Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
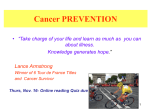
Studying Help-Seeking for Testicular Cancer: Some Lessons from the Literature (Part 2) OLIVER J. MASON University College, London KATE STRAUSS Kidderminster Hospital Worcestershire, United Kingdom When patients delay seeking medical attention after noticing symptoms of cancer there may be consequences in terms of the eventual staging of the disease at diagnosis, its prognosis and their survival. This review focuses on the psychosocial factors influencing help-seeking behaviour, hoping to draw lessons for testicular cancer in particular. Although the majority of studies have focussed on breast cancer, there is increased attention on other cancers including testicular cancer. This review outlines the methodology and terminology of “patient delay” and some of its consequences, before considering the range of influences of potential relevance to testicular cancer from a wide range of studies. It makes specific recommendations concerning the measurement of delay and methodology generally. Both psychological factors such as symptom interpretation, denial, avoidance, and distress as well as social factors are highlighted when studying the process by which men come to consult physicians. Keywords: men, help-seeking behaviour, testicular cancer, patient delay, physicians A lthough commonly considered a single disease, cancer is a term that is used to describe more than two hundred different diseases (Nezu, Nezu, Friedman, Faddis, & Houts, 1998). The most common cancers in men are lung and skin cancers (accounting for more than a third of the cases), and in women breast and skin cancers account for a similar proportion of cases (Rees, Goodman, & Bullimore, 1993). Rees et al. (1993) state that over their lifespan approximately three out of 10 people Correspondence concerning this article should be sent to Oliver Mason, Sub-department of Clinical Health Psychology, University College London, London, England WC1N 3BG. Electronic mail: [email protected]. International Journal of Men's Health, Vol. 3, No. 2, Summer 2004, 111-127. © 2004 by the Men's Studies Press, LLC. All rights reserved. 111 MASON and STRAUSS will develop cancer and two thirds of these will die as a result of the disease (or one in five of the population). It is a disease that generally affects an older age group with 75% of cancers registered in people over the age of 60. Although these aspects inform lay perceptions of cancer in general, testicular cancer does not fit the “general picture,” occurring as it does in younger men with a high survival rate when treated appropriately. However, one should note the significant gap between men’s and women’s attendance at health centres, with men attending less often (Watson, 2000), and that men suffer increased mortality. The Department of Health and Human Services (Courtenay, 2000) noted that in the United States men’s death rates for cancer are one and a half times greater than for women. These two factors have led to the common adage in health literature that “women are sicker, but men die quicker” (Lahelma, Martikainen, Rahkonen, & Silventoinen, 1999, p. 7). The United Kingdom census (Quinn, Babb, Brock, Kirby, & Jones, 2001) identified around 1,400 cases of testicular cancer in 1997, forming just over 1% of all male cancer. Incidence was highest (13 per 100,000) in 30-34 year olds, and more than half of all cases were under 35. It appears that the incidence of testicular cancer is increasing in the western world (Chilvers, Saunders, Bliss, Nicholls, & Horwich, 1989; Dearnaley, Huddart, & Horwich, 2001). However, the prognosis for testicular cancer has steadily improved, and it is estimated (Gascoigne & Whitear, 1999) that deaths in England and Wales fell by 40% between the late 1970s and 1980s. This is probably due to improved detection and treatment, the introduction of serum markers, and the use of chemotherapy since the mid-1970s. However, one review of epidemiological and histological evidence across several regions in Europe and Asia (Forman & Moller, 1994) suggested that both the increase and variability in incidence point to environmental influences such as environmental estrogenic compounds. Although the cause of testicular cancer is unknown, intra-organismic suggestions include genetic factors, undescended testicles, and infantile hernia (Dearnaley et al., 2001). Several decades of cancer research have focused on what have become known as “patient delay” and the factors involved in the time between first noticing symptoms and first seeking medical help. Why study patient delay in cancer, and testicular cancer in particular? When diagnosed before invasion beyond the testicular tissues, there is a five-year survival rate of more than 95% (Wardle et al., 1994). However, this study also found that 50% of cases present once spreading has occurred and that this is associated with a lower survival rate. Consonant with this, Rosella (1994) relates the fact that half of men present for medical attention and are diagnosed once the disease has spread further than the testicles, epididymis, and spermatic cord due to “delay behaviour” and to the “extremely rapid growth of testicular tumours” (p. 667). Though possibly not representative of other countries, one Turkish study (Toklu, Ozen, Sahin, Rastadoskouee, & Erdem, 1999) found total delay averaged 23 weeks. Half of the 145 patients presented with scrotal pain, but neither this nor diagnostic delay, income, or education was associated with staging.1 Factors affecting delay include not only medical but also psychological and social influences such as personality, attitudes to health and the body, gender, and race. We examine the concept of patient delay and the results of a wide range of 112 STUDYING HELP-SEEKING studies of psychosocial factors so as to highlight implications for the study of testicular cancer. PATIENT DELAY The concept of delay has long been considered an important issue in oncology and is most often divided into two categories: “patient delay” and “provider delay” (AbdelFattah et al., 1999; Burgess, Ramirez, Richards, & Love, 1998; Caplan & Helzlsouer, 1992). A third subcategory of “provider delay” has also been defined as delay following referral to hospital (Carter & Winslet, 1998) and may be further separated into primary care delay and secondary care delay. This paper is concerned with the first issue, namely the time taken from the first detection of symptoms by the patient to the point at which medical help is sought. “Patient delay” is the common terminology used in the literature to describe this phenomenon. However, Worden and Weisman (1975) argued that the concept of delay has a tendency to assign blame and negligence to the patient and that in so doing there is a danger that the complexities involved in the process (including the characteristics of differing cancers and psychosocial factors) are not given proper significance and understanding. They argued for the term delay to be replaced by the less loaded term of “lag time.” Despite the publication of this article 25 years ago, patient delay remains the terminology most used, and so we have retained it despite its weaknesses. As well as implying negligence by patients, the term delay also implies an imposed boundary below which is an “acceptable” time limit for seeking help and above which it is “unacceptable.” Clearly the definition and measurement of delay are critical to any conclusions that can be drawn. DEFINING AND MEASURING DELAY The majority of studies have determined patient delay as the time between first noticing symptoms and first face-to-face consultation with a medical professional (Burgess et al., 1998; Mansson et al., 1993; Nosarti et al., 2000; Styra, Sakinofsky, Mahoney, Colapinto, & Currie, 1993). These studies therefore include in their estimates of patient delay not only the time taken by patients to seek medical attention, but also the time period between first contact of the healthcare system (the arrangement of an appointment) to first face-to-face contact (actual consultation). However, any delay between the arrangement of an appointment and first consultation is better considered as system delay and confounds estimates of true patient delay when waitlist times are variable. A minority of other studies have defined delay as the time between first noticing symptoms and first contact with the healthcare system (Lauver, Coyle, & Panchmatia, 1995; Lauver & Tak, 1995), thereby excluding any time period between first contact and first consultation. Clearly a model of how delay arises is useful in studying what is undoubtedly not a unitary phenomenon. Andersen and colleagues’ model of total patient delay (Andersen & Cacioppo, 1995) attempts to describe several stages of the prediagnostic period of general application to a variety of physical disorders (see Figure 1). Each stage is dichotomous, and a move to the next stage is determined by decisions and interpretations in the previous 113 MASON and STRAUSS stage. The period following detection of an unexplained symptom but before inference of illness is called appraisal delay. The second period of illness delay involves making a choice between seeking medical attention and self-treating the illness. When the person realizes the symptom does not disappear spontaneously and decides to seek medical help, he moves into a phase of behavioral delay that concludes when he makes an appointment. Finally, scheduling delay occurs when the appointment does not follow soon after its arrangement. This may be due to the medical specialist (when it is impossible to make an appointment within a certain time) or to the patient (when it takes a while before a convenient time for the patient occurs). Andersen and Cacioppo (1995) found that the delay intervals were independent of one another and that appraisal delay constituted at least 60% of the total for women with breast cancer or gynecological tumors. Detects unexplained sign(s) and/or symptom(s) Yes Appraisal Delay Infers illness No Yes No Decides to seek Medical attention No Acts on decision by making an appointment No First receives medical attention Figure 1. Andersen et al.’s model of patient delay. 114 Illness Delay Yes Behavioural Delay Yes Scheduling Delay Yes STUDYING HELP-SEEKING In some studies delay has been considered a continuous variable (usually in days) without an explicit cut-off point between participants considered as “delayers” or “nondelayers.” While others use a cut-off to separate discrete groups of “delayers” and “nondelayers,” there seems to be little consensus within the literature as to what constitutes delay. The definitions of delay used by different studies ranged between a time period of one week or more (Colbert, 1994) to six months or more (Styra et al., 1993). Despite the lack of any real consensus on this issue, many authors consider three months as the rule of thumb for the definition of a lengthy delay period that at least facilitates comparison. Mor, Masterson-Allen, Goldberg, Guadagnoli, and Wool (1990) studied three different kinds of cancer patients— newly diagnosed lung, breast, and colorectal patients. Their rationale for a threemonth cut-off point was based on two older papers: Pack and Gallo (1938) seem to have set a standard for this type of research by defining delay as a wait by the patient of three months and over. Antonovsky and Hartman (1974), in their review on delay and the detection of cancer, argued that three months was reasonable given their conclusion that 35-50% of cancer patients wait more than three months before seeking help. These arguments for a three-month cut-off point have been used in other recent studies of breast cancer (Burgess, Ramirez, Richards, & Love, 1998; Burgess, Ramirez, Smith, & Richards, 2000; Faccione & Dodd, 1995). Burgess et al. (2000) based their rationale on an argument that previous studies have shown that approximately one-fifth of women had waited for three months or more prior to seeking help. However, it is not clear whether this or other cut-off points would be appropriate for testicular cancer, and at least initially we would recommend treating delay as a continuous variable with no absolute time limit applied. A further issue arises when studies include individuals who have self-discovered symptoms alongside those who have had symptoms recognised through other means. Faccione and Dodd (1995) in their study on women’s help-seeking narratives for breast cancer included not only women who had self-discovered symptoms but also women who had symptoms discovered through routine mammographies and breast examinations by physicians. Quantitative studies also tend to confound these pathways to healthcare: Keinan, Carmil, and Reick’s (1991) sample of 62 women seeking medical attention for potential breast cancer included 10 who had their lump discovered by a doctor during a routine checkup. As currently there is no routine screening for testicular cancer, self-discovery constitutes the sizeable majority of individuals with as yet unknown consequences in terms of delay. Rates of routine testicular self-examination (TSE) are unknown but probably negligible since health education in this arena is sparse. Indeed, evidence about just how self-discovery of symptoms comes about is lacking. Delay is usually determined through participant self-report, medical records, or a combination of both. Diclemente and Temoshok (1983) have noted that many articles neglect to state exactly how delay is established with individuals who self-report and what questions are asked to determine this. Different phraseology will elicit different responses. The use of language is clearly important, as this is a sensitive area of enquiry. When delay is unduly emphasised, participants can feel judged and may underreport time taken in seeking medical help (Worden & Weisman, 1975). Just such a fear is very relevant to a cancer, and testicular cancer is a case in point, where 115 MASON and STRAUSS embarrassment and stigma are commonly an issue, and even wholesale denial may have operated for a considerable time. Any potential evaluation apprehension (McBurney, 1998) should be reduced by ensuring the absence of implied judgement or expectation (Nosarti et al., 2000), though this is the exception rather than the rule. The objectivity of medical records has also been called into question (Diclemente & Temoshok, 1983) since delay is not systematically recorded and there is usually no explanation of how it has been determined from the available evidence. Some studies have acknowledged the difficulty in accurately determining delay and have sought to overcome this by the use of guided recall in face-to-face interviews (Lauver, 1994; Lauver & Tak, 1995) where care has been taken to improve accuracy by the use of memory cues. However, this dedication to obtaining an accurate estimation of delay is again the exception rather than the rule but is probably the only reliable way to determine delay in testicular cancer. Our own experience when interviewing is that considerable sensitivity and some rapport are required to obtain accurate information—something questionnaire measures may simply not achieve. DELAY AND PROGNOSIS Delay in seeking help for cancer symptoms has been shown to be important in terms of the staging of the disease at diagnosis and also survival rates. Several studies have found patient delay in breast cancer to associate with advanced disease staging at diagnosis (Lauver & Ho, 1993) and to contribute to increased mortality (see Richards, Westcombe, Love, Littlejohns, & Ramirez, 1999, for review). Others have found that patient delay has been associated with increased tumour size (Neave, Mason, & Kay, 1990; Rossi et al., 1990). Keinen, Carmil, and Reick (1991/1992) reported that there is a unanimous agreement among professionals of the importance of detecting breast cancer in its early stages and that this significantly enhances recovery. The largest meta-analysis (Richards et al., 1999) to date of more than one hundred thousand breast cancer patients concluded that delays of more than three months were significantly associated with lower survival and more advanced stage. Nosarti et al. (2000) also noted the need for public policy to encourage early detection to ensure early treatment and improve outcome. A similar picture is found with cancers other than breast cancer, though the evidence is sparser. Friedman et al. (1994) in their study on skin cancer suggest that differences in survival rates among different ethnic groups may be related to differences in the time taken to seek help. Studies that have sought to examine the relationship between delay behaviour, staging of the disease, and survival in testicular cancer have demonstrated more mixed results. One large-scale study of 352 men (Hernes, Harstad, & Fossa, 1996) conducted during three time periods over a time span of 12 years, found that patient delay of less than 16 weeks in men with Seminoma-type tumours was correlated with the incidence of stage I disease and that in all patients (both Teratoma-type and Seminoma-type) patient delay of three months or more was significantly correlated with a decreased five-year survival rate. Tavolini, Zuliani, Norcen, Dal Moro, Abatangelo, and Oliva (1999) found greater delay to be associated with more advanced staging in nonseminomas also. This and similar evidence suggests that it is 116 STUDYING HELP-SEEKING important and worthwhile to make attempts to shorten both patient delay and doctor delay by raising awareness and through educational programs. Hernes et al. (1996) further found that during that 12-year period there had been no significant reduction in patient delay or doctor delay, suggesting that there remains a lack of knowledge of testicular cancer in young men and primary care doctors. By way of exception, Chilvers et al. (1989) also found that shorter patient delay was correlated with earlier staging of the disease, but interestingly found that there was an inverse relationship between patient delay and relapse-free survival. Importantly, they propose that this is related to the fact that more aggressive, faster-growing tumours are more likely to result in symptoms that would lead men to seek medical attention sooner rather than less aggressive, slower-growing tumours. They still therefore conclude that seeking early medical attention for any testicular changes is essential and that their results do not invalidate this message. The findings that men with earlier staging have sought medical help sooner has also been supported by Bosl et al. (1981) and Thornhill, Fennelly, Kelly, Walsh, and Fitzpatrick (1987). In contrast, Fossa et al. (1981) found that there were no negative effects of delay either in terms of staging or survival, and Thornhill et al. (1987) found no relationship between delay and survival. Although the exact nature of the relationship between delay, disease staging, and survival remains unclear, the consensus is that men should present with testicular changes as early as possible. In conclusion, most studies support the urgency of early detection in various cancers, including skin cancer (Henrikkus, Girgis, Redman, & Sanden-Fisher, 1991), gastric cancer (Zilling, Walther, & Ahren, 1990), colorectal cancer (Dent et al, 1990), chest cancer (Koyi, Hillerdal, & Brandén, 2002), and testicular cancer (Chapple, Ziebland, & McPherson, 2004; Gascoigne, Mason, & Roberts, 1999; Sanden & Eriksson, 2000). EMPIRICAL STUDIES OF PSYCHOSOCIAL INFLUENCES The literature on psychosocial influences on delay has, in the main, been related to women and breast cancer symptoms, the past decade seeing three major reviews in the field of breast cancer and delay (Caplan & Helzlsouer, 1992; Faccione, 1993; Ramirez, 1999). However, there are some exceptions to the breast cancer literature including studies on those who have been diagnosed with bladder cancer (Mansson, Anderson, & Colleen, 1993), brain tumours (Salander, Bergenheim, Hamberg, & Henriksson, 1999), testicular cancer (Chapple et al., 2004; Gascoigne et al., 1999; Sanden & Eriksson, 2000), and a range of different cancers (Chakravorty, Chakravorty, Patel, DeSouza, & Doongaji, 1993; Mor et al., 1990). In addition, there have been studies on help-seeking and cancer symptoms prior to diagnosis, including rectal bleeding (Dent et al., 1990), signs of melanoma (Hennrikus et al., 1991) and lower urinary tract symptoms (Hunter & Berra-Unamuno, 1997). Though some aspects of the large literature on breast cancer are undoubtedly relevant, the obvious sex and age differences involved mean that psychosocial influences probably differ to those with testicular cancer. In particular, younger males might be expected to have less specific knowledge and different attitudes and beliefs about health, illness, and mortality, though the impact of these on the health behaviour of young men is largely unknown. 117 MASON and STRAUSS Several types of psychosocial factors have received the lion’s share of empirical attention that might broadly be classified as cognitive, affective, and social, though these are understandably related. Cognitive factors include health locus of control (“Is my health under my control?”), expectations of help-seeking outcome, the perceived value of seeking help, interpretations of symptoms, and beliefs with regard to susceptibility to cancer. Affective factors include anxiety, depression, anger, and optimism. Finally, a wide range of social factors have been studied, most notably the impact of perceived social norms and social support as well as race and socioeconomic status. Although breast cancer has been the main focus in this research area, some studies have included other cancers either by combining across several or examining a single disease site. We consider, in turn, some of the implications from questionnaire and interview-based studies of breast cancer and then of other cancers. Finally, we turn to testicular cancer, where the evidence so far is largely qualitative. BREAST CANCER STUDIES As there are no studies specific to testicular cancer using psychometric assessments, we have turned to the extensive literature on other cancers, most notably breast cancer. Some of the most extensive studies of breast cancer have been conducted by Lauver and colleagues; in particular, they have developed several measures for use at first presentation (Lauver, 1994; Lauver & Ho, 1993; Lauver & Tak, 1995)— something lacking for male cancers. For instance, Lauver and Ho (1993) found that longer delay was significantly associated with less habitual general healthcare behaviour and with having no identified practitioner. Greater anxiety was associated with less delay only for women who had no identified practitioner—a feature that is undoubtedly even more frequent for younger men. African-American women, Latino women, younger women, and those with lower occupational status also tended to have longer delays. Culture and race are highly pertinent and sensitive issues in the study of testicular cancer, too, though they may well operate differently in younger men. In one of the largest studies to date, Nosarti et al. (2000) interviewed 692 women presenting with symptoms to a breast clinic to determine delay, the reasons for it, presenting symptoms, mammogram histories, previous breast problems, and beliefs and attitudes toward cancer. Alongside many breast cancer specific findings, “long delay” (defined as waiting more than 27 days to seek medical help) was associated with the belief that symptoms were not serious, poor health awareness, fear of a cancer diagnosis, and higher levels of psychiatric morbidity. Fear and anxiety seem both able to motivate presentation for some (Lauver & Ho, 1993) and cause delay for others (Nosarti et al., 2000). Illustrating some potentially relevant standardised measures, Keinan et al. (1991) looked at the role of personality (health locus of control, hopelessness, repression-sensitisation, and trait anxiety) and behaviour patterns (body awareness) in predicting women’s delay following the discovery of a breast lump. They found no associations between the personality variables and delay, although lower body awareness did correlate with longer delay. Although this may be causal, it might also be that body awareness had increased in some women since diagnosis, and 118 STUDYING HELP-SEEKING direction of influence is a general issue in cross-sectional studies. Styra et al. (1993) were also interested in the concept of denial and how this affected presentation in those with breast lumps. Problem “tacklers” and problem “avoiders” were identified through the use of the Problem-Solving Interview (PSI), through which individuals were also classified as “identifiers” or “nonidentifiers” of a breast lump as a problem. However, there was no relationship between delay and identification of the breast lump as a problem, nor between depression/psychiatric morbidity and identification. Although a patient’s style of tackling health problems may be relevant, the evidence remains equivocal, and measures designed for general use may miss the relevance of affect and denial when specifically focussed on the symptoms of a specific potential cancer. A clear recommendation to emerge from the work on breast cancer is the need for the development of measures specific to the disease and patients themselves. These tend to produce a higher proportion of significant findings that are of greater relevance to the specific presentation of the illness. Richer themes can sometimes be better identified by interviews than the more restrictive questionnaire studies: Lauver et al. (1995) interviewed 138 women prediagnosis using open-ended questions to elicit reasons for and barriers to seeking care. Themes were established based on the interviews and then each interview examined to determine absence or presence of those themes. Half of responders indicated that there were no barriers, and these were significantly less likely to delay. Barriers included previous commitments, limited finance/insurance, fear, transportation problems, and lack of knowledge in terms of accessing services. Reasons women gave for seeking care included seeking consultation for physical symptoms, obtaining a diagnosis, addressing concerns or worries, dealing with risk of cancer, external influences, seeking early detection, and receiving treatment. Few if any of these are specific to breast cancer and may well apply in oncology generally. However, as we have already seen, many factors may be more specific to the symptomatology concerned. One recent large-scale study (Meechan, Collins, & Pertrie, 2003) examined the role of both symptoms and related emotional state in 85 women referred to a specialist breast clinic prior to their clinic appointment. Unsurprisingly, women with an identifiable breast lump and greater distress about their symptoms delayed for a significantly shorter period than those without. The nature of symptoms is clearly important, and the differences between an acutely presenting serious symptom such as bleeding and a less salient one are illustrated by a study of careseeking for signs of melanoma (Henrikkus et al., 1991). In this context, no relationship was found between delay and the experience of different or more numerous symptoms. The three top reasons given for not seeking help included thinking the symptom was not serious or that it would clear up in half of cases, having no time (11%), and deciding to wait and see (10%). The majority of participants believed that their susceptibility to melanoma at some point in their life was low. Many of these factors are shared with testicular cancer depending on the form of symptoms experienced. Burgess et al. (1998) conducted semi-structured interviews with 185 breast cancer patients following diagnosis. Those who delayed reported significantly less fear on the discovery of their symptoms, were less likely to have immediately disclosed their symptoms to another, and were more likely to have been prompted by another to finally seek help. In terms of immediate disclosure with regard to symptoms, 119 MASON and STRAUSS women living with partners were more likely to disclose immediately. As the previous paper demonstrates [see this issue: “Testicular Cancer: Passage Through the Help-Seeking Process for a Cohort of U.K. Men (Part 1)”], the role of partners is frequently a crucial one with respect to a patient’s response to testicular changes, suggesting that in this respect testicular cancer patients may resemble breast cancer patients. Mirroring the disparities of psychometric results, other interview results (Colbert, 1994) found that fear of diagnosis or of treatment, as well as the adoption of a “wait and see” approach, brought longer delay. Shorter delay was also associated with being married or living with a partner as opposed to being single or widowed. This is a poor study methodologically since not all women had self-discovered symptoms and true delay could not be ascertained, so conclusions from this paper are weak. In summary, when considering the implications for the, as yet, largely uncharted territory of testicular cancer, some of the particularities of testicular changes and their attribution as well as more broadly applicable psychosocial factors should be included. These require sensitive measurement that should probably go beyond standardized psychometrics. OTHER QUANTITATIVE STUDIES Considering studies of other individual cancer types, the particular medical features as well as different methods and measures make comparisons difficult and some factors are specific to the cancer involved. A study of brain tumour patients (Salander et al., 1999) illustrates this with results from 28 patients and their spouses. Three patient factors made individuals less inclined to identify themselves as being sick and in need of help. These included two factors that other studies have commented on: attribution of symptoms to nonserious causes or “less alien symptoms” (sic) and avoidance. However, the third is rather specific to brain tumour presentation and includes personality changes such as lethargy and the inability to initiate action or accurately judge the situation. Dent et al. (1990) explored delay in presentation following rectal bleeding and psychological factors, beliefs, and behaviour associated with this. Delay was found to be unrelated to age, sex, social status, availability of social support, and the belief that symptoms may indicate cancer. No relationship was found between any of the measured psychological traits (anxiety, depression, hypochondriasis, and emotional control) and delay. Once again the failure of general measures and the relevance of symptom interpretation and denial/avoidance are highlighted. The sole study to use postal questionnaires, Mansson et al. (1993) investigated presentation history in bladder cancer. Age and gender were not related to delay: the only clinical variable significantly associated with promptness in seeking help was haematuria (i.e., the appearance of blood in the urine). No significant relationships were found between delay and whether initial symptoms were considered serious, whether individuals had previous protracted illnesses, or educational level. The rather remote data collection may have been less sensitive than interviewing, and significant drop-out biased the sample toward younger people and those with lower stages of disease, suggesting this may not be a valuable data collection technique where sensitivity is a key, as is clearly the case in testicular cancer. 120 STUDYING HELP-SEEKING Few studies have investigated younger patients, though one recent study (Llewellyn, Johnson, & Warnakulasuriya, 2004) investigated under-45-year olds with oral squamous cell carcinoma (i.e., the second most common skin cancer after basal cell carcinoma)—itself also a relatively rare disorder increasing in prevalence. Delay was longest for those who lacked further education, who perceived themselves as under stress prior to diagnosis, and, intriguingly, those who smoked less tobacco. It is possible that the degree of attention to health may be greater in those with further education and, paradoxically, for those engaging in potentially risky behaviors. Several studies have contained a mixture of different cancer patients, including some that allow for their comparison. Mor et al. (1990) studied more than six hundred individuals with newly diagnosed lung, breast, and colorectal cancer. Results showed that colorectal cancer patients with more advanced disease at diagnosis or with another chronic illness were significantly less likely to have delayed. Breast cancer patients who also had another chronic illness were less likely to delay, but no relationships of this kind were observed for lung cancer patients. Taken together these results suggest that many psychosocial effects may be illness-specific. Chakravorty et al. (1993) used a standardised measure of psychiatric morbidity in a large mixed sample. Unlike the previous study, no attempt was made to differentiate between cancers, and they do not list those included. Unsurprisingly, those who had delayed had significantly higher psychological distress scores. The main reasons given for delay were that the cancer was not diagnosed by the primary caregiver, the patient was ignorant of the disease or did not realise he/she needed early treatment, relatives/friends had died of cancer, and fear or avoidance of cancer. The methodology is poorly documented, it appeared to confound referrer delay with that of the patient, and, as with other papers, the language implied blame of patients. The merging of patient and system delay could explain the unusually high number of patients (62%) whom they considered to have delayed a considerable amount of time. Although a study comparing testicular with other cancers is overdue, these many pitfalls require attention if valid results are to be obtained. QUALITATIVE APPROACHES TO TESTICULAR CANCER More recently there has been an interest in applying qualitative approaches to helpseeking behaviour. Least usefully perhaps, as they combined cancers of many types, de Nooijer, Lechner, and de Vries (2002) interviewed 23 men and women about the process. Unsurprisingly, many attributed symptoms to common ailments at first, although embarrassment and shame were contributors to delay. In addition to the study reported earlier, three qualitative studies have investigated testicular cancer (Chapple et al., 2004; Gascoigne et al., 1999; Sanden & Eriksson, 2000). Gascoigne et al. (1999) interviewed six participants using a semi-structured interview format to elicit information with regard to the history of the symptoms, thoughts and feelings, interpretations of symptoms, knowledge, and past behaviour in seeking help. They highlighted three important areas: “symptom appraisal,” “care seeking,” and “living up to images of masculinity.” They note that typically men attributed their symptoms to external causes, although one attributed it to cancer (with a delay of six 121 MASON and STRAUSS months). Men often shared their symptoms with others, usually partners or relatives, and this often resulted in encouragement to seek help. Half of the men involved were described as having been encouraged by their wives, while embarrassment and fear of diagnosis were barriers to seeking help. Although not a specific line of initial enquiry within this study, the third category of living up to images of masculinity emerged spontaneously from the data. This included issues of not feeling whole and of feeling judged by other men and the observation that women are more able than men to talk about personal issues. The 21 males in Sanden and Eriksson’s study (2000) also described the process of help-seeking. Commonly, men adopted a “wait and see” approach but also sought to define the reasons for their testicular changes. In common with the previous study, the authors related the “wait and see” approach to attributions to external causes, embarrassment about talking about testicular symptoms, avoidance of a cancer diagnosis, and confusion with fluctuating symptoms. Nine men chose not to talk to others, and six men did not talk to anyone prior to seeking help. Lastly, Chapple et al. (2004) found that those who sought help relatively quickly had heard about testicular cancer in the media, had seen leaflets in GPs’ surgeries, or knew others with this disease. Men who delayed feared appearing weak or being thought of as a hypochondriac or lacking in masculinity, recalled past illness or painful examinations, or were embarrassed. These papers raised issues once again related to attributions about symptoms. As with other studies, Salander et al. (1999) and Henrikkus (1991) found that the attributions people made with regard to symptoms were important to future helpseeking behaviour. However, Mansson et al. (1993) and Dent et al. (1990) found attributions had no relationship to delay. Overall these studies demonstrate the difficulty in establishing any definitive influences on cancer and delay, although various factors have emerged that deserve further attention: namely, attributions, symptoms, the role of partners, the role of anxiety, and embarrassment for males. CONCLUSIONS Several likely factors emerge from this selective review that might prove relevant to testicular cancer. Given its prominence in other forms of cancer, the issue of symptomatology and its relationship to delay is a highly pertinent one (Nosarti et al., 2000). In the public mind, cancer is commonly associated with lumps and pain, and these types of symptom have been commonly found to decrease delay. Caplan (1995), for example, found that nondelayers (less than two months) often had symptoms that increased as opposed to fluctuated, decreased, or remained static. Women with these symptoms may have interpreted their symptoms as more serious and, as we have seen, attributions concerning severity are influential. Crucially, testicular changes rarely involve pain—a fact unknown to most men. In several studies, poor health awareness was also associated with increased delay, and this is very likely to be the case with testicular cancer. Health education aimed at raising awareness of its symptoms and how to perform TSE (i.e., Testicular Self-Exam) is sorely needed, as is research into its effectiveness. An earlier review restricted to breast cancer (Ramirez et al., 1999) came to the conclusion that “overall, the evidence is currently insufficient to inform the develop122 STUDYING HELP-SEEKING ment of specific strategies to shorten delay by patients” (p. 1130). Little has happened to advance this state of affairs, and it certainly applies in the case of testicular cancer. They suggest that one useful way forward may be to take previous research findings and refine these with the use of qualitative research. Such research could also move away from the concept of separating individuals into “delayers” and “non-delayers” per se and seek to understand further the process of help-seeking across a wide range of delay times. One model of patient delay has delineated several stages, though it is uncertain whether this a useful way of understanding the process: several qualitative studies including our own (this issue) have highlighted the nonlinear nature of the process, with a uncertainty about symptoms and severity at several time-points. Overall, there is a great deal of variability of findings that is unsurprising given the varied nature of sampling, methodology, and measurement employed in studying patient delay in cancer. Nevertheless, some consistent results appear to implicate patients’ habits, norms, and expectations regarding both their health in general and specific symptoms of potential disease in particular. It is not the presence or absence of a symptom per se but how one perceives its cause, severity, controllability, or treatability that, in part, determines behaviour. The role of emotional processes remains less certain, though they are undoubtedly an important part of delay. Distress is another variable to emerge of substantive influence, at least for some in some contexts. A simple relationship is unlikely to be the case in testicular cancer since processes of defence and denial often operate to reduce apparent distress while increasing delay yet further. In this context, avoidance has been highlighted by several qualitative studies as a key contributor to delay. Key methodological suggestions highlighted by the review included the utility of comparing different samples rather than combining several cancer groups without discrimination. A clear need is seen for measures that are specific and sensitive to the issues in testicular cancer. While these may well include questionnaires, they probably need to be administered in the context of sensitive interviewing since even the determination of the length and nature of delay has pitfalls for the overly simplistic measure. The early stages of just how a symptom has been detected and the process by which this is acted upon are still largely unknown, and these issues exemplify the need for nonblaming and in-depth research. We would recommend adoption of the less pejorative phrase “lag-time,” noting that this is multi-determined and implies no criticism of the patient. Given the fear and embarrassment that surrounds open discussion of cancer, something particularly highlighted by several qualitative studies of testicular cancer, good relationships with physicians who model a comfortable handling of sensitive issues is paramount. At the beginning of the review, the disparity in men’s and women’s health behaviour was noted, with consequences for mortality rates. At least part of this difference may result from a disparity in health awareness and knowledge, and research highlighting testicular cancer seems a case in point with low awareness and poor knowledge of its symptoms. While most testicular cancer was self-detected (or detected by a partner), this was a case of passively noticing change rather than a result of testicular self-examination (to our knowledge something not mentioned by a single respondent in qualitative studies including our own). Health education may 123 MASON and STRAUSS help lead to much greater use of TSE in the future, and it will be interesting to see whether this is indeed the case and whether it has an impact on delay. Given the relatively young age of many patients, it may be that the diversity of emerging male gender roles and less “traditional reluctance” in care seeking will lead to changes to patterns of healthcare utilisation in younger men. Much empirical research suffers from the absence of social and economic influences, and these too have been shown to be critical in other cancers. While these may operate via intrapsychic processes, they also undoubtedly have a direct effect on delay—via availability of care, for example. Not only should quantitative studies continue to elaborate on the findings of this corpus of evidence, extending it to other cancers, but qualitative approaches may help to elucidate why these factors have their effects. Together these approaches may help improve the prospects of reducing delay by informing effective education and intervention. NOTE 1. Staging is a system by which malignant tumours are classified. This is done using information about primary tumours, regional lymph node status, and the absence or presence of distant metastases. An overall clinical stage is then allocated (I to IV). The use of the staging system enables the evaluation of treatment and may help clinicians in deciding about prognoses and appropriate management (Rees et al., 1993). REFERENCES Abdel-Fattah, M.M., Anwar, M.A., Mari, E., El-Shazly, M.K., Zaki, A.A., Bedwari, R.N., et al. (1999). Patient- and system-related diagnostic delay in breast cancer. European Journal of Public Health, 9, 15-19. Andersen, B.L., & Cacioppo, J.T. (1995) Delay in seeking a cancer diagnosis: Delay stages and psychophysiological comparison processes. British Journal of Social Psychology, 34(1), 33-52. Antonovsky, A., & Hartman, H. (1974). Delay in the detection of cancer: A review of the literature. Health Education Monographs, 2, 98-128. Burgess, C.C., Ramirez, A.J., Richards, M.A., & Love, S.B. (1998). Who and what influences delayed presentation in breast cancer? British Journal of Cancer, 77, 1343-1348. Burgess, C.C., Ramirez, A.J., Smith, P., & Richards, M.A. (2000). Do adverse life events and mood disorder influence delayed presentation of breast cancer? Journal of Psychosomatic Research, 48, 171-175. Caplan, L.S. (1995). Patient delay in seeking help for potential breast cancer. Public Health Reviews, 23, 263-274. Caplan, L.S., & Helzlsouer, K.J. (1992) Delay in breast cancer: A review of the literature. Public Health Reviews, 20, 187-214. Carter, S., & Winslet, M. (1998) Delay in the presentation of colorectal carcinoma: A review of causation. International Journal of Colorectal Disease, 13, 27-31. 124 STUDYING HELP-SEEKING Chakravorty, S.G., Chakravorty, S.S., Patel, R.R., Desouza, C.J., & Doongaji, D.R. (1993). Delay in specialist consultation in cancer patients. Indian Journal of Cancer, 30, 61-66. Chapple A., Ziebland S., & McPherson A. (2004). Qualitative study of men’s perceptions of why treatment delays occur in the U.K. for those with testicular cancer. British Journal of General Practice, 54, 25-32. Colbert, K. (1994, June). Why opt for an unnecessary delay? Professional Nurse, 643-645. Courtenay, W.H. (2000). Constructions of masculinity and their influence on men’s well-being: A theory of gender and health. Social Science and Medicine, 50, 1385-1401. Dearnaley, R.A., Huddart, R.A., & Horwich, A. (2001) Managing testicular cancer. British Medical Journal, 322, 1583-1588. Dent, O.F., Goulston, K.J., Tennant, C.C., Langeluddecke, P., Mant, A., Chapius, P.H., et al. (1990). Rectal bleeding. Patient delay in presentation. Diseases of the Colon and Rectum, 33, 851-857. de Nooijer, J., Lechner. L., de Vries, H. (2001). A qualitative study on detecting cancer symptoms and seeking medical help; an application of Andersen’s model of total patient delay. Patient Education and Counselling, 42(2), 145-157. Diclemente, R.J., & Temoshok, L. (1983). Enhancing the value of patient delay studies for cancer control: Methodological and statistical considerations. Advances in Cancer Control: Research and Development, 20, 129-137. Facione, N.C. (1993). Delay versus help-seeking for breast cancer symptoms: A critical review of the literature on patient and provider delay. Social Science and Medicine, 36, 1521-1534. Facione, N.C., & Dodd, M.J. (1995). Women’s narratives of helpseeking for breast cancer. Cancer Practice, 3, 219-225. Forman, D., & Moller, H. (1994). Testicular cancer. Cancer Surveys, 19-20, 323341. Friedman, L.C., Bruce, S., Weinberg, A.D., Cooper, P., Yen, A., & Hill, M. (1994). Early detection of skin cancer: Racial/ethnic differences in behaviors and attitudes. Journal of Cancer Education, 9, 105-110. Gascoigne, P., & Whitear, B. (1999). Making sense of testicular cancer symptoms: A qualitative study of the way in which men sought help from the health-care services. European Journal of Oncology Nursing, 3, 62-69. Gascoigne, P., Mason, M.D., & Roberts, E. (1999). Factors affecting presentation and delay in patients with testicular cancer: Results of a qualitative study. Psycho-Oncology, 8, 144-154. Henrikkus, D., Girgis, A., Redman, S., & Sanden-Fisher, R.W. (1991). A community study of delay in presenting with signs of melanoma to medical practitioners. Archives of Dermatology, 127, 356-361. Hunter, D.J., & Berra-Unamuno, A. (1997). Treatment-seeking behaviour and stated preferences for prostatectomy in Spanish men with lower urinary tract symptoms. British Journal of Urology, 79, 742-748. 125 MASON and STRAUSS Keinan, G., Carmil, D., & Reick, M. (1991). Predicting women’s delay in seeking medical care after discovery of a lump in the breast: The role of personality and behavior patterns. Behavioral Medicine, Winter, 177-183. Koyi, H., Hillerdal, G., & Brandén, E. (2002). Patient’s and doctors’ delays in the diagnosis of chest tumors. Lung Cancer, 35(1), 53-57. Lahelma, E., Martikainen, P., Rahkonen, O., & Silventoinen, K. (1999). Gender differences in ill health in Finland: Patterns, magnitude and change. Social Science and Medicine, 48, 7-19. Lauver, D. (1994). Care-seeking behavior with breast cancer symptoms in Caucasian and African-American women. Research in Nursing and Health, 17, 421-431. Lauver, D., & Ho, C.H. (1993). Explaining delay in care seeking for breast cancer symptoms. Journal of Applied Social Psychology, 23, 1806-1825. Lauver, D., & Tak, Y. (1995). Optimism and coping with a breast cancer symptom. Nursing Research, 44, 202-207. Lauver, D., Coyle, M., & Panchamatia, B. (1995). Women’s reasons for and barriers to seeking care for breast cancer symptoms. Women’s Health Institute, 5, 27-35. Llewellyn, C.D., Johnson, N.W., & Warnakulasuriya, S. (2004) Factors associated with delay in presentation among younger patients with oral cancer. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology, 97, 707-713. Mansson, A., Anderson, H., & Colleen, S. (1993). Time lag to diagnosis of bladder cancer—Influence of psychosocial parameters and level of health-care provision. Scandinavian Journal of Urology and Nephrology, 27, 363-369. McBurney, D.H. (1998). Research methods (4th ed.). London: Brooks/Cole. Meechan, G., Collins, J., & Petrie, K.J. (2003). The relationship of symptoms and psychological factors to delay in seeking medical care for breast symptoms. Preventive Medicine, 36(3), 374-378. Mor, V., Masterson-Allen, S., Goldberg, R., Guadagnoli, E., & Wool, M.S. (1990). Pre-diagnostic symptom recognition and help-seeking among cancer patients. Journal of Community Health, 15, 253-266. Neave, L., Mason, B., & Kay, R. (1990). Does delay in diagnosis of breast cancer affect survival? Breast Cancer Research and Treatment, 15, 103-108. Nezu, A.M., Nezu, C.M., Friedman, S.H., Faddis, S., & Houts, P.S. (1998). Helping cancer patients cope. A problem-solving approach. Washington, DC: American Psychological Association. Nosarti, C., Crayford, T., Roberts, J.V., Elias, E., McKenzie, K., & David, A.S. (2000). Delay in presentation of symptomatic referrals to a breast clinic: Patient and system factors. British Journal of Cancer, 82, 742-748. Pack, G.T., & Gallo, J.S. (1938). The culpability for delay in the treatment of cancer. American Journal of Cancer, 33, 443-462. Quinn, M., Babb., P., Brock, A., Kirby, L., & Jones, J. (2001) Cancer trends in England and Wales, 1950-1999. London: Office for National Statistics. Rees, G.J., Goodman, S.E., & Bullimore, J.A. (1993). Cancer in practice. Oxford: Butterworth-Heinemann. 126 STUDYING HELP-SEEKING Richards, M.A., Westcombe, A.M., Love, S.B., Littlejohns, P., & Ramirez, A.J. (1999). Influence of delay on survival in patients with breast cancer: A systematic review. The Lancet, 353, 1119-1126. Rossi, S., Cinini, C., Di Pietro, C., Lombardi, C., Crucitti, A., Bellatone, R., et al. (1990). Diagnostic delay in breast cancer: Correlation with disease stage and prognosis. Tumori, 76, 559-562. Salander, P., Bergenheim, A.T., Hamberg, K., & Henriksson, R. (1999). Pathways from symptoms to medical care: A descriptive study of symptom development and obstacles to early diagnosis in brain tumour patients. Family Practice, 16, 143-148. Sanden, I., & Eriksson, C. (2000). An interview study of men discovering testicular cancer. Cancer Nursing, 23, 304-309. Styra, R., Sakinofsky, I., Mahoney, L., Colapinto, N.D., & Currie, D.J. (1993). Coping styles in identifiers and nonidentifiers of a breast lump as a problem. Psychosomatics, 34, 53-60. Tavolini, I.M., Zuliani, G., Norcen, M., Dal Moro, F., Abatangelo, G., & Oliva, G. (1999). Prevention and early diagnosis of testicular neoplasms. Archivio Italiano di Urologia, Andrologia, 71, 27-30. Toklu, C., Ozen, H., Sahin, A., Rastadoskouee, M., & Erdem E. (1999). Factors involved in diagnostic delay of testicular cancer. International Urology & Nephrology, 31, 383-8. Watson, J. (2000). Male bodies: Health, culture and identity. Buckingham: Open University Press. Worden, J.W., & Weisman, A.D. (1975). Psychosocial components of lagtime in cancer diagnosis. Journal of Psychosomatic Research, 19, 69-79. Zilling, T.L., Walther, B.S., & Ahren, B. (1990). Delay in diagnosis of gastric cancer: A prospective study evaluating doctors’ and patients’ delay and its influence on five year survival. Anticancer Research, 10, 411-416. 127