Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
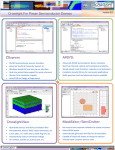
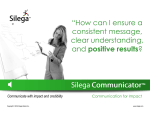
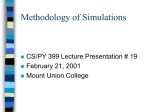
Simulation Techniques for Risk-Based Financing Estimates in Behavior... http://www.crystalball.com/articles/yennie.html > Back to the Article Library CRYSTAL BALL ARTICLES Simulation Techniques for Risk-Based Financing Estimates in Behavioral Health Managed Care By Henry Yennie, BCSW November 11, 1999 Background As managed care initiatives sweep through public sector behavioral health and social services, an increasing number of providers are faced with estimating costs, prices and/or rates for a risk-based financing project. These estimates are fraught with danger and tremendous risk for these organizations, many of which have difficulty with basic cost-finding analyses. This paper outlines a model for rate setting that introduces the concept of simulation modeling to the traditional rate estimation process. The purpose is to assist organizations in understanding the nature of the risk in these types of arrangements and to assist in the formulation of realistic rate estimates. The Basics of Capitation Rate Setting The tools for rate setting vary from organization to organization with the most common being a spreadsheet-based model. In this paper we will focus on capitation rate setting and use a typical HMO carve-out model as the example. The most common calculation method for determining a capitation rate is the fee-for-service method, which projects the cost of services delivered based on the contracted or calculated costs per unit of service. The projected utilization of different types of services is combined with the projected costs per unit of service to yield a total cost translated into a per member per month rate. In general, a capitation rate will have the following three components: 1. The estimated cost of direct clinical services, expressed as a "per member per month" number. This component of the capitation rate expresses the organization’s projection of the cost of delivering direct clinical services to the covered group and results from the following formula: Cost of Service = Number of services x cost per unit of service The number of services to be delivered is a function of the following variables: ITEM DEFINITION Population Penetration The number of covered members who will actually use services Utilization per 1,000 Number of services used by the covered members expressed in per 1,000 member units. This number is derived by calculating: The total episodes of care 1 of 12 2/28/05 2:43 PM Simulation Techniques for Risk-Based Financing Estimates in Behavior... http://www.crystalball.com/articles/yennie.html The average length of each episode The total number of units of service The formula for services per 1,000 members may be used to calculate the statistic for any time period chosen, such as for the day, for the month, year to date, and so forth. When calculating units per 1000, use the assumption of a 365-day year as opposed to a 12-month year to prevent variations that are due solely to the length of the month. The formula is as follows: [A / (B / 365)] / (C / 1000) Where A = services per time unit B = days per time unit C = plan membership This calculation can and should be done for hospital days, outpatient visits, and all other levels of care. Depending upon the types of covered services, as defined in the benefit plan, the organization must determine the utilization of services for a variety of levels of care. A common "continuum of care" for which utilization must be projected is as follows: Acute 24-hour care and 23-hour observation Partial hospitalization and day treatment Intensive outpatient services Outpatient service Again, depending upon the benefit plan, these utilization projections should be calculated for both mental health and chemical dependency services separately. Also, given the organization’s scope of services or the composition of the network, this continuum may be expanded or contracted to reflect the range of services available for member treatment. Combining these variables into an "experience table" for our sample member group of 92,000 covered lives for one year of service might look as follows: Level of Care Penetration Admits ALOS Total Units Days/Visits/1000 Inpatient MH 0.32% 298 7 2,027 22.0 Partial MH 0.07% 64 6 412 4.5 Alt. Res. MH 0.00% 2 155 286 3.1 Outpatient MH 1.67% 1,533 7 10,422 113.3 Inpatient CD 0.06% 59 6 365 4.0 Partial CD 0.04% 35 7 238 2.6 Alt. Res. CD 0.00% 3 9 23 0.3 Outpatient CD 0.01% 6 4 23 0.3 Combining the utilization projections with the cost of service estimates will yield the first general estimate of the capitation rate. 2 of 12 2/28/05 2:43 PM Simulation Techniques for Risk-Based Financing Estimates in Behavior... http://www.crystalball.com/articles/yennie.html Costs for services can be determined as follows: If the organization is accepting capitation for its services only, a full cost study should be completed to determine both the direct and indirect costs for each type of service to be delivered by the organization under the capitation arrangement. This can be derived from financial and statistical reports, and it should take into account all of the overhead expenses required to deliver those services. If the organization is providing services through a network of practitioners, then the organization should have contracts with those practitioners that state the rates to be paid for various services. If these practitioners include hospital units and other facility-based services, then per diem contracts should be obtained to facilitate cost projections as well as contain costs for the contract. The determination of unit costs can be fairly straightforward for institutional services that are based on per diem payments. If, for example, the psychiatric inpatient service network consists of two hospitals, one with a $400 per diem and the other with a $500 per diem, a simple average or weighted average based on the projected volume of services to be delivered by each can be used. The following is an example: Facility Total Days Per Diem Total Cost Unit A 250 $400 $100,000 Unit B 350 $500 $175,000 Totals 600 $275,000 Weighted Average Cost per Day $458.33 A similar method can be used to determine the average cost per unit of outpatient service when the organization uses clinicians with varying disciplines and contract rates. 2. The estimated overhead costs required to support the management of the contract expressed as a "per member per month" number. Every capitated arrangement will require support services and an administrative infrastructure to support the services directly provided by the organization and to support the authorization and payment of services provided by others through a network. These overhead costs should be carefully detailed and added to the direct costs of clinical services to arrive at an equitable capitation rate. Failure to incorporate some portion of overhead costs in a capitated arrangement can lead to negative financial results. Overhead costs can be estimated by preparing a budget outlining the type, number and costs of the services required to support management of the contract. The total cost of these administrative services is then converted into a PMPM rate and added to the direct clinical cost PMPM to continue building the capitation estimate. Some of the elements influencing the type and size of supporting administrative infrastructure are as follows: Type of clinical management protocol utilized (i.e. aggressive, moderate, etc.) Number of covered lives and number of benefit plans administered Use and required size of a practitioner network Quality and clinical efficiency of the organization and/or the provider network National Committee on Quality Assurance (NCQA) and Health Plan Employer Data and Information Set (HEDIS) reporting requirements Presence and nature of claims payment requirements 3 of 12 2/28/05 2:43 PM Simulation Techniques for Risk-Based Financing Estimates in Behavior... http://www.crystalball.com/articles/yennie.html Presence and nature of member service requirements As with utilization control and risk management, a large group size allows the organization to more effectively spread the overhead costs. Further, if overhead costs can be allocated among several different capitation contracts, the organization can allocate more of each capitation rate to clinical service delivery and profit. 3. The estimated profit for the organization expressed as a "per member per month" number. The third major component of a capitation rate is the allocation of an amount for profit and an allowance for capital costs. This can be either a fixed cost added to the two other components of clinical service costs and overhead or a percentage of the total costs. The latter method is the most common. While there is wide variation in the percentage of profit allocated to a contract, a common range is 6% to 10% of total costs. In our sample model, we will focus only on the first rate component, the cost of care. VARIABILITY AND RISK IN THE MODEL Most organizations tend to construct this model in a spreadsheet, using single-point estimates for the variables involved to arrive at an estimated rate. What is usually missing from these models is a calculation of the probability of the estimate occurring along with an estimate of the degree of risk involved in each of the variables and in the final estimate. Using our sample data for the HMO carve-out, we can construct a model similar to the following: Level of Care Units/1000 Cost per Unit Cost PMPM Inpatient MH 22.0 $458.33 $0.841 Partial MH 4.5 $225.00 $0.084 Alt. Res. MH 3.1 $75.00 $0.019 Outpatient MH 113.3 $58.00 $0.548 Inpatient CD 4.0 $458.33 $0.152 Partial CD 2.6 $225.00 $0.048 Alt. Res. CD 0.3 $75.00 $0.002 Outpatient CD 0.3 $85.00 $0.002 TOTALS $1.696 The "Cost PMPM" was derived using the following formula: (Forecast Annual Utilization Rate/1000) x FFS Rate ___________________________________ 12 Months As an example, the formula for inpatient mental health is: (0.022*458.33)/12 Given the data in our sample, this procedure yields an initial rate estimate for the cost of services of $1.696 per member per month. As the model is in spreadsheet form, we can manipulate the values of each cell to see the effect on the final cost of care. 4 of 12 2/28/05 2:43 PM Simulation Techniques for Risk-Based Financing Estimates in Behavior... http://www.crystalball.com/articles/yennie.html LIMITS OF SPREADSHEET MODELS In our model for the cost of services, variables can be characterized as either "unknown" (we have no knowledge about the true value) or "uncertain"(some knowledge about the true value). The major variables that are unknown or uncertain are: Penetration rates for the various levels of care Utilization assumptions for the various levels of care, primarily ALOS Cost assumptions for the various levels of care Once we have reached this point in our model construction and recognize the potential variability in the estimate, we are faced with a common dilemma: What values do we change and what are the probabilities of those values occurring in real life? In other words, how do we know our estimate is valid, and what is the nature and extent of the risk involved for our organization? We typically answer these questions using a variety of single-point variations in the model, i.e. we change the value of one cell and see the effect on the target value (The "Cost PMPM" in our model). We can go a step further and construct "worse case", "most likely case", and "best case" scenarios. But again, this limits us to three likely outcomes, and we are still missing a measure of the degree of risk involved and the probability of any of those cases occurring. We are still faced with a substantial obstacle: How many changes and what changes do we make for the variables? In our model, for example, it would be impractical to substitute a variety of different possible values for the "outpatient mental health visits per 1000 per month" variable in order to see the outcome on cost. This type of single-cell input is impractical for all the variables in the model. Although it might be physically possible to substitute a large number of values for each variable, it quickly becomes practically impossible to track the effects of each change on the target cell. David T. Hulett succinctly states the problem: "Future estimates are not facts but statements of probability about how things will turn out. Because estimates are probabilistic assessments, costs may actually be higher or lower than estimated even by seasoned professional estimators." USING SIMULATION TECHNIQUES The use of simulation techniques allows us to directly address the probability features of a capitation estimate by conducting a large number of "what ifs" on each uncertain variable in the model. In short, it allows us to perform a cost risk analysis. This type of analysis allow us to answer the following questions: "What is the most likely cost?" The traditional method assumes that this is the baseline cost computed by summing the estimates of cost for the various levels of care, but this is not so. "How likely is the baseline estimate to be overrun?" Traditional methods do not address this problem. "What is the cost risk exposure?" This is also the answer to the question; "How much contingency do we need on this project?" For capitation projects, the issue would the correct amount of reserves to set aside for potential cost overruns. "Where is the risk in this project?" This is the same as: "Which cost elements cause the most need for the contingency?" Risk analysis principles can be used to answer this question. Use of simulation techniques in rate setting is recognition of the variability inherent in the "uncertain" variables in the model. The quickest and most efficient way to perform these analyses 5 of 12 2/28/05 2:43 PM Simulation Techniques for Risk-Based Financing Estimates in Behavior... http://www.crystalball.com/articles/yennie.html is through the use of simulation software. This example will use Crystal BallÓ by Decisioneering, Inc. to illustrate the advantages of these techniques. Additional Data Requirements All cost risk estimate techniques are based on probability distributions. A probability distribution describes the likelihood of specific values occurring out of a range or set of values. If the range of values is limited to certain fixed values, the probability distribution is said to be discrete. If the range of values contains an infinite set of possible values, the distribution is said to be continuous. Depending upon the nature of the data, there are a variety of probability distribution types that can describe the data. The two most popular distribution types that "fit" behavioral healthcare data include: The Triangular distribution: The triangular distribution shows the number of successes when you know the minimum, maximum, and most likely values. For example, you could describe the number of intakes seen per week when past intake data show the minimum, maximum, and most likely number of cases seen. It has a continuous probability distribution. The parameters for the triangular distribution are Minimum, Maximum, and Likeliest. There are three conditions underlying triangular distribution: The minimum number of items is fixed. The maximum number of items is fixed. The most likely number of items falls between the minimum and maximum values, forming a triangular shaped distribution, which shows that values near the minimum and maximum are less apt to occur than those near the most likely value. The Lognormal distribution: The lognormal distribution is widely used in situations where values are positively skewed (where the distribution has a long right tail; negatively skewed distributions have a long left tail; a normal distribution has no skewness). Examples of data that "fit" a lognormal distribution include financial security valuations or real estate property valuations. Financial analysts have observed that the stock prices are usually positively skewed, rather than normally (symmetrically) distributed. Stock prices exhibit this trend because the stock price cannot fall below the lower limit of zero but may increase to any price without limit. Similarly, healthcare costs illustrate positive skewness since unit costs cannot be negative. For example, there can’t be negative cost for services in a capitation 6 of 12 2/28/05 2:43 PM Simulation Techniques for Risk-Based Financing Estimates in Behavior... http://www.crystalball.com/articles/yennie.html contract. This distribution accurately describes most healthcare data. The parameters for the lognormal distribution are Mean and Standard Deviation. The three conditions underlying lognormal distribution are: The unknown variable can increase without bound, but is confined to a finite value at the lower limit. The unknown variable exhibits a positively skewed distribution. The natural logarithm of the unknown variable will yield a normal curve. Other common distribution types not used in this paper include: Binomial Beta Custom Exponential Extreme Value Gamma Geometric Hypergeometric Logistic Negative Binomial Normal Pareto Poisson Uniform Weibull In order to describe the distribution types of the "uncertain" variables in our model, we need additional data about the uncertain variables. There are several sources for this additional data: Analysis of Historical Data: If an organization has historical data describing an uncertain variable, a simple analysis will yield the appropriate distribution and parameters, such as the mean and the standard deviation. Interviews with Experts: In those cases where historical data is unavailable or unreliable, additional information may be obtained from interviews with staff or other experts. This is particularly applicable for descriptions of data that fit a triangular distribution. As Hulett states, "(Interview) participants can describe and estimate the low, most likely and high range estimates." Proxy Estimates: Proxy estimates refer to the use of similar data sets. These can often be obtained from consulting firms specializing in claims data analysis and risk-based rate 7 of 12 2/28/05 2:43 PM Simulation Techniques for Risk-Based Financing Estimates in Behavior... http://www.crystalball.com/articles/yennie.html estimation. Once an organization is able to describe the likely distributions of the uncertain variables, simulation techniques can be employed. We will employ the Monte Carlo simulation technique as used in the Crystal BallÓ software. This technique employs a series of random numbers, constrained by the distribution parameters chosen, to calculate the cost risk model and the resulting effect on the target cells – the cost of care. This technique can accommodate models such as ours that have a large possible number of "what-ifs" that would be impractical to manipulate on a case-by-case basis. As an example, the process can conduct up to 10,000 trials – or "what ifs" – on each assumption cell using the parameters defined in the underlying distribution. As Hulett states, "A Monte Carlo simulation "solves" the problem many times. Each solution is called an iteration. For each iteration, the simulation program selects a cost (or utilization parameter) at random from the probability distribution specified by the analyst for each uncertain cost (or utilization) element." Another sampling technique available in Crystal Ball is the Latin Hypercube method or (technique). This differs from the Monte Carlo technique in that it uses a stratified sampling technique. This is preferable when additional accuracy in distribution "tails" is desired. In other words, Latin Hypercube simulation stratifies the distribution and ensures that "what-if" values are chosen from each stratum. On the other hand, Monte Carlo simulation chooses "what if" values at random from the entire range of the distribution, and consequently may or may not take sufficient sample values from the tails. The differences in the techniques can be illustrated in the following simple drawing: For illustrative purposes, we used a lognormal distribution for the "uncertain" penetration rates in the model. Using the data in our sample model, we defined the following distributions for the uncertain utilization variables: Assumption: Inpatient MH Lognormal distribution with parameters: Mean Standard Dev. Assumption: Partial MH Lognormal distribution with parameters: Mean 8 of 12 0.32% 0.10% 0.07% 2/28/05 2:43 PM Simulation Techniques for Risk-Based Financing Estimates in Behavior... http://www.crystalball.com/articles/yennie.html Standard Dev. Assumption: Outpatient MH Lognormal distribution with parameters: Mean Standard Dev. Assumption: Inpatient CD Lognormal distribution with parameters: Mean Standard Dev. Assumption: Partial CD Lognormal distribution with parameters: Mean Standard Dev. Assumption: Outpatient CD Lognormal distribution with parameters: Mean Standard Dev. 0.02% 1.67% 0.50% 0.06% 0.02% 0.04% 0.01% 0.01% 0.01% Using the software’s capability to run 10,000 trials, we produced the following means for the model: Level of Care Penetration Admits ALOS Total Units Units/ 1000 Unit Cost Cost PMPM Inpatient MH 0.33% 300 7 2,037 22.1 458.3 0.846 Partial MH 0.07% 64 6 411 4.5 225.0 0.084 Alt. Res. MH 0.00% 2 155 286 3.1 75.0 0.019 Outpatient MH 1.67% 1,532 7 58.0 0.547 Inpatient CD 0.06% 59 6 367 4.0 458.3 0.152 Partial CD 0.04% 35 7 239 2.6 225.0 0.049 Alt. Res. CD 0.00% 3 9 23 0.3 75.0 0.002 Outpatient CD 0.01% 5 4 23 0.3 85.0 0.002 TOTALS 2.17% 2,000 10,419 113.2 1.701 The model produced a mean expected Cost PMPM of $1.701, very near our spreadsheet estimate. One frequency chart output of the model can be illustrated as follows: 9 of 12 2/28/05 2:43 PM Simulation Techniques for Risk-Based Financing Estimates in Behavior... http://www.crystalball.com/articles/yennie.html The following important information can be obtained from this chart: The range of possible "Costs PMPM" plus or minus three standard deviations from the mean of $1.701 is $0.750 to $2.750. This represents a wide range of possible outcomes (99.73%). The "certainty level" of actual costs coming in at or below the projected mean of $1.701 is only 54.4%. In other words, given the nature of the underlying data, we have a 45.6% chance of the actual Cost PMPM being more than the projected mean. The "negative outcomes" indicate the areas of probability where the costs exceed the capitation revenue of $1.701 PMPM. Another view of the output is a cumulative chart: The blue-shaded area shows the range of possible outcomes below the mean at the 54% certainty level. Another way to view this output is that the organization would have to provide at least $1.05 PMPM in reserve to cover possible cost overruns. For most organizations, this is an unacceptable level of risk. An organization willing to tolerate only a 20% chance of cost overruns would require a PMPM rate of at least $1.946 as illustrated below ($2.750 – $1.701): 10 of 12 2/28/05 2:43 PM Simulation Techniques for Risk-Based Financing Estimates in Behavior... http://www.crystalball.com/articles/yennie.html DETERMINING THE RISK IN THE MODEL Simulation can be used effectively to determine the nature/source of uncertainty of the risk inherent in the model through the use of sensitivity analysis. A key output of the software is the identification of the specific variables that have the greatest effect on the outcomes of the model. We can rank the variables by their contribution to risk in the model. This analysis allows an organization to focus analytical resources on those uncertainties in the estimate that matter the most. For our sample model, the sensitivity analysis is as follows: Given our data, the two variables of Inpatient Mental Health utilization and Outpatient Mental Health utilization together contribute to 97% of the variance in the model. This has two important implications: 1. The analysis points to these two variables as those most likely to contribute to variance from the mean cost PMPM. Thus, they should be primary targets for clinical improvement and management and should become "key indicators" for the project. Additional planning and discussions with clinical leadership can often yield strategies for control of these important variables. 2. Because of their importance, the organization can devote additional analytical resources to the data that produced the underlying distributions. Perhaps another data set can be acquired and the distribution parameters refined. The sensitivity analysis allows an organization to focus resources on those variables that matter the most in the model and the ultimate outcome. Summary This paper has outlined the relative advantages of using simulation techniques in the development of risk-based pricing proposals. Traditional spreadsheet models that rely on single-point cost and utilization estimates do not furnish adequate information on the potential risk involved. Using simulation software such as Crystal Ball® , we were able to calculate a large number of "what ifs" on each uncertain variable defined in the model. As Hulett states, "Traditional methods cannot answer the important questions of: (1) How likely are we to overrun? (2) What is our exposure? and (3) Where is the risk in the project?" Using Monte Carlo simulation, 11 of 12 2/28/05 2:43 PM Simulation Techniques for Risk-Based Financing Estimates in Behavior... http://www.crystalball.com/articles/yennie.html an organization faced with a capitation opportunity can gain critical knowledge about the reasonableness of rates, and the nature of the risk involved in the model. The sample used in this paper is a simple reproduction of complex financial models used in actual rate estimates. An actual model would involve a larger number of variables An organization should be prepared to devote sufficient resources to data gathering and analysis in order to ensure these methods produce reliable data. For more information, contact: Henry Yennie, BCSW Senior Associate 1219 Carter Avenue Baton Rouge, LA 70806 225-923-2343 voice 225-924-3622 fax [email protected] Return to Top Home | Risk Resources | Products | Services | Support | News | About Us | How to Buy © 2000-2003 Decisioneering, Inc. 12 of 12 2/28/05 2:43 PM