Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Aortic stenosis wikipedia , lookup
Antihypertensive drug wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Coronary artery disease wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
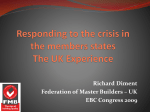
730 In Vivo Relation of Intramyocardial Blood Volume to Myocardial Perfusion Evidence Supporting Microvascular Site for Autoregulation Xue-si Wu, MD; Daniel L. Ewert, PhD; Yun-He Liu, MD; and Erik L. Ritman, MD, PhD Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Background. The goal of this study was to explore the role of several factors that affect intramyocardial blood volume by using minimally invasive computed tomography. Anesthetized dogs were scanned with the dynamic spatial reconstructor, a high-speed tomographic scanner, during injection of a bolus of iohexol into the aortic root. Methods and Results. In control dogs, it is indicated that the fraction of myocardium that is blood (FMB, %) relates to myocardial perfusion (F, milliliters per gram per minute) in that region as FMB--a *F.2, where a=9.5± 1.2% (milliliters times minute per gram) '2 (mean± SD) in the subendocardium and a=9.6+1.1% in the subepicardium. In another group of dogs, for the myocardium perfused by a stenosed epicardial artery, a increased to approximately 10 for a 25-43% stenosis (or pressure gradient of 9 mm Hg across narrowing) and to greater than 11 for a 50-55% stenosis (or pressure gradient of 40 mm Hg across narrowing). In these dogs, flow was not impaired under control hemodynamic conditions, but the usual increase of flow (i.e., flow reserve) observed under maximum vasodilation conditions was impaired. In another group of dogs, progressive embolization (using 15-,um-diameter microspheres) of the left ventricular myocardial microcirculation caused the value of a to remain at approximately 9.5 with embolization up to 501% of the fatal dose of microspheres, but it then decreased progressively with embolization to 4.6 at the fatal dose. Conclusions. We conclude that the FMB/F relation reflects hemodynamic conductance at the microvascular level. (Circulation 1992;85:730-737) ethods for estimating intramyocardial blood volume (expressed as fraction of myocardium that is blood, FMB) are either quite invasive and/or indirect'; hence, it is questionable whether those estimates are representative of the FMB throughout the in vivo heart within a neveropened thorax. Whether FMB reflects microvascular behavior within the intact subject could provide insight into pathophysiological mechanisms affecting the microcirculation. As demonstrated by Kanatsuka et al,2 autoregulation occurs primarily at the < 100-,umdiameter arteriolar level. Hence, arteriolar vasodilation, combined with capillary recruitment,3,4 should manifest as increased intramyocardial blood volume. In this study, we evaluate fast computed tomography M From Beijing Anzhen Hospital (X.-S.W.), Beijing, China; the Department of Electrical and Electronics Engineering (D.L.E.), North Dakota State University, Fargo, N.D.; and the Department of Physiology and Biophysics (E.L.R., Y.-H.L.), Mayo Medical School, Rochester, Minn. Supported in part by research grants HL-04664 and HL-43025, National Institutes of Health, Bethesda, Md. Address for correspondence: Erik L. Ritman, MD, PhD, Mayo Medical School, 200 First Street SW, Rochester, MN 55905. Received March 1, 1991; revision accepted September 17, 1991. (CT) as a relatively noninvasive method for estimating FMB by comparing the magnitudes of estimated intramyocardial blood volume and their changes in response to hemodynamic manipulations against the literature values. We performed this evaluation by changing coronary flow by progressively altering left ventricular work load, by locally constricting the cross-sectional area of a proximal epicardial coronary artery lumen, or by controlled embolization of terminal arterioles with 15 -,m- or 16.5 -am-diameter microspheres. The hypothesis underlying these studies is that maintenance of local myocardial blood flow results from an ischemia-driven hyperemia downstream to a partial obstruction to blood flow (e.g., stenosis or microembolization). Consequently, epicardial coronary stenosis should result in increased FMB in its perfusion territory, whereas microvascular embolization should result in no change in FMB until more than the number of microvessels needed to maintain the perfusion status quo are embolized. Methods Experimental Sequence A total of 48 dogs in five experimental groups were anesthetized with Innovar Vet (0.4 mg fentanyl and Wu et al Intramyocardial Blood Volume by Fast CT Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 20 mg droperidol per milliliter) plus a 2:1 N20-02 gas mixture. The dogs were ventilated with a Harvard pump. All had a No. 8 Rodriques catheter position with its tip in the aortic root for injection of approximately 30 ml iohexol contrast agent. Of these five groups of dogs, groups 2 and 3 were part of other studies by Chung et a15 and Spyra et al,6 respectively. A bipolar catheter was positioned with its tip in the coronary sinus to permit atrial pacing (generally 112 or 120 beats per minute). An additional Rodriques catheter was positioned with its tip in the right atrium for injection of 30 ml iohexol contrast agent. A 6F Millar catheter with a pressure transducer at its tip was positioned in the left ventricular cavity for monitoring left ventricular (LV) pressure. In group 1 (four dogs, weight, 21-26 kg), a balloontipped catheter was positioned in the proximal descending intrathoracic aorta to permit, by balloon inflation, rapid increase of hemodynamic afterload. Infusion of adenosine into the right atrium via the pacing catheter lumen (1 mg/kg/min) was used to cause coronary arterial bed vasodilation while the inflated aortic balloon maintained aortic pressure at the control level. In group 2, 20 dogs (weight, 22-28 kg) were prepared identically to those in group 1. An additional balloon-tipped catheter was positioned in the inferior vena cava to permit, by balloon inflation, rapid decrease of hemodynamic preload. In group 3, 11 dogs (weight, 22-27 kg) had 2-3mm-diameter hollow plastic cylinders embolized, via catheter and guide wire, into a selected proximal epicardial coronary artery.7 The sizes of the cylinders' lumina resulted in stenoses ranging from 25% to 55% of the vessel lumen diameter proximal to the 731 was administered (in seven of the dogs), angiotensin II could be infused (0.01-0.1 ug/kg/min) to maintain aortic pressure at control levels. After catheterization of the animals was completed, each dog was placed supine on a molded cast and positioned in the dynamic spatial reconstructor (DSR) scanner so that the heart was centered in the imaging field. cylinder. DSR Scan Details of the DSR scanner have been described elsewhere.9 Briefly, the DSR scanner consists of a rotatable cylindrical gantry housing 14 x-ray sources positioned in a semicircle. Fourteen video cameras are arranged on the semicircle opposite the x-ray tubes. These cameras record the x-ray projection images on a hemicylindrical fluorescent screen. The projection images, each recorded as 120 horizontal video scan lines on a multichannel video disc recording system, provide input for tomographic images of parallel transverse sections at 0.9-mm intervals over the full cephalocaudal extent of the heart. The analog video signal is digitized and the digital information for the same line of all 14 cameras is simultaneously submitted to a reconstruction algorithm. Computation results in an image of a transverse section at the level of the digitized video lines covering the region of interest. The entire LV is imaged in three dimensions by the stack of parallel transverse sections reconstructed in this manner. Each DSR scan involved sequential pulsing of 14 x-ray sources within 11 msec, and this sequence of exposures was repeated 60 times per second over the 10- or 20-second duration of the scan sequence. X-ray voltage was set at 110 kV, with x-ray current ranging from 500 mA to 800 mA, depending on the size of the dog. In group 4, three dogs (weight, 21-23 kg) had a 4F balloon-tipped catheter positioned in either the proximal left anterior descending coronary artery (LAD) or the left circumflex coronary artery (LCx). The balloon was partially inflated to produce a selected pressure gradient between the aortic root and catheter tip distal to the intracoronary balloon. In group 5, 10 dogs (weight, 21-32 kg) had a 4F catheter tip positioned in the left main coronary artery, proximal LAD, or LCx. Nonradioactive microspheres were injected via this catheter to progressively embolize the myocardial territory perfused by the catheterized vessel. In these dogs, the atrioventricular conduction tissue was previously selectively destroyed with a local injection of -1 ml 34% Formalin under fluoroscopic monitoring by using the needle assembly developed for the percutaneous technique described by Williams et al.8 An additional pacing catheter was positioned in the right ventricle and paced independently from the right atrial pacing catheter so that, if needed, atrial pacing could be performed at twice the ventricular rate to maintain atrial contractions in phase with that of the ventricles. In this group, an additional aortic catheter was positioned so that, after hexamethonium (30 mg/kg) Experimental Protocol In group 1, all dogs were infused with adenosine (1 ml/kg/min in all four; two also had 0.5 ml/kg/min, making a total of six evaluations) during injection of a thorium oxide (one dog) or ethiodol (three dogs) emulsion into the aortic root. The thorium oxide (Electron Microscopy Sciences, Fort Washington, Pa.) and ethiodol (Savage Laboratories, Melville, N.Y.) contrast agents were emulsified in saline by use of a sonication device (Dynatech Laboratories, Inc., Chantilly, Va.): Two milliliters per kilogram were injected over a 3-second period. In group 2, four study sets were performed. Each set involved an aortic root injection of nonionic contrast agent (iohexol, 1 ml/kg) for the estimation of myocardial perfusion and intramyocardial blood volume. The levophase of a right atrial injection of contrast agent was used to provide the LV chamber volume throughout the cardiac cycle and myocardial wall delineation at end diastole, the same timing used for making the myocardial perfusion estimates. These studies were performed under control, elevated aortic pressure, decreased inferior vena caval inflow, and adenosine infusion conditions. 732 Circulation Vol 85, No 2 February 1992 Contrast~injection e! o-rtc : ROP 1 Se Myoar&t RQ 4 tA i. FIGURE 1. Illustration of densitometnc method for generation of indicator dilution curves from fast computed tomography (CT) images showing regions of interest (ROI) over aortic root and myocardium used to estimate the image brightness values from which indicator dilution curve is generated. (Reproduced with permission by E. L. Ritman, Mayo Clin Proc 1990;65:1336-1349.) ... Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 In group 3, a study sequence much as indicated for group 2 was performed with a hollow plastic cylinder in situ under control and under adenosine infusion conditions. In group 4, the study sequences were performed under control conditions and sequential conditions of increasing intracoronary balloon inflation. In group 5, the study sequences were performed under control, adenosine infusion, repeat control, and a sequence of bolus injections of microspheres until ventricular fibrillation occurred. For seven of the 10 dogs, 16.5 -,m-diameter microspheres (Du Pont/New England) were used. In the other three dogs, the first injection into the coronary artery was with the 16.5-gm microspheres, and subsequent injections used 15 -gm latex microspheres (E-Z Trac, Los Angeles, Calif.). The microspheres were prepared according to manufacturers' instructions and were injected slowly into the coronary catheter. Typically, an average of 8.5 million microspheres were injected at a time. Immediately after the injection, the DSR scan was performed. New quantities of microspheres were prepared and administered at 30-45 -minute intervals. This process was repeated until the heart arrested. DSR Data Analysis Details of estimation of myocardial blood flow by analyzing DSR images of the aortic root angiograms were described by Wang et al.1"1 The images generated by each of the 14 television cameras on the DSR scanner were reconstructed into the images of transverse sections (-5-6 mm thick) through the aortic root and at the midventricular level of the LV. The image reconstructions were performed at the enddiastolic phase of all heart cycles throughout the 20-second scanning period. Dye dilution curves of the aortic root and of the myocardium were then generated from the sequence of DSR images (Figure 1). These curves represent the appearance and departure of the contrast agent in the region of the image being measured. Any region (global, transmural, and small pieces) within the image could be selected for measurement. These curves were used to calculate myocardial perfusion (F) in milliliters per gram per minute and FMB expressed as percent of myocardial volume. Nonionic contrast agent has less impact on coronary flow primarily because it has lower osmolality than ionic contrast agents.1' Nonetheless, like ionic contrast agent, up to 15% of the contrast agent enters the extravascular space on the first pass.12 Consequently, the opacification of the myocardium does not return to baseline immediately after the bolus passes through the myocardial circulation.'3 The area under the curve, therefore, would be overestimated. To overcome this problem, we used a mathematical technique developed by Bentley et a114 to correct for this phenomenon in the kidney. To evaluate the validity of this mathematical correction in myocardial perfusion, we studied four dogs (group 1) so that we could compare this mathematically corrected analysis of an iohexol curve with a curve generated from images recorded during injection of a thorium oxide suspension or ethiodol emulsion, which do not enter the extravascular space. This involved two or three injections of contrast agent into the aortic root at 30-minute intervals under very similar hemodynamic conditions. The mathematical technique generates a sigmoidal curve (dash and dot line in middle panel of Figure 2) describing the progressive accumulation of extravascular dye by integrating the arterial input curve (not shown in Figure 2) and scaling the plateau of the resulting sigmoidal curve to equal the value of the original myocardial curve (dashed in middle panel of Figure 2) when it settles at a stable, abovebaseline value. This sigmoidal curve is then subtracted from the original myocardial curve to gener- Wu et al Intramyocardial Blood Volume by Fast CT 733 space is illustrated in Figure 2. When the original (upper panel) was used to compute FMB, a value of 26.8% was obtained. If the computed curve (middle panel) is used, an FMB value of 20.2% results. This latter result compares closely with the value of 20.0% obtained from the thorium oxide Nonionic Contrast Agent curve (0) CJ) suspension curve (lower panel). The results from the four dogs (group 1) studied to evaluate the reproducibility and accuracy of this approach for estimating FMB are summarized by two regression equations describing the linear leastsquares best fit to the totally intravascular (ethiodol or thorium, Y%) and partially extravascular (iohexol, X%) contrast agent-based estimates of FMB. When the fact that some iohexol remains in the extravascular space is ignored, the regression equation is Y=0.74X+5.26, r=0.951, whereas, when the Bentley method is used to correct for that extravascular component, Y=0.98X+3.70, r=0.946. The intercept 3.70 is not distinguishable from zero at the level of p=0.05. Because of the near 1:1 slope of the Bentley method, all our dilution curves were analyzed using this mathematical correction for loss of contrast to the extravascular space. In group 2, the aortogram image data were used to estimate the transmural intramyocardial blood volume and flow under different hemodynamic loading situations without abnormal coronary circulation. As shown in Figure 3, it was observed that the intramyocardial blood volume relates curvilinearly to myocardial perfusion in that region. The curve FMB=a . F`12 fits the data points fairly well at flows higher than 0.8 ml/g/min. The magnitudes of the average (+SD) a were 9.5+1.2% and 9.6+1.1% (milliliters times minutes per gram)'/2 for the subendocardial third and the subepicardial third of the wall, respectively. Although other analytic curves may have a better statistical fit to all the data points, we use the square root relation for reasons detailed in the "Discussion." That heart rate impacts on the transmural Curve (O-C) (k :t FMB 20.2% Original Curve 11 1 (0) ,5t Cm \\\X l Computed Extravascular N \ " Curve (C) Thorium Oxide Suspension Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 FMB 20.0 % Original Curve TIME FIGURE 2. Schemes of contrast dilution curves generated by passage ofthorium oxide suspension and by iohexol injected to aortic root for calculation of intramyocardial blood volume (FMB) and flow. Upper panel derived from contrast of iohexol, which partially enters the extravascular space; lower panel fiom thorium oxide, which remains intravascular. ate the intravascular curve (solid line in middle panel of Figure 2), which is the curve of interest for our FMB and F calculations. Results One example of the mathematical technique used to correct for loss of iohexol to the extravascular 30 Subepicordium 30 Subendocardium * _ °20 * 20 * 4D 0 P- 9.5 x 112 C) o to I O 2 4 6 8 0 2 4 6 8 FLOW (mL/g/min) FIGURE 3. Scatterplots show curvilinear relations between intramyocardial blood volume (FMB) and flow (F) in subendocardium and subepicardium. Solid curves are the least-squares best fit of formula FMB =a *F"P2 to the experimental data points. Circulation Vol 85, No 2 February 1992 734 12 P<.05 12 12 l* # 12 * .It E .E to E IN. i -4 1O to ,c 10,1 8 IE 8 -4 11.. 10 _ 8_ N 3 Meon ± SD _ C NS IL 6 E k 6 _ 4 4 _ IN * = ** = 2_ r| T i- I 2 9 1 * a 0 0 2 r-- I *- 4 e *P<0*0 Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 0 25-43 50-55 CORONARY DIAMETER STENOSIS (%) myocardial blood volume and perfusion distribution was illustrated in one anesthetized dog. In the control (resting) state, the endocardial/epicardial ratios of F and FMB at 72 beats per minute were 1.6 and 1.5, respectively, and fell to 0.94 and 0.92 at a heart rate of 112 beats per minute. In maximum vasodilation with adenosine, the endocardial/epicardial ratios of F and FMB at 72 beats per minute were 0.86 and 0.89, respectively, and fell to 0.81 and 0.85 when heart rate increased to 112 beats per minute. In group 3, each region of interest was identified as one of three categories: a control region, a region perfused by a 25-43%, or by a 50-55% stenosed artery. The average myocardial F and FMB of each group is shown in Figure 4. The flow was not decreased under control conditions; however, the FMB/F relation increased significantly in territories perfused by stenosed vessels with values of a= 9.1+0.7 for no stenoses, 10.1+0.9 for 25-43% stenoses, and 11.1+0.9 for 50-55% stenoses, respectively. There is a significant difference (p<0.01) between any two values. In group 4, flow started to decrease (see Figure 5) at a pressure gradient across the coronary narrowing (due to partial inflation of intracoronary balloon) greater than 40 mm Hg, but the value of a was already significantly (p<0.01) elevated when the pressure gradient was greater than 9 mm Hg. 0 PcO.OOt5 0 Ui FIGURE 4. Graph shows myocardial perfusion characteristics from dogs with/without intracoronary hollow plug, which show the role of coronaty stenosis. The value of a was obtained from the least-squares best fit of formula FMB= a *Fl2 (FMB, intramyocardial blood volume; F, flow) to the experimental data points for all dogs' regions perfused by the indicated percent stenosis. The value a (i.e., FMB at flow =1 mlIg/min) increased gradually but significantly in the temritory perfused by a coronary artery with 24-43% or 50 -55% stenosis. .1 p<0.o01 NS .- l-.I P<O.05 P<o.of 0 -4 42.. 0 0 6 -4IE Compared toAP=0 1au -L_ 9 40 85 112 A P ACROSS CORONARY NARROWING (mm Hg) FIGURE 5. Graph shows myocardial perfusion characteristics in dogs with an intracoronary balloon. In resting state, the value at a (intramyocardial blood volume at flow=] ml/g/ min) increased significantly at moderate narrowing (pressure gradient, AP, across balloon -40 mm Hg), whereas flow was impaired only at more severe narrowing (AP -85 mm Hg). However, flow relative to myocardium perfused by a nonstenosed vessel decreased significantly at moderate narrowing with maximum vasodilation (not shown). FMB, intramyocardial blood volume. In group 5, progressive embolization of the myocardial microcirculation obtained by sequential coronary injections of microspheres induced the modulation of FMB and F as shown in Figure 6. Both FMB and F 12 NS NS 12 Pc0.05 PcO.05 PcO.001 ~~~~~~~~1 i Mwn±FSD 10 E 4-.c_ Ik. ,c 6 to , E Lat. 4 ° ik 06 NS IT 1UL NS P<aOOO NS P'O.OO1 2 L~~ a 0 1-25 26-50 51-75 76-9 100 PERCENT OF FATAL#&SPHERE DOSE ' M% FIGURE 6. Graph shows effect of microsphere embolization on modulation of intramyocardial blood volume (FMB) and perfusion. Both the value of a (FMB at F=] ml/g/min) and flow (F) decreased gradually but significantly in the teritory perfused by a vessel with more than 50% offatal microsphere dose. Wu et al Intramyocardial Blood Volume by Fast CT 20 1.4 0 0 t 15 0 0.0 * 0 S (0 -50% of FatoPIDose) , JO _ * >,<y=9.6=9.x"t1 0 1U P<0a01 7fx "2 P'0O05 ~~~y= (75-99%) 1X * 5 92 0 4.6x" yz P<.001 (100%) U I 0 05 . I 1.0 * . 2.0 1.5 FLOW (mL/g/min) 2.5 Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 FIGURE 7. Plot shows that intramyocardial btlood volume (FMB) to flow (F) relation remained unch tanged, with FMB=9.6 FPI2, until more than 50% of a fi;atal dose of microspheres was embolized into the coronary ci, rculation. As the fatal dose was approached, the relation's ,value of a decreased progressively. decreased significantly in the range of 51-7 5% of fatal dose of microspheres. However, as shown in Figure 7, the FMB to F relation in the 0-50% of fatal dose group remained indistinguishable from that in gr(Dup 2. Discussion Previous studies confirmed that the myocardial perfusion estimated by CT relates linearily to perfusion estimated by the generally accepted radioactive microsphere method.10"15,16 We are quite (encouraged about our dye dilution-based estimates o Ifintramyocardial blood content because our data arev consistent with values in the literature,1"17-19 which range from 5% to 27% with most values ranging fr( )m 10% to 20% (several authors used ml/100 g LV)). That our fast CT estimates of FMB and F are comsistent with those presented by investigators using other methods is illustrated in Table 1. Although we have no direct head-to-he;ad comparison of the CT-based method and other generally more invasive methods, an additional cir(cumstantial confirmation of the validity (or at least nneaning) of the FMB is that it is consistent with Poisezuille's law. This law predicts that vascular flow (F) is proportional to AP R4/L, where R is the radius of a vessel 735 lumen and AP is the pressure gradient along vessel of length L. If we assume that the volume (V) of the intramyocardial vessels is proportional to LR' and if L remains essentially unchanged with vasomotion and recruitment, it then follows that F oAP* V2. Thus, if AP remains essentially constant (which we attempted to do by maintaining aortic pressure at control levels with the aortic balloon inflation), we expect Vo F"', which, if we equate FMB with V, is what we observe. A decrease of vascular resistance in acutely ischemic myocardium is well documented. A possible mechanism is described by the adenosine hypotheSiS,20 which states that ischemia results in accumulation of adenosine, which in turn leads to vasodilation, which would in turn tend to reverse ischemia because of the resulting increase in perfusion. This hypothesis is based in part sure the assumption that normal blood flow is maintained by the resulting increased gradient increased by downstream across the stenosis. This gradient is dropping to the intra-arterial the stenosis by further opening of the vascular beds. This opening of the vascular beds should manifest as increase in intramyocardial blood volume to a level higher than expected for the flow. Our data, therefore, support the hypothesis that distal to an epicardial coronary artery stenosis, there should be an increase in blood volume reflecting the vasodilation. With stenosis causing a pressure drop across the stenosis greater than 40 mm Hg, we observed a slight progressive decrease in FMB an observation that is consistent with the observations of Kanatsuka et al,2 who found that despite dilation of the <100-,um vessels during ischemia, the larger vessels constricted. The data from this present study are consistent with the flow reserve phenomenon, but, as indicated in Figures 4 and 5, also suggest that the FMB-to-flow relation is a possibly more sensitive index of the hemodynamic impact of a mild coronary artery stenosis than is the flow reserve index.21 Thus, for a stenosis less than 55% or generating a pressure gradient less than 40 mm Hg, there is no discernible change in blood flow, but at a stenosis of 25% or generating a pressure gradient of 9 mm Hg, there is a discernible increase in FMB. The effect of microsphere embolization indicates that absolute value of FMB decreased during injection of a cumulative microsphere dose equal to and TABLE 1. Intramyocardial Blood Volume and Percent of Myocardial Volume Comment Reference Value (%) Animal Radioactive tagging of RBC and/or plasma 25-27 7-26 Rat Radioactive tagging of RBC and/or plasma 8-10 Swine 28,29 Radioactive tagging of RBC and/or plasma 6-10 Dog 30,31 Mean indicator transit time 11-17.8 Dog 1,32 24 Ultrasonic measurement of wall thickness 10-20 Dog Left ventricular hypertrophy 33 27 Dog RBC, red blood cells. - 736 Circulation Vol 85, No 2 February 1992 greater than 50% fatal dose, beyond which dose the FMB (under control conditions) progressively diminishes. We observed that the value of a was 4.6 just before cardiac arrest. This could mean that, under control hemodynamic conditions, approximately half (i.e., 4.6/9.5) of control FMB is available when the heart ceases to function. The number of microspheres required to arrest the heart (2.5 x 105/g) matches those needed (5 x 105/g) by Hori et al,22 who injected 15-,um microspheres selectively into the LAD of open-chest dogs that were treated with prazosin, a postsynaptic a-blocker, but aortic pressure was not maintained at control levels. Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Summary The magnitude of the FMB, estimated by fast CT, behaves quantitatively like the invasively measured microvascular volume as reported in the literature. Second, this volume has a predictable relation to myocardial perfusion. Because this relation is independent of the location within the heart wall, the observed spatial heterogeneity of blood flow is most likely due to the heterogeneity of blood volume. Local blood volume appears to be strongly driven by local perfusion needs as illustrated by increase of blood volume beyond a coronary stenosis and by the steady blood volume up to a 50% fatal-dose embolization of the myocardial microcirculation. This observation is quite consistent with the recent direct observations3,23 of epicardial arterioles that suggest that the bulk of autoregulation occurs at the microvascular level. Acknowledgments The authors wish to thank Don Erdman and his colleagues for their help with the preparation of the animals and DSR scans. Christine Welch made the illustrations, and Marissa Miller typed the manuscript. References 1. Morgenstern C, Holjes U, Arnold G, Lochner W: The influence of coronary pressure and coronary flow on intracoronary blood volume and geometry of the left ventricle. Pflugers Arch 1973;340:101-111 2. Kanatsuka H, Lamping KG, Eastham CL, Marcus ML: Heterogeneous changes in epimyocardial microvascular size during graded coronary stenosis. Circ Res 1990;60:389-396 3. Rose CP, Goresky CA: Vasomotor control of capillary transit time heterogeneity in the canine circulation. Circ Res 1976;39: 541-554 4. King RB, Bassingthwaighte JB, Hales JPS, Rowell LB: Stability of heterogeneity of myocardial blood flow in normal awake baboons. Circ Res 1985;57:285-295 5. Chung N, Wu X, Bailey KR, Ritman EL: LV pressure-volume area and oxygen consumption: Evaluation in intact dog by fast CT. Am J Physiol 1990;258(Heart Circ Physiol 27):H1208H1215 6. Spyra WJT, Bell MR, Bahn RC, Zinsmeister AR, Ritman EL, Bove AA: Detection of mild coronary stenoses using the dynamic spatial reconstructor. Invest Radiol 1990;25:472-479 7. Gewirtz H, Most AS: Production of a critical coronary arterial stenosis in closed chest laboratory animals. Am J Cardiol 1981;47:589-596 8. Williams JC, Lambert EH, Titus JL: Use of intracardial A-V nodal potentials in producing complete heart block in dogs. JAppi Physiol 1969;27:740-744 9. Ritman EL, Robb RA, Harris LD: Imaging Physiological Functions: Experience With the Dynamic Spatial Reconstructor. Philadelphia, Praeger, 1985, p 302 10. Wang T, Wu X-S, Chung N, Ritman EL: Myocardial blood flow estimated by synchronous, multislice, high-speed computed tomography. IEEE Trans Med Imaging 1989;8:70-77 11. Higgins CB: Cardiotolerance of lohexol, survey of experimental evidence. Invest Radiol 1985;20(suppl):S65-S69 12. Whitaker JW, Tancredi RG, Yipintsoi T, Donald D: Myocardial transport of diatrizoate meglumine (abstract). Physiologist 1980;23:6 13. Canty JM Jr, Judd RM, Brody AS, Klocke FJ: Extravascular contrast loss significantly overestimates fast CT measurements of intramyocardial blood volume (abstract). Circulation 1990; 82(suppl III):III-125 14. Bentley MD, Lerman LO, Hoffman EA, Fiksen-Olsen JJ, Ritman EL, Romero JC: In vivo measurement of renal blood flow (RBF) with dynamic CT (abstract). Physiologist 1989;32: 208 15. Gould RG, Lipton MJ, McNamara MT, Sievers RE, Koshold S, Higgins CB: Measurement of regional myocardial blood flow in dogs by ultrafast CT. Invest Radiol 1988;23:348-353 16. Rumberger JA, Feiring AJ, Lipton MJ, Higgins CB, Ell SR, Marcus ML: Use of ultrafast computed tomography to quantitate regional myocardial perfusion: A preliminary report. J Am Coll Cardiol 1987;9:59-69 17. Feigl EO: Coronary physiology. Physiol Rev 1983;63:1-2053 18. Crystal GJ, Downey HF, Bashour FA: Small vessel and total coronary blood volume during intracoronary adenosine. Am J Physiol 1981;241(Heart Circ Physiol 10):H194-H201 19. Salisbury PF, Cross CE, Rieben PA: Physiological factors influencing coronary blood volume in isolated dog hearts. Am JPhysiol 1961;200:633-636 20. Berne RM: The role of adenosine in the regulation of coronary blood flow. Circ Res 1980;47:808-813 21. McGinn AL, White CW, Wilson FR: Interstudy variability of coronary flow reserve: Influence of heart rate, arterial pressure, and ventricular preload. Circulation 1990;81:1319-1330 22. Hori M, Tamai J, Kitakaze M, Ivalwa K, Gotoh K, Iwai K, Koretsune Y, Kagiya T, Kitababahe A, Kamada T: Adenosineinduced hyperemia attenuates myocardial ischemia in coronary microembolization in dogs. Am J Physiol 1989;257(Heart Circ Physiol 16):H244-H251 23. Dellsperger KC, Jahzen JL, Eastham CL, Marcus ML: Effects of acute coronary artery occlusion on the coronary microcirculation. Am J Physiol 1990;259(Heart Circ Physiol 28): H909-H916 24. Gaasch WH, Bing OHL, Franklin A, Rhodes 0, Bernard SA, Weintraub RM: The influence of acute alterations in coronary blood flow on left ventricular diastolic compliance and wall thickness. Eur J Cardiol 1981;7(suppl):147-161 25. Everett NB, Simmons B, Lasher EP: Distribution of blood (Fe59) and plasma (1131) volumes of rats determined by liquid nitrogen freezing. Circ Res 1956;4:419-424 26. Gibson JGH, Seligman AM, Peacock WC, Aub JC, Fine J, Evans RD: The distribution of red cells and plasma in large and minute vessels of the normal dog, determined by radioactive isotopes of iron and iodine. J Clin Invest 1946;25: 848-857 27. Rakusan K, Wachtlova M, Poupa 0: An attempt to determine indirectly the vascularity of heart muscle by measuring the tissue concentration of haemoglobin in normal and anaemic rats. Physiol Bohemoslov 1969;18:1-5 28. Howe BB, Winbury MM: Effect of acute coronary occlusion on myocardial nutritional circulation in swine. Am J Physiol 1969;216:1069-1074 29. Winbury MM, Losada M, Kessel D, Howe BB, Pensinger RR: Pentaethyritoltetranitrate and dipyridamole on cardiac nutritive flow and blood content. Am J Physiol 1971;220:1558-1563 30. Howe BB, Windbury MM: Effect of pentrinitrol, nitroglycerin and propanolol on small-vessel blood content of canine myocardium. J Phannacol Exp Ther 1973;187:465-474 Wu et al Intramyocardial Blood Volume by Fast CT 31. Weiss HR, Windbury MM: Nitroglycerin and chromonar on small-vessel blood content of the ventricular walls. Am J Physiol 1974;226:838-843 32. Hirsch EF, Lochner W: Messung der Durchblutung und der Blutftillung des coronaren Gefassbettes mit der Testoffinjection Methode am narkotisierten Hund bei geschlossem Thorax. Pflugers Arch 1962;274:624-632 737 33. O'Keefe DO, Hoffman JIE, Cheitlin R, O'Neill MJ, Allard JR, Shapkin E: Coronary blood flow in experimental canine left ventricular hypertrophy. Circ Res 1978;49:342-353 KEY WORDS * coronary stenosis * embolization * fast CT microcirculation . Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 In vivo relation of intramyocardial blood volume to myocardial perfusion. Evidence supporting microvascular site for autoregulation. X S Wu, D L Ewert, Y H Liu and E L Ritman Downloaded from http://circ.ahajournals.org/ by guest on June 11, 2017 Circulation. 1992;85:730-737 doi: 10.1161/01.CIR.85.2.730 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1992 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/85/2/730 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/