Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hospital-acquired infection wikipedia , lookup
Periodontal disease wikipedia , lookup
Rheumatic fever wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Vaccination wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Molecular mimicry wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Kawasaki disease wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Sarcocystis wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Infection control wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Ankylosing spondylitis wikipedia , lookup
Rheumatoid arthritis wikipedia , lookup
Behçet's disease wikipedia , lookup
Neuromyelitis optica wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Onchocerciasis wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Autoimmunity wikipedia , lookup
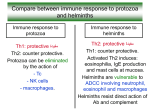
Opinion TRENDS in Parasitology Vol.19 No.10 October 2003 447 Chagas disease: a role for autoimmunity? Rick L. Tarleton Center for Tropical and Emerging Global Diseases, Department of Cellular Biology, University of Georgia, Athens, GA 30602, USA Despite many years of investigation and discussion, the cause of disease in chronic Trypanosoma cruzi infection remains a hotly debated topic. The primary point of contention is whether Chagas disease is an autoimmune disease resulting from inappropriate immune responses to self antigens that are induced and perhaps perpetuated by T. cruzi infection, or whether this disease is a result of the inability to adequately, and without significant cumulative damage, control T. cruzi infection on the part of some hosts, including the 30-40% of infected individuals who develop clinical disease. This review updates some of the data applicable to this debate with emphasis on the role of parasite persistence in Chagas disease. Several recent reviews [1– 3], including the Opinion by Girones and Fresno [4] in Trends in Parasitology, outlined many of the data supporting an autoimmune etiology for Chagas disease. These reviews pose soe questions for proponents of alternative views, which will be addressed here. But, before dealing directly with the experimental data on Chagas disease, it is instructive to consider how autoimmunity became enshrined as the causative factor in chronic T. cruzi infection. Chagas disease is the manifestation of tissue damage resulting from infection with the protozoan parasite, Trypanosoma cruzi. Despite the obvious connection between infection and disease, T. cruzi infection and Chagas disease are often considered as separate entities. The infection is usually viewed as an acute event with any resulting symptoms being a direct result of parasite invasion and the immune response to this invasion. The acute infection is normally controlled, although not cleared, and acute symptoms are alleviated by a competent host immune response. By contrast, Chagas disease is clearly uncoupled from the initial infection in time (by several decades in humans), and chronic disease symptoms are generally considered to result from different mechanisms than those that are operative in the acute infection. However, even some of the earliest and most vocal proponents of autoimmunity as the cause of Chagas disease realized that the separation of acute infection from chronic disease was probably an artificial one (see, for example, Ref. [5]). Historical perspective Autoimmunity rose to the forefront as a proposed cause of Chagas disease for one simple reason – parasites are Corresponding author: Rick L. Tarleton ([email protected]). difficult to detect at sites of the most severe pathological damage in chronically infected hosts. Observers of this fact cast about for an explanation and, as early as the 1940s, the idea of a role for ‘allergic’ mechanisms in Chagas disease was proposed (reviewed in Ref. [6]). Various technical advances helped to further explore the role of immune dysfunction in Chagas disease, resulting in the evolution of hypotheses on the mechanisms by which antiself immune responses could be generated, including polyclonal activation, molecular mimicry and bystander activation [1]. This evolution was coincident with the investigation of autoimmune diseases in general, including those linked to infectious diseases, resulting in a set of postulates by which one could attempt to assess the contribution of autoimmune responses to disease [7,8]. These developments also took place within the context of an explosion in the understanding of the immune system, the generation of diversity within it and the mechanisms that regulate host immune responses. The artificial uncoupling of T. cruzi infection from Chagas disease made it relatively easy to discount the contribution of persistent parasitic infection to disease severity in T. cruzi infection. The supposed absence of parasites at or near sites of disease is still cited as proof of a dissociation between active infection and disease, and in support of an autoimmune etiology for Chagas disease [1,9,10]. However, even ardent supporters of autoimmunity as the cause of disease in T. cruzi infection now largely concede that parasite persistence is a co-requisite, if not a prerequisite, for pathology [3,4]. This conclusion is based on the overwhelming evidence for parasite persistence in chronic T. cruzi infection and for a linkage between the sites of parasite persistence and the presence of disease in that tissue. Much of the data in support of this point, including the detection of parasite DNA, parasite protein and even intact parasites using various techniques, has been previously reviewed in detail [11,12], and additional support not included in these reviews continues to mount [13,14]. Not only is parasite persistence being nearly uniformly documented in linkage with severe disease, there is also emerging evidence in human cases and in experimental models that re-infection or continued exposure (due to continued residence in areas of active transmission) increases parasite load, in addition to disease severity [15 – 17]. Cumulatively, these data demonstrate that the initial suggestions of a disjunction between T. cruzi infection and Chagas disease was a problem of the insensitivity of http://parasites.trends.com 1471-4922/$ - see front matter q 2003 Elsevier Ltd. All rights reserved. doi:10.1016/j.pt.2003.08.008 448 Opinion TRENDS in Parasitology techniques, rather than a true absence of parasites at sites of disease in chagasic patients. Given this conclusion, it is interesting to consider whether or not Chagas disease would ever have been considered an autoimmune disease if these more sensitive techniques had been available to some of the early investigators of chronic Chagas disease. However, despite the general agreement that parasite persistence is a crucial causative factor in chronic Chagas disease, autoimmunity still has strong advocates, as recent reviews document [1– 4]. Among the questions posed by these reviews are: (1) why do lesions develop primarily in the heart and not at other sites of parasite persistence? (2) why does parasite burden not always correlate with disease severity? and (3) how does one exclude the possibility that autoimmune pathogenesis is fundamental to Chagas disease? The heart of the matter? Whereas it is true that Chagas disease is a clinical syndrome primarily involving the heart, other tissues are affected as well. The most studied other site for human disease is the gut and it was appreciated very early in the discovery of the parasite and the description of Chagas disease that gut pathology occurred in a variable, but significant proportion (generally estimated at , 10%) of infected individuals [18]. The timing of occurrence (i.e. decades after the initial infection), the type of tissue affected (e.g. muscle) and the type of damage (inflammation, scaring, loss of nervous function and elasticity) are all similar to what is observed in the heart. These similarities strongly suggest a common etiology. In experimental hosts, disease is also evident in the skeletal muscle, again with the same characteristics of delayed onset, inflammation and loss of muscle function. Skeletal muscle disease also exists, but is less well documented, in human infections [19,20]. Persistence of T. cruzi has been documented in several other sites, including the bladder [21], adrenal gland [22,23], skin [24] and central nervous system [25]. Thus, parasite persistence in the heart and at other sites of disease in chronic T. cruzi infection is firmly established. Perhaps, rather than asking why the heart is the only tissue affected in Chagas disease, we should question why disease is primarily focused in muscle tissue. If disease is similar in these various muscle sites, how does this mesh with the idea of cardiac-based autoimmunity? The answer to the first question is that muscle appears to be one of the main tissues where T. cruzi has the ability to persist for decades. The tissue specificity of disease in different hosts correlates well with parasite persistence in those tissues. For example, in different mouse models of the chronic disease, the persistence of parasites in skeletal muscle correlates with disease development in that tissue, whereas persistence in heart is linked to inflammatory disease there [26]. In humans, the link between tissuespecific persistence of T. cruzi and clinical disease is demonstrated by: (1) the detection of parasite DNA in the hearts, but not in the esophageal tissue, of individuals with cardiac disease; and (2) the detection of parasite DNA in the esophageal tissue, but not the hearts, of those with esophageal disease [27,28]. http://parasites.trends.com Vol.19 No.10 October 2003 Parasite burden and disease The lack of a direct quantitative correlation between parasites and parasite components and sites of disease is often cited as supporting autoimmunity as the cause of Chagas disease [1,3,4,10]. For example, Palomino et al. [10] report the presence of parasite antigens in 12 out of 12, and parasite-filled pseudocysts in 9 out of 12 chagasic hearts submitted to extensive immunohistochemical analysis. However, this investigation did not document a quantitative link between parasite antigen and tissuespecific lesions, prompting the authors to conclude that autoimmunity must be at work in the development of these lesions. These are difficult experiments, and Palomino et al. are to be commended for the exhaustive and high quality analysis of the tissues. However, like earlier investigations that failed to detect T. cruzi in chagasic hearts, these types of studies are also limited by available techniques. Immunohistochemistry cannot provide quantitative data easily and it is not possible to know the evolutionary history of a lesion from the ‘snapshot’ of that process provided by tissue sections. An equally (if not more) plausible conclusion from these studies is that some lesions are more active, more recent, or maybe even just happened to be sectioned through areas of current or recent infection (and thus have intact parasites or parasite antigen associated with them), whereas other lesions lack parasites or parasite antigens because of the effective clearance of parasites from this site, or because of the angle or depth of the section. If the presence or absence of parasites is not responsible for the focal nature of lesions in Chagas disease, then what is? What is distinctive about cardiomyocytes in one area of the heart that makes them susceptible to autoimmune damage, whereas adjacent cells are resistant? Until technical advances provide the means to follow the evolution of a lesion over time, it is difficult to determine exactly how lesions arrive at the point that one observes in histological sections. Another set of data that addresses the issues of parasite levels and disease severity comes from studies of the effect of drug treatment during the chronic phase of infection on the progression of disease. Viotti et al.’s studies on the effectiveness of chemotherapeutic treatment in reducing the incidence of disease progression in long-term follow-up studies are seminal [29]. These studies have been extended to a larger group of patients with similar results (R. Viotti et al., unpublished). The most remarkable study is that by Apt et al., who conducted a nine-year follow-up study on 299 chronically infected patients treated with either itraconazole or allopurinol during the chronic stages of infection [30]. These authors reported that the frequency of new electrocardiogram (ECG) abnormalities was significantly lower in the itraconazole-treated group when compared with that in the untreated group and that 50% of the patients who exhibited ECG abnormalities before treatment became electrocardiographically normal during the follow-up. These results suggest that disease can be arrested and even reversed with aggressive treatment to reduce the parasite burden. Unfortunately, not all studies have yielded such encouraging results (for review, see Ref. [31]). In addition to problems of experimental design, low numbers of Opinion TRENDS in Parasitology individuals in the study groups and short follow-up periods, the poor efficacy of existing drugs in reducing parasite load contributes to the variable results in longterm follow-up studies. For example, Braga et al. found no difference with respect to numbers of circulating parasites detected by PCR between patients treated during the chronic stage of the infection and those left untreated [32]. In cases where chemotherapy fails to alter the prevalence of infection or the parasite load in a group of chronically infected individuals, there is likewise a failure to achieve an improvement in the clinical picture following this treatment [33]. Alternatively, therapies that are effective in reducing or eliminating T. cruzi infection in chronic patients result in significant improvements in clinical status [30] (R. Viotti et al., unpublished). Apt et al. and Viotti et al.’s studies also substantiate the conclusion that individuals who become spontaneously seronegative without treatment (presumably self-cured) also do not show progression toward severe disease. In addition to parasite load and location being tightly linked to disease severity and its location, there is evidence that Chagas disease is not self-perpetuating and does not occur in the absence of infection [26,34]. Thus, Chagas disease fails to meet the most crucial criteria for being considered an autoimmune disease [8]. A substantial body of work shows that Chagas disease progresses in the presence of higher parasite burden and is reduced when parasite burden is reduced. Although a uniformly effective treatment does not exist yet, it is encouraging that therapies capable of reducing parasite burden have an excellent chance of reducing disease development or preventing progression of clinical disease, irrespective of the presence of possible autoimmune responses. If not autoimmunity, then what is it? There seems little doubt that anti-self responses exist in T. cruzi infection. This should not be surprising, considering that all individuals have autoreactive T cells and B cells that can be activated under the appropriate set of circumstances. All chronic infections provide these circumstances, for example, a pro-inflammatory milieu, tissue damage and the release of cryptic epitopes enhanced antigen presentation as a result of upregulation of co-stimulatory molecules, all of which are associated with persistence of a pathogen. What is it about Chagas disease that distinguishes it from other persistent infections and turns it into an autoimmune disease? Some propose that it is the target(s) of the autoimmune responses that the makes T. cruzi infection different. Indeed, several potentially mimicked antigens have been described in T. cruzi – ‘perhaps too many’ in the estimation of Girones and Fresno [4]. Some limited data have suggested that the responses to the mimicked antigens can be pathogenic [35 – 38]. Others suggest that polyclonal activation is the key in T. cruzi-induced autoimmunity [39]. However, in sum, the evidence supporting either molecular mimicry or polyclonal activation directly in the pathogenesis of T. cruzi infection is sparse. With respect to mimicry, it is clear that T. cruzi infection meets only one of http://parasites.trends.com Vol.19 No.10 October 2003 449 the five criteria deemed necessary to call this an autoimmune disease (see those outlined in Ref. [8]). If Chagas disease is not caused by autoimmune reactivity, then why does it occur and how does one account for the latency and spectral nature of the disease, characteristics normally associated with autoimmune diseases. More importantly with respect to treatment and prevention, why do a subset of T. cruzi-infected individuals develop disease, whereas the majority do not? Two interacting factors are associated with the development (or not) of severe disease: (1) parasite burden; and (2) the effectiveness of the host immune response in controlling parasites in specific tissues. The link between parasite burden and disease has been reviewed in depth above. Parasite burden is, in turn, largely dependent on how effective the host immune response is in killing parasites or limiting parasite replication. Variations in the parasite strain(s) infecting an individual help determine parasite burden, but so too does the effectiveness of the immune response, which is highly variable between individuals. When immune control is inefficient, parasite load and inflammation, and thus the potential for tissue damage, increases. Increased inflammation with poor immune control might seem counterintuitive. But, the immune system is generally self-regulating – a wellexecuted response that achieves clearance (or perhaps more often, ‘near’ clearance) of a pathogen results in less tissue damage than does an ineffective response that allows for persistence of the pathogen in greater numbers. The evidence that the quality of the immune response to T. cruzi correlates with disease severity comes from several types of studies. First, the effect of immunosuppression or of genetic deficiencies in the immune response on disease severity is well documented in humans and in animal models with T. cruzi infection [11,12,40]. In all cases, the compromise of one or more of the immune mechanisms that are known to be important in the control of T. cruzi infection results in increased parasite load and increased incidence of chronic-stage disease. This is most clearly seen in humans with respect to co-infection with HIV [40]. Second, treatments that boost immune responses decrease the severity of disease. Prophylactic vaccination of mice with genes of the T. cruzi transsialidase family results in substantially less chronic-stage disease [41]. Third, there are emerging (although still limited) data from immunological studies in animal models and in humans that support a link between the strength and nature of the antiparasite response and the severity of chronic stage disease. For example, Laucella et al. have found a higher frequency of T. cruzispecific interferon g (IFN-g)-producing memory T cells in individuals without clinical symptoms when compared with those with severe disease (S. Laucella et al., unpublished). In addition, there continue to be reports of infected individuals who become seronegative over time (i.e. they appear to cure spontaneously, almost certainly as a result of a particularly effective immune response). None of these individuals exhibit progressive disease following conversion to seronegative [29,42] (R. Viotti et al. unpublished), which argues strongly in favor of the participation of an effective antiparasite response in preventing disease 450 Opinion Chagasic TRENDS in Parasitology Asymptomatic (a) Vol.19 No.10 October 2003 development. If autoimmunity was important in disease, then an occasional previously infected seronegative would be expected to have progressive disease. Perspective The controversy over the etiology of Chagas disease will continue for some time. There are no data that can absolutely rule out autoimmunity as having any role in disease development, and the support for autoimmunity as a primary cause of pathology in this, or for any other infectious disease, is far from definitive [8]. One area of agreement that has emerged in recent years is that parasite persistence is required for disease. However, the evolution of disease as a result of this persistence is still unclear. Girones and Fresno propose that a ‘trigger’ might be required to initiate the disease process, although the nature of this trigger is still unclear [4]. Figure 1 illustrates how disease might occur in the absence of autoimmunity, highlighting the ability of a competent immune response to limit parasite load and thus tissue damage (see animation of this process on: http://tango. ctegd.uga.edu/chagas.htm). Further studies and better tools are needed to test the validity of the mechanism illustrated in Fig. 1. Whatever the mechanism for disease, one goal seems clear: patients will benefit from a reduced parasite burden. This cannot be achieved by targeting autoimmunity as the problem in Chagas disease. Global suppression of immune responses in chagasic patients is out of the question, and suppression of responses to one or more of the proposed autoantigens is also problematic (J.S. Leon and D.M. Engman, unpublished). A reduction in parasite burden can be achieved not only through the discovery of better chemotherapeutics, but also with the use of immunologicals, potentially including therapeutic vaccines, to enhance host immune control of the infection. Effective chemotherapy could enhance anti-T. cruzi immunity [43]. Driving the immune response toward an appropriate, efficient control of the parasite burden – something that happens in the majority of individuals – is an approach which has not until now been pursued with sufficient vigor. (b) (c) (d) Acknowledgements TRENDS in Parasitology Fig. 1. Proposed model for lesion progression in symptomatic (chagasic) and asymptomatic Trypanosoma cruzi infection. (a) Lesions originate from a single infected cell. (b) Parasites (indicated in brown) released from infected cells invade adjacent cells or circulate to other sites. Immune recognition results in inflammation (lymphocytes indicated in blue), which regulates the spread of parasites to varying degrees in different patients, depending on the quality (i.e. type and intensity) of the immune response. (c) Tissue destruction occurs as a result of parasite destruction, killing of infected cells by immune effectors (represented by blue cells), and peripheral damage to noninfected cells. Efficient immune control results in less tissue damage in asymptomatic patients. (d) When immune control is not efficient, the lesion size increases and fibrosis is extensive (chagasic). By contrast, efficient control of parasite replication results in less tissue damage and a selfhealing lesion (asymptomatic). For an animated version of this process, go to: http://tango.ctegd.uga.edu/chagas.htm http://parasites.trends.com Thanks to David Engman and Rodolfo Viotti for sharing data from unpublished works, and to the past and present members of the Tarleton laboratory for their contributions to the data and ideas expressed in this review. R.L.T.’s laboratory is supported by grants from the National Institutes of Health. R.L.T. is a Burroughs Wellcome Fund Scholar in Molecular Parasitology. References 1 Engman, D.M. and Leon, J.S. (2002) Pathogenesis of Chagas heart disease: role of autoimmunity. Acta Trop. 81, 123 – 132 2 Leon, J.S. and Engman, D.M. (2001) Autoimmunity in Chagas heart disease. Int. J. Parasitol. 31, 555– 561 3 Soares, M.B. et al. (2001) The pathogenesis of Chagas’ disease: when autoimmune and parasite-specific immune responses meet. An. Acad. Bras. Cienc. 73, 547 – 559 4 Girones, N. and Fresno, M. (2003) Etiology of Chagas disease myocarditis: autoimmunity, parasite persistence, or both? Trends Parasitol. 19, 19 – 22 5 Takle, G.B. and Hudson, L. (1989) Autoimmunity and Chagas’ disease. Curr. Top. Microbiol. Immunol. 145, 79 – 92 Opinion TRENDS in Parasitology 6 Brener, Z. (1980) Immunity to Trypanosoma cruzi. Adv. Parasitol. 18, 247 – 292 7 Rose, N.R. and Bona, C. (1993) Defining criteria for autoimmune diseases (Witebsky’s postulates revisited). Immunol. Today 14, 426 – 430 8 Benoist, C. and Mathis, D. (2001) Autoimmunity provoked by infection: how good is the case for T cell epitope mimicry? Nat. Immunol. 2, 797 – 801 9 Caliari, M.V. et al. (2002) Quantitative analysis of cardiac lesions in chronic canine chagasic cardiomyopathy. Rev. Inst. Med. Trop. Sao Paulo 44, 273– 278 10 Palomino, S.A. et al. (2000) Systematic mapping of hearts from chronic chagasic patients: the association between the occurrence of histopathological lesions and Trypanosoma cruzi antigens. Ann. Trop. Med. Parasitol. 94, 571 – 579 11 Tarleton, R.L. (2003) Trypanosoma cruzi and Chagas disease: cause and effect. In World Class Parasites: American Trypanosomiasis (Vol. 7) (Tyler, K.M. and Miles, M.A., eds), pp. 107– 116, Kluwer Academic Publishers 12 Tarleton, R.L. (2001) Parasite persistence in the aetiology of Chagas disease. Int. J. Parasitol. 31, 550 – 554 13 Guarner, J. et al. (2001) Mouse model for Chagas disease: immunohistochemical distribution of different stages of Trypanosoma cruzi in tissues throughout infection. Am. J. Trop. Med. Hyg. 65, 152 – 158 14 Monteon-Padilla, V. et al. (2001) Persistence of Trypanosoma cruzi in chronic chagasic cardiopathy patients. Arch. Med. Res. 32, 39 – 43 15 Bustamante, J.M. et al. (2003) Indeterminate Chagas’ disease: Trypanosoma cruzi strain and re-infection are factors involved in the progression of cardiopathy. Clin. Sci. (Lond.) 104, 415 – 420 16 Bustamante, J.M. et al. (2002) Trypanosoma cruzi reinfections in mice determine the severity of cardiac damage. Int. J. Parasitol. 32, 889 – 896 17 Storino, R. et al. (2002) Chagasic cardiopathy in endemic area versus sporadically infected patients. Rev. Saude Publica 36, 755– 758 18 Guerra, F. (1970) American trypanosomiasis. An historical and a human lesson. J. Trop. Med. Hyg. 73, 105 – 118 19 Laguens, R.P. et al. (1975) Immunopathologic and morphologic studies of skeletal muscle in Chagas’ disease. Am. J. Pathol. 80, 153 – 162 20 Sanz, O.P. et al. (1978) An electrophysiological investigation of skeletal muscle in human chronic Chagas’ disease. Arq. Neuropsiquiatr. 36, 319 – 326 21 Buckner, F.S. et al. (1999) Detection of live Trypanosoma cruzi in tissues of infected mice by using histochemical stain for betagalactosidase. Infect. Immun. 67, 403 – 409 22 Rodrigues, D. et al. (2002) Pathologic findings in the adrenal glands of autopsied patients with acquired immunodeficiency syndrome. Pathol. Res. Pract. 198, 25– 30 23 Teixeira Vde, P. et al. (1997) Correlation between adrenal central vein parasitism and heart fibrosis in chronic chagasic myocarditis. Am. J. Trop. Med. Hyg. 56, 177 – 180 24 La Forgia, M.P. et al. (2003) Cutaneous manifestation of reactivation of Chagas disease in a renal transplant patient: long-term follow-up. Arch. Dermatol. 139, 104 – 105 25 Silva, N. et al. (1999) Trypanosoma cruzi meningoencephalitis in HIVinfected patients. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol. 20, 342 – 349 Vol.19 No.10 October 2003 451 26 Zhang, L. and Tarleton, R.L. (1999) Parasite persistence correlates with disease severity and localization in chronic Chagas’ disease. J. Infect. Dis. 180, 480– 486 27 Jones, E.M. et al. (1993) Amplification of a Trypanosoma cruzi DNA sequence from inflammatory lesions in human chagasic cardiomyopathy. Am. J. Trop. Med. Hyg. 48, 348 – 357 28 Vago, A.R. et al. (1996) PCR detection of Trypanosoma cruzi DNA in oesophageal tissues of patients with chronic digestive Chagas’ disease. Lancet 348, 891 – 892 29 Viotti, R. et al. (1994) Treatment of chronic Chagas’ disease with benznidazole: clinical and serologic evolution of patients with longterm follow-up. Am. Heart J. 127, 151 – 162 30 Apt, W. et al. (2003) Itraconazole or allopurinol in the treatment of chronic American trypanosomiasis: the regression and prevention of electrocardiographic abnormalities during 9 years of follow-up. Ann. Trop. Med. Parasitol. 97, 23 – 29 31 Coura, J.R. and de Castro, S.L. (2002) A critical review on Chagas disease chemotherapy. Mem. Inst. Oswaldo Cruz 97, 3 – 24 32 Braga, M.S. et al. (2000) Persistent infections in chronic Chagas’ disease patients treated with anti-Trypanosoma cruzi nitroderivatives. Rev. Inst. Med. Trop. Sao Paulo 42, 157– 161 33 Lauria-Pires, L. et al. (2000) Progressive chronic Chagas heart disease ten years after treatment with anti-Trypanosoma cruzi nitroderivatives. Am. J. Trop. Med. Hyg. 63, 111 – 118 34 Tarleton, R.L. et al. (1997) Autoimmune rejection of neonatal heart transplants in experimental Chagas’ disease is a parasite-specific response to infected host tissue. Proc. Natl. Acad. Sci. U. S. A. 94, 3932– 3937 35 Girones, N. et al. (2001) Dominant T- and B-cell epitopes in an autoantigen linked to Chagas’ disease. J. Clin. Invest. 107, 985– 993 36 Leon, J.S. et al. (2001) Cardiac myosin autoimmunity in acute Chagas’ heart disease. Infect. Immun. 69, 5643– 5649 37 Pontes-de-Carvalho, L. et al. (2002) Experimental chronic Chagas’ disease myocarditis is an autoimmune disease preventable by induction of immunological tolerance to myocardial antigens. J. Autoimmun. 18, 131 – 138 38 Cunha-Neto, E. et al. (1995) Autoimmunity in Chagas disease cardiopathy: biological relevance of a cardiac myosin-specific epitope crossreactive to an immunodominant Trypanosoma cruzi antigen. Proc. Natl. Acad. Sci. U. S. A. 92, 3541– 3545 39 Reina-San-Mart, N.B. et al. (2000) Lymphocyte polyclonal activation: a pitfall for vaccine design against infectious agents. Parasitol. Today 16, 62 – 67 40 Ferreira, M.S. and Borges, A.S. (2002) Some aspects of protozoan infections in immunocompromised patients – a review. Mem. Inst. Oswaldo Cruz 97, 443 – 457 41 Garg, N. and Tarleton, R.L. (2002) Genetic immunization elicits antigen-specific protective immune responses and decreases disease severity in Trypanosoma cruzi infection. Infect. Immun. 70, 5547– 5555 42 Arribada, A. et al. (1986) A four year follow up survey of chagasic cardiopathy in Chile. Bull. Pan Am. Health Organ. 20, 254 – 266 43 Olivieri, B.P. et al. (2002) Benznidazole treatment following acute Trypanosoma cruzi infection triggers CD8(þ) T-cell expansion and promotes resistance to reinfection. Antimicrob. Agents Chemother. 46, 3790– 3796 Articles of interest in other journals Dobson, C.B. et al. (2003) Do infectious agents play a role in dementia? Trends Microbiol. 11, 312–317 Agbo, E.C. et al. (2003) Trypanosoma brucei genomics and the challenge of identifying drug and vaccine targets. Trends Microbiol. 11, 322–329 Festing, M.F.W. (2003) Principles: The need for better experimental design. Trends Pharmacol. Sci. 24, 341–345 Segal, S and Hill, A.V.S. (2003) Genetic susceptibility to infectious disease. Trends Microbiol. 10.1016/S0966-842X(03)00207-5 White, R.J. et al. (2003) Targeting metalloenzymes: a strategy that works. Curr. Opin. Pharmacol. 10.1016/S1471-4892(03)00115-2 http://parasites.trends.com