38: 1156 –1162. 34. Buxton AE, Lee KL, Hafley GE, Prystowsky EN, Josephson ME, Fisher JD, Gold MR. A simple model using the MUSTT database can stratify total mortality and sudden death risk of coronary disease patients. J Am Coll Cardiol. 2004;43:425A. 35. Zimetbaum PJ, Buxton AE, Batsford W, Fisher JD, Hafley GE, Lee KL, O’Toole MF, Page RL, Reynolds M, Josephson ME. Electrocardiographic predictors of arrhythmic death and total mortality in the Multicenter Unsustained Tachycardia Trial. Circulation. 2004;110:766 –769. Everyone With an Ejection Fraction Less Than or Equal to 30% Should Receive an Implantable Cardioverter-Defibrillator Arthur J. Moss, MD T he automatic implantable defibrillator was introduced into clinical medicine by Mirowski et al1 in 1980, when they published their report on the life-saving benefit of the implanted defibrillator in 3 patients with recurrent episodes of ventricular tachyarrhythmias. Thereafter, there were numerous reports of effective defibrillator therapy in individual high-risk patients and in retrospective analyses of series of patients who had a defibrillator im- Ejection Fraction and ICD Therapy Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 planted because of documented episodes of hemodynamically compromising ventricular tachycardia or ventricular fibrillation. Most of these studies compared survival after defibrillator implantation with either historical controls or assumed death when the defibrillator fired. When the implantable defibrillator was first introduced, the device provided only shock therapy for fast ventricular tachyarrhythmias. Subsequent technological improvements have included transvenous leads, improved rhythm-detection algorithms, enhanced data storage, pacing capability, antitachycardia pacing features, augmented programmability, extended battery life, and reduction in the size of the implanted device. With these features, the device became known as the implantable cardioverter-defibrillator (ICD). When the preliminary 1989 report of the Cardiac Arrhythmia Suppression Trial (CAST) showed that antiarrhythmic drugs were associated with increased mortality as compared with placebo,2 it was clear that randomized ICD trials would have to be carried out. Since 1990, 10 large randomized ICD trials involving at-risk patients have been published or presented at international cardiology meetings. Seven of the trials were for primary prevention, in that the ICD was implanted to reduce mortality in patients with left ventricular dysfunction from ischemic or nonischemic cardiomyopathy. These primary prevention trials involved patients who had not yet experienced a documented life-threatening ventricular tachyarrhythmia. Three trials were for secondary prevention and involved implantation of the ICD in patients who either had survived an aborted cardiac arrest or had experienced a documented life-threatening ventricular tachyarrhythmia. Considerable data exist regarding the inverse relationship between the level of the ejection fraction (EF) and subsequent cardiac mortality.3 As the EF falls below 0.40, there is a progressive increase in the 1-year cardiac mortality rate (Figure 1). Approximately 50% of all cardiac mortality is the result of sudden death according to the 1-hour definition for sudden death. Presently, there are no reliable methods for identifying in advance those patients who are more likely to die from sudden than from nonsudden cardiac death. Thus, a reduced EF has become the major eligibility criterion for enrolling patients in primary-prevention ICD trials to reduce mortality. The question at the heart of this controversy-incardiology discussion is whether an EF ⱕ0.30 alone is sufficient to select patients who should have an ICD implanted. A few of the risk parameters frequently discussed are do patients with an EF ⱕ0.30 require additional risk stratification such as increased QRS duration, inducible ventricular tachyarrhythmias, or advanced New York Heart Association functional class? A corollary to this question is can a low-risk group of patients be identified within the low EF group with such a low mortality that the ICD is unlikely to improve survival within a reasonable time horizon? This article reviews the 10 major randomized ICD trials involving 8002 patients in which each trial had at least 90 patients per treatment arm and used all-cause mortality as the end point.4–13 The 2543 Figure 1. One-year mortality rate as a function of the EF measured at hospital discharge after MI. Reprinted with permission from N Engl J Med.3 Copyright 1983, Massachusetts Medical Society. particular focus of my presentation will be derived from randomized ICD trials in which the relative benefit of ICD therapy was evaluated in patients with EFs ⱕ0.30. The Multicenter Unsustained Tachycardia Trial (MUSTT) was not a randomized ICD trial, but rather a randomized study to determine whether electrophysiologically guided antiarrhythmic drug therapy would reduce the risk of sudden death among patients with coronary artery disease, EF ⱕ0.40 (median EF 0.30), and asymptomatic unsustained ventricular tachycardia.14 Some of the observational ICD findings in MUSTT provide useful outcome information about ICD effectiveness in patients with reduced EF, and findings from MUSTT are discussed. It is my position based on available evidence from these 10 randomized ICD trials plus MUSTT that the overwhelming majority of cardiac patients with an EF ⱕ0.30 should receive a prophylactic ICD. Randomized Trials Primary ICD Prevention Studies The design characteristics of 7 ICD primary-prevention trials are presented in Table 1, with the relative hazard ratios (HR) and the absolute ICD-related mortality reductions for ICD versus conventional therapy for each trial shown in Figures 2 and 3, respectively. Four of the trials involved only patients with ischemic heart disease, 1 study focused exclusively on patients with nonischemic cardiomyopathy, and 2 studies enrolled patients having ischemic or nonischemic cardiomyopathy. In the primary prevention trials, eligibility involved patients with an EF ⱕ0.35 in 5 trials (n⫽3907) and ⱕ0.30 in 1 trial (n⫽1232). Although there is some variability in the 2544 Circulation May 17, 2005 TABLE 1. Randomized Primary-Prevention ICD Trials Date Started; Date Published No. of Patients Eligibility Average Follow-Up, mo MADIT (ICD vs conventional treatment)4 12/27/1990; 12/27/1996 CABG Patch (ICD vs conventional treatment)5 08/14/1990; 11/27/1997 196 Previous MI, EF ⱕ0.35, NSVT, EPS⫹ 27 900 CAD, abnormal SAECG, CABG surgery MADIT-II (ICD vs. conventional treatment)9 32 07/11/1997; 03/21/2002 1232 Previous MI, EFⱕ0.30 20 COMPANION (CRT-D vs OPT)12* 01/20/2000; 05/10/2004 903 I & NICM, NYHA class III or IV, EF ⱕ0.35, QRS ⱕ0.12 s 16 DEFINITE (ICD vs conventional treatment)10 07/09/1998; 05/10/2004 458 NICM, EFⱕ0.35, NSVT or ⬎10 PVC/24 h 29 SCD-HeFT (ICD vs placebo)13† 09/16/2001; 03/08/2004 1676 I & NICM, EF ⱕ0.35 48 2000; 03/08/2004 674 Within 6–40 d of acute MI, EF ⱕ0.35, HRV (SDNN) ⱕ70 ms 30 Trial 11 DINAMIT (ICD vs conventional treatment) Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 CAD indicates coronary artery disease; CRT-D, cardiac-resynchronization therapy with pacemaker-defibrillator; EF, nonischemic cardiomyopathy; HRV, heart rate variability; NSVT, nonsustained ventricular tachycardia; OPT, optimal ventricular contraction; SAECG, signal-averaged electrocardiogram; and SDNN, standard deviation of normal heart beat *Three-arm trial (CRT-D, CRT, and OPT), but comparison in this analysis only for CRT-D vs optimal pharmacological †Three-arm trial (ICD, amiodarone, and placebo), but comparison in this analysis only for ICD vs placebo. results, the overall average HR of all 7 trials is 0.72, a value indicating a 28% reduction in the risk of death in the ICD-treated patients as compared with the conventionally treated patients (Figure 2). The absolute reduction in mortality between ICD- and conventionally treated patients also was variable among the various studies, with an overall absolute 2-year mortality reduction of 3.0 percentage points, from 17.3% in the conventionally treated patients to 14.3% in the ICD-treated patients (Figure 3). Secondary ICD Prevention Studies The design characteristics of 3 secondary-prevention trials are presented in Table 2, with the relative HRs and the absolute ICD-related mortality reductions for ICD versus conventional ther- Figure 2. HR (ICD:conventional treatment) and 95% confidence limits for mortality in 7 primary-prevention trials. The average HR for the 7 trials is 0.72 (n⫽6039). COMPANION indicates Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure trial; DEFINITE, DEFibrillators In Non-Ischemic cardiomyopathy Treatment Evaluation trial; and SCD-HeFT, Sudden Cardiac Death in Heart Failure Trial. Other abbreviations as in text. ejection fraction; I & NICM, ischemic and pharmacological therapy; PVC, premature intervals. therapy. apy for each trial shown in Figures 4 and 5, respectively. Patients enrolled in these 3 trials had documented or suspect life-threatening ventricular tachyarrhythmias, including patients who had been resuscitated from ventricular fibrillation, those with ventricular tachycardia associated with syncope or severe hemodynamic compromise, and those who experienced unmonitored syncope in whom a full workup suggested a ventricular tachyarrhythmia as the cause of the loss of consciousness. The patients in these 3 trials had mean EFs in the range of 0.31 to 0.47, values considerably higher than in the primary-prevention trials. The efficacy of ICD therapy in these 3 trials was compared against antiarrhythmic drugs (mostly amiodarone). The HR and 95% confidence intervals for all-cause mortality in each of the 3 studies for ICD-treated patients compared with those receiving antiarrhythmic drugs are presented in Figure 4. The overall average HR of 0.65 indicates a 35% reduction in the risk of death from ICD therapy. The mortality difference between ICD- and conventionally treated patients in these secondaryprevention trials showed an overall absolute 2-year mortality reduc- Figure 3. Two-year mortality rates in 7 primary-prevention ICD trials. The average 2-year mortality rates in the conventional and ICD treatment groups were 17.3% and 14.3%, respectively, with an absolute 2-year mortality reduction of 3.0 percentage points with ICD therapy. TABLE 2. Ejection Fraction and ICD Therapy 2545 Average Follow-Up, mo Reference Randomized Secondary-Prevention ICD Trials Date Started; Date Published No. of Patients AVID (ICD vs AAD) 06/01/1993; 11/27/1997 1016 Near-fatal VF, VT with syncope or hemodynamic compromise 18 6 CIDS (ICD vs amiodarone) 10/01/1990; 03/21/2000 659 Near-fatal VF, VT with syncope or hemodynamic compromise, unmonitored syncope thought to be result of VT 36 7 CASH (ICD vs amiodarone vs metoprolol) 03/01/1997 08/15/2000 288 Resuscitated from cardiac arrest secondary to sustained VT/VF 48 8 Trial Eligibility AAD indicates antiarrhythmic drugs; VF, ventricular fibrillation; and VT, ventricular tachycardia. tion of 7.5 percentage points, from 23.0% in the conventionally treated group to 15.5% in the ICD-treated patients (Figure 5). Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 Electrophysiologically Guided Drug Study (MUSTT) The primary aim of the MUSTT study was to evaluate the efficacy of electrophysiologically guided antiarrhythmic therapy. In patients who had an unsuccessful drug test, an ICD could be recommended.14 The patients who received nonrandomized ICD therapy had a significantly lower risk of cardiac arrest or death from arrhythmia than those not receiving an ICD. In a secondary analysis involving MUSTT patients who did not receive antiarrhythmic therapy, total mortality and arrhythmic deaths/cardiac arrest occurred more frequently in patients with EF ⬍0.30 than in those with an EF of 0.30 to 0.40.15 EF and ICD Efficacy There are 7 primary prevention trials with HR data for mortality in patients with EFs ⱕ0.30, and 6 primary prevention trials with relevant outcome data for EF ⬎0.30 (Figure 6). For those with EFs ⱕ0.30, the average hazard ratio was 0.71, indicating a 29% reduction in the risk of death with ICD therapy in this subgroup. This finding is in contrast to patients with EFs ⬎0.30 who had an average HR of 1.01, a value indicating no benefit from ICD therapy relative to conventional therapy in this subgroup. In the nonrandomized ICD portion of the MUSTT trial, the relative risk for death from all causes was 0.40 (P⬍0.01) for those receiving an ICD as Figure 4. HR (ICD:conventional treatment) and 95% confidence limits for mortality in 3 secondary-prevention trials. The average HR for these 3 trials is 0.65 (n⫽1963). CIDS indicates Canadian Implantable Defibrillator Study; CASH, Cardiac Arrest Study Hamburg. Other abbreviations as in text. compared with those without an ICD, but a breakdown was not provided for EF above and below 0.30.14 Regarding secondary-prevention trials, data from the Antiarrhythmics Versus Implantable Defibrillators (AVID) study are relevant.16 The AVID findings indicate that patients with an EF ⱖ0.35 have virtually the same survival with ICD therapy as with antiarrhythmic drugs. Although there are no reported data for patients with an EF ⱕ0.30, those with EFs ⬍0.20 and those with EFs in the range of 0.20 to 0.34 obtained considerable improvement in survival with the ICD. Commentary The available data indicate that ICD therapy provides a meaningful and significant reduction in mortality in high-risk patients with ischemic and nonischemic cardiomyopathy as part of primary- and secondary-prevention strategies. These populations contain considerable risk heterogeneity, with clear survival benefit in patients with EFs ⱕ0.30, but not in patients with EFs ⬎0.30. The meta-analysis findings indicate that sicker patients (ie, those with lower EFs) benefit more from ICD therapy.17 The MUSTT study indicates that those Figure 5. Two-year mortality rates in 3 secondary-prevention trials. The average 2-year mortality rates in the conventional and ICD treatment groups were 23.0% and 15.5%, respectively, with an absolute 2-year mortality reduction of 7.5 percentage points with ICD therapy. 2546 Circulation May 17, 2005 Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 Figure 6. HR (ICD:conventional treatment) and 95% confidence limits for mortality by EF. The number of patients in the DINAMIT study by EF was not available, so the DINAMIT study was excluded from computation of the average HR. A, EF ⱕ0.30 (average HR⫽0.71, n⫽4752, excluding DINAMIT). B, EF ⬎0.30 (pooled HR⫽1.01, n⫽1485, excluding DINAMIT). with an EF ⬍0.30 are at greater mortality risk than those with higher EFs,15 so it is likely that the ICD benefit in MUSTT was concentrated in those with lower EFs. Patients with ischemic or nonischemic cardiomyopathy and EF ⱕ0.30 should be considered for defibrillator implantation. It would be overly simplistic to recommend that everyone with an EF ⱕ0.30 should receive an ICD. Patients with a recent myocardial infarction or recent coronary artery bypass graft (CABG) surgery do not seem to benefit from ICD therapy, according to results from the CABG Patch trial and the Defibrillator IN Acute Myocardial Infarction Trial (DINAMIT). Such patients were excluded from eligibility in the successful trials. Patients with major noncardiac comorbidity who were not enrolled in the randomized ICD trials are not candidates for ICD therapy. Within the qualifying group of patients with EF ⱕ0.30, there are surely some low-risk patients with mortality rates so low that ICD therapy could not possibly improve outcome. For example, in unpublished analyses from the Multicenter Auto- matic Defibrillator Implantation Trial (MADIT-II), routine interrogations of the ICD revealed that 35% of patients received appropriate ICD therapy with antitachycardia pacing or shock for potentially life-threatening ventricular tachyarrhythmias within 3 years after device implantation. The question is how to identify in advance patients who will and will not require ICD therapy. To date, appropriate risk-stratification studies have not provided validated criteria for selecting or excluding patients with reduced EF for prophylactic ICD therapy. Our research group has been working on this problem, and we recently carried out a retrospective analysis of outcomes in the MADIT-II study population.18 Preliminary findings indicate 6 independent baseline risk factors associated with mortality in the conventional therapy group: age ⱖ72 years, EF ⱕ0.25, atrial fibrillation, New York Heart Association class ⱖ class III, creatinine ⱖ1.4 mg/dL, and QRS ⬎0.13 seconds. The 2-year mortality rates in those with 0, 1 to 2, and ⱖ3 of these risk factors were 3.0%, 20%, and 41%, respectively. The ICD:Conventional therapy HRs in these 3 risk groups in the total MADIT-II population were 3.2 (P⫽0.16) for 0 risk factors, 0.54 (P⬍0.01) for 1 to 2 risk factors, and 0.55 (P⬍0.01) for ⱖ3 risk factors. The low-risk group with 0 of the 6 risk factors made up 20% of the population and did not receive any benefit from ICD therapy. In fact, this low-risk group seemed to do worse with ICD therapy, although the difference was not statistically significant. Replication and validation of these findings in other at-risk populations would provide useful risk-stratification data for identifying patients who may not benefit from an ICD. An issue has surfaced regarding the use of QRS duration as a major criterion for selecting at-risk patients who should or should not receive ICD therapy. In MADIT-II, prespecified QRS durations at ⬍0.12 seconds, 0.12 to 0.15 seconds, and ⬎0.15 seconds revealed that patients with wider QRS complexes seemed to achieve a better benefit from the ICD than patients with narrower QRS complexes, although there were no significant differences in ICD efficacy among these 3 subgroups.9 The US Center for Medicare & Medicaid Services carried out a retrospective, post-hoc analysis of the MADIT-II data and reported that patients with a QRS ⬎0.12 seconds achieved a significantly greater benefit from ICD therapy than did patients with QRS ⱕ0.12 seconds.19 A metaanalysis of relevant primary prevention trials (Figure 7) reveals significant benefit with ICD therapy in patients with QRS duration ⱖ0.12 seconds (HR⫽0.70, P⫽0.01, n⫽2414), and a slightly smaller but still a significant ICD benefit in those with QRS duration ⬍0.12 seconds (HR⫽0.82, P⬍0.03, n⫽2533). These analyses indicate that QRS duration alone should not be used to select patients who should receive an ICD. Induction of ventricular tachycardia or ventricular fibrillation with programmed electrical stimulation has been used for some time in the selection of patients for ICD therapy. In general, inducibility is more useful in identifying patients for risk of ventricular tachyarrhythmias in those with wellpreserved ventricular function than in those with moderately to severely reduced ventricular function. In MADIT-II, elec- Ejection Fraction and ICD Therapy 2547 before device replacement is required. Other analyses have applied Markov model– based methods with nonverifiable assumptions that rely on speculative extrapolation of survival curves and cost patterns to encompass longer time horizons. None of the cost-effective analyses dealt exclusively with patients having an EF ⱕ0.30. Post-trial follow-up studies need to be performed to obtain a clearer picture of the lifetime costs and benefits from ICD therapy. Conclusion Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 The findings from relevant randomized defibrillator trials indicate that the ICD saves lives in a spectrum of cardiac patients with left ventricular dysfunction and an EF ⱕ0.30. Within this large population of potential ICD recipients, some patients should not receive an ICD because of co-morbid conditions. Attempts to identify low-risk patients who are unlikely to benefit from ICD therapy are in progress. At present, I recommend that ICDs be implanted in patients with an EF ⱕ0.30 unless there are specific contraindications because survival is unequivocally improved with this therapy in this patient group. References Figure 7. HR (ICD:conventional treatment) and 95% confidence limits for mortality by QRS duration. The number of patients in the DINAMIT study by QRS duration was not available, so the DINAMIT study was excluded from computation of the average HR. A, QRS ⱖ0.12 s (average HR⫽0.70, n⫽2514, excluding DINAMIT). B, QRS ⬍0.12 s (average HR⫽0.82, n⫽2535, excluding DINAMIT). trophysiological testing was carried out in 593 patients who had an ICD, and 36% of these patients were inducible into ventricular tachycardia or ventricular fibrillation. Inducibility into ventricular tachyarrhythmias was associated with greater appropriate ICD therapy for ventricular tachycardia but reduced ICD therapy for ventricular fibrillation during follow-up than patients who were not inducible. These MADIT-II findings suggest that in patients with EF ⱕ0.30, inducibility with electrophysiological testing is not clinically useful in identifying patients who should receive an ICD for the prevention of sudden cardiac death. Cost-effectiveness data have not been used in developing my position because existing studies are limited. Only a few costeffectiveness studies based on real data have been reported.20 –22 The primary, clinical trial analyses involve relatively short time horizons of only 2 to 5 years after ICD implantation— considerably shorter than the assumed 5- to 7-year longevity of the ICD 1. Mirowski M, Reid PR, Mower MM, Watkins L, Gott VL, Schauble JF, Langer A, Heilman MS, Kolenik SA, Fischell RE, Weisfeldt ML. Termination of malignant ventricular arrhythmias with an implanted automatic defibrillator in human beings. N Engl J Med. 1980;303:322–324. 2. Preliminary report: effect of encainide and flecainide on mortality in a randomized trial of arrhythmia suppression after myocardial infarction. The Cardiac Arrhythmia Suppression Trial (CAST) Investigators. N Engl J Med. 1989;321:406 – 412. 3. Risk stratification and survival after myocardial infarction. N Engl J Med. 1983;309:331–336. 4. Moss AJ, Hall WJ, Cannom DS, Daubert JP, Higgins SL, Klein H, Levine JH, Saksena S, Waldo AL, Wilber D, Brown MW, Heo M. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter Automatic Defibrillator Implantation Trial Investigators. N Engl J Med. 1996;335:1933–1940. 5. Bigger JT Jr. Prophylactic use of implanted cardiac defibrillators in patients at high risk for ventricular arrhythmias after coronary-artery bypass graft surgery. Coronary Artery Bypass Graft (CABG) Patch Trial Investigators. N Engl J Med. 1997;337:1569 –1575. 6. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. The Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. N Engl J Med. 1997;337:1576 –1583. 7. Connolly SJ, Gent M, Roberts RS, Dorian P, Roy D, Sheldon RS, Mitchell LB, Green MS, Klein GJ, O’Brien B. Canadian implantable defibrillator study (CIDS): a randomized trial of the implantable cardioverter defibrillator against amiodarone. Circulation. 2000;101:1297–1302. 8. Kuck KH, Cappato R, Siebels J, Ruppel R. Randomized comparison of antiarrhythmic drug therapy with implantable defibrillators in patients resuscitated from cardiac arrest: the Cardiac Arrest Study Hamburg (CASH). Circulation. 2000;102:748 –754. 9. Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, Daubert JP, Higgins SL, Brown MW, Andrews ML. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877– 883. 10. Kadish A, Dyer A, Daubert JP, Quigg R, Estes NA, Anderson KP, Calkins H, Hoch D, Goldberger J, Shalaby A, Sanders WE, Schaechter A, Levine JH. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med. 2004;350:2151–2158. 11. Connolly SJ, Hohnloser SH. DINAMIT: the defibrillator in acute myocardial infarction trial. Available at: http://www.medscape.com/ viewarticle/472003. Accessed April 22, 2004. 2548 Circulation May 17, 2005 Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 12. Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, Carson P, DiCarlo L, DeMets D, White BG, DeVries DW, Feldman AM. Cardiacresynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350:2140–2150. 13. Bardy G. SCD-HeFT: the Sudden Cardiac Death in Heart Failure Trial. Available at: www.sicr.org/scdheft_results_acc_lbcc.pdf. Accessed April 22, 2004. 14. Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G. A randomized study of the prevention of sudden death in patients with coronary artery disease. Multicenter Unsustained Tachycardia Trial Investigators. N Engl J Med. 1999;341:1882–1890. 15. Buxton AE, Lee KL, Hafley GE, Wyse DG, Fisher JD, Lehmann MH, Pires LA, Gold MR, Packer DL, Josephson ME, Prystowsky EN, Talajic MR. Relation of ejection fraction and inducible ventricular tachycardia to mode of death in patients with coronary artery disease: an analysis of patients enrolled in the multicenter unsustained tachycardia trial. Circulation. 2002;106:2466 –2472. 16. Domanski MJ, Sakseena S, Epstein AE, Hallstrom AP, Brodsky MA, Kim S, Lancaster S, Schron E. Relative effectiveness of the implantable cardioverterdefibrillator and antiarrhythmic drugs in patients with varying degrees of left ventricular dysfunction who have survived malignant ventricular arrhythmias. AVID Investigators. Antiarrhythmics Versus Implantable Defibrillators. J Am Coll Cardiol. 1999;34:1090–1095. 17. Moss AJ. Implantable cardioverter defibrillator therapy: the sickest patients benefit the most. Circulation. 2000;101:1638 –1640. 18. Vyas A, Moss AJ, Zareba W, Hall W, McNitt S. Risk stratification of MADIT-II patients for predicting mortality and ICD benefit. Circulation. 2004;110:III-503. 19. Centers for Medicare & Medicaid Services. National coverage analysis: implantable cardioverter defibrillators (#CAG-00157N). Tracking sheet. Available at: http://www.cms.hbs.gov/ncdr/trackingsheet.asp?id⫽39. Accessed April 22, 2004. 20. Mushlin AI, Hall WJ, Zwanziger J, Gajary E, Andrews M, Marron R, Zou KH, Moss AJ. The cost-effectiveness of automatic implantable cardiac defibrillators: results from MADIT. Multicenter Automatic Defibrillator Implantation Trial. Circulation. 1998;97:2129 –2135. 21. O’Brien BJ, Connolly SJ, Goeree R, Blackhouse G, Willan A, Yee R, Roberts RS, Gent M. Cost-effectiveness of the implantable cardioverterdefibrillator: results from the Canadian Implantable Defibrillator Study (CIDS). Circulation. 2001;103:1416 –1421. 22. Larsen G, Hallstrom A, McAnulty J, Pinski S, Olarte A, Sullivan S, Brodsky M, Powell J, Marchant C, Jennings C, Akiyama T. Cost-effectiveness of the implantable cardioverter-defibrillator versus antiarrhythmic drugs in survivors of serious ventricular tachyarrhythmias: results of the Antiarrhythmics Versus Implantable Defibrillators (AVID) economic analysis substudy. Circulation. 2002;105:2049–2057. Response to Moss Alfred E. Buxton, MD D r Moss argues that based on randomized trials, all patients, except those with standard implantable converter-defibrillator (ICD) contraindications, whose ejection fraction (EF) is ⱕ30% should be treated with an ICD. For this argument to be valid, the characteristics of patients enrolled in these trials must be representative of patients that we care for in practice, not simply those enrolled in the trial. Does the evidence support this? Except for Multicenter Automatic Defibrillator Implantation Trial-II (MADIT-II), every study cited required risk factors other than EF: Sudden Cardiac Death in Heart Failure Trial, Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure, and DEFibrillators In Non-Ischemic cardiomyopathy Treatment Evaluation (SCD-HeFT, COMPANION, and DEFINITE) required that patients have congestive heart failure. MADIT and the Multicenter Unsustained Tachycardia Trial (MUSTT) required spontaneous and inducible ventricular tachycardia. In secondary-prevention trials, ⬍50% of patients had an EF ⱕ30%. Thus, only MADIT-II required an EF ⱕ30 alone. How representative of all patients with an EF ⱕ30% is the MADIT-II population? There is evidence of significant selection bias for recruitment into that trial. Two thirds of patients enrolled had congestive heart failure.1 The highest mortality in the control group occurred in patients enrolled ⬎10 years after the most recent infarction, contrary to all of the other data (showing that highest mortality occurs within 1 year postinfarction).2 The 2-year mortality of 22% reported by MADIT-II far exceeds that observed in population-based postinfarct trials, such as Autonomic Tone and Reflexes After Myocardial Infarction (ATRAMI) (⬍10%),3 and is even higher than that observed in the control arm of the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) (14.4%).4 The problem is that these trials were designed to demonstrate that the ICD reduces mortality in selected populations; they were not designed to test how best to use the ICD. That is the task before us. References 1. Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, Daubert JP, Higgins SL, Brown MW, Andrews ML; the Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877– 883. 2. Wilbur D, Zareba W, Hall W, Brown M, Lin A, Andrews M, Burke M, Moss AJ. Time dependence of mortality risk and defibrillator benefit after myocardial infarction. Circulation. 2004;109:1082–1084. 3. La Rovere MT, Pinna GD, Hohnloser SH, Marcus FI, Mortara A, Nohara R, Bigger JT Jr, Camm AJ, Schwartz PJ. Baroreflex sensitivity and heart rate variability in the identification of patients at risk for life-threatening arrhythmias: implications for clinical trials. Circulation. 2001;103: 2072–2077. 4. Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, McNulty SE, ClappChanning N, Davidson-Ray LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH; the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–237. Ejection Fraction and ICD Therapy 2549 Response to Buxton Arthur J. Moss, MD N Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 ot everyone with a low ejection fraction benefits from an implantable cardioverter-defibrillator, but considerable evidence exists that an ejection fraction ⱕ30% identifies a meaningful proportion of patients at risk for sudden death. Buxton argues that additional risk stratifiers beyond ejection fraction ⱕ30% should be used, but which stratifiers? Electrophysiological testing and increased QRS duration do not reliably identify patients at increased risk for sudden death in this high-risk group. Buxton suggests that an ejection fraction ⱕ30% is an inadequate risk stratifier because it does not approach 100% sensitivity and specificity in the prediction of patients likely to die suddenly. Medicine is replete with examples in which good clinical practice involves overtreatment of high-risk patients to prevent serious complications. For example, because acute appendicitis cannot be diagnosed correctly 100% of the time, exploratory abdominal surgery is indicated when the diagnosis is uncertain. Finding a normal appendix a certain percentage of the time must be acceptable if the surgeon is to prevent life-threatening problems from complicating a missed acute appendicitis. Similarly, until we have more reliable tests to identify cardiac patients at risk for sudden death, it is my position that in the absence of contraindications, patients with ejection fractions ⱕ30% secondary to ischemic or nonischemic cardiomyopathy should receive an implantable cardioverter-defibrillator to improve survival and prevent sudden death. Not Everyone With an Ejection Fraction ≤30% Should Receive an ICD Alfred E. Buxton Circulation. 2005;111:2537-2549 doi: 10.1161/01.CIR.0000165057.88551.2C Downloaded from http://circ.ahajournals.org/ by guest on June 12, 2017 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2005 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/111/19/2537 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/