Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
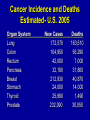
NECK MASSES: UNC MS III SURGERY • Case discussions by students • Discussion of thyroid disorders • Discussion of how to develop a differential diagnosis • Management algorithm THYROID COLIN G THOMAS, Jr. MD Professor, Department of Surgery University of North Carolina Incidence of Thyroid Disorders in Connecticut (Annual physical Examination, 1544 Patients – One Year) Simple goiter Graves’ disease Iatrogenic hyperthyroidism Hot nodule Multinodular goiter Thyroiditis Single cold nodule Hypothyroidism Cancer Total # 29 15 2 9 13 8 8 6 0 90 % 1.88 0.97 0.10 0.58 0.84 0.51 0.51 0.39 0.00 5.78 Cancer Incidence and Deaths Estimated- U.S. 2005 Organ System Lung Colon Rectum Pancreas Breast Stomach Thyroid Prostate New Cases 172,570 104,950 42,000 32,180 212,930 24,000 25,690 232,090 Deaths 163,510 56,290 7,000 31,800 40,870 14,000 1,490 30,050 Thyroid Cancer 1985 1994 New Cases 10,000 13,900 17,200 (↑ 72%) 1,120 1,200 (↑8%) Deaths 1,100 American Cancer Society 1998 1998 Evaluations of Nodular Thyroid Disease • History- symptoms, duration, familial • Physical findings, i.e. topography, firmness, surface, lymphadenopathy • Thyroid functions tests- TFT (s) - TSH Diagnostic Studies- Thyroid Cancer Fine Needle Aspiration- Establishes Cytologic Diagnosis Thyroid function tests (TSH- 1st in Thyroiditis) Technetium Scan- reflects trapping function, “hot nodule” Ultrasonography- reflects volume, composition, occult nodules Thyroid Cancer- Diagnosis • Cytology • Scans – Technetium – Radioiodine – Sestamibi – MR/CT/PET • Ultrasound • Frozen Sections • Fixed Sections Thyroid Cancers* Papillary Follicular Hürthle Medullary Anaplastic *National Cancer Data Base 31,513 patients (1985-1995) 80% 11% 3% 4% 2% Biological Characteristics • Thyrotropin Receptor– Adenylate Cyclase Systems • Iodine Trapping/Organification • Thyroglobin Production Papillary Carcinoma • Ames (Age, Distant Metastases, Extent, Size) • 89%- Low risk; Mortality 1.8% and • 11% High Risk, Mortality 46% Adjuvant Therapy Thyroxine → TSH Suppression Radiodiodine (Ablation/Rx) Thyroxine ↓ → TSH ↑ Recombinant TSH External Radiation (?) Chemotherapy (?) Neck Masses Marion Couch, MD PhD Department of OHNS University of North Carolina Some pearls: • 90% of adult neck masses are malignant • 90% of pediatric neck masses are infectious in nature • Know your anatomy then develop a differential diagnosis • Close observation • Generally, one course of a broad spectrum antibiotic is acceptable then ….. • It is never wrong to refer to a specialist for evaluation and probable biopsy • Imaging is important but tissue is everything • If you don’t get an answer with a FNA, repeat it up to three times. Consider ultrasound guided or CT guided FNA. • Never violate a neck or I will come after you. HISTORY • • • • • • • Age Duration Acute symptoms Recent travel Trauma Insect bites, pets Tobacco, alcohol, XRT CONGENITAL • Central neck: – Thyroglossal duct cysts • Pyramidal lobe of thyroid – – – – Sebaceous cysts Hemangiomas Laryngocele Ectopic thyroid • Lateral neck: – Branchial cleft cysts – Cystic hygromas – Dermoids Branchial cleft cyst Branchial cleft cysts Branchial cleft cyst Branchial cleft cyst Inflammation • Reactive lymphadenopathy • Sialoadenitis • Cervical adenitis Infectious • • • • • • • • • • Staph and strep EBV – mono TB Atypical TB HIV Cat scratch fever (Bartonella henselae) Toxoplasmosis Actinomycosis Tick-borne: Rocky Mountain Spotted Fever Lemierre’s Syndrome: septic thromb. IJV Trauma • Hematoma –Acute and expanding –Chronic and organizing • AV fistula • Pseudoaneurysm Metabolic, Idiopathic, Autoimmune • Castleman’s disease • Sarcoidosis • Kimura’s disease Neoplasms • Benign: –Lipomas –Neuromas –Fibromas –Hemangiomas –Carotid body tumors –Angiomas Neoplasms • Malignant – Thyroid – Squamous cell carcinoma (SCAA) – Lymphoma – Sarcoma – Salivary gland tumors – Metastasis: • SCCA, adenocarcinoma, undifferentiated carcinoma, melanoma Management • 1 course of broad spectrum antibiotics • Consider bloodwork and imaging • REFERAL Pearls • Avoid excisional biopsies • Use CT but consider MRI for salivary gland problems • Role of nonionizing ultrasound –Like a stethoscope? National Comprehensive Cancer Network • Use www.nccn.org for evidence-based, consensus guidelines for: – Staging – Evaluation – References – Treatment – All sites – Updated annually.