Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
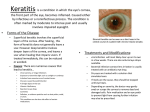
Pediatric Infectious Keratitis at Tertiary Referral Centers in Vancouver, British Columbia Gelareh S. Noureddin, MD, Sachiko Sasaki, MD, Andrea L. Butler, MD, Christopher J. Lyons, MD FRCSC, Simon P. Holland, MD FRCSC, Sonia N. Yeung, MD PhD FRCSC The authors have no financial interests to disclose. Introduction • Microbial keratitis is a potentially sight-threatening condition. • In children, it may lead to amblyopia secondary to corneal scarring. • Prompt and effective treatment results in better visual outcomes. • Regional patterns of infection and antibiotic sensitivity are helpful in making treatment decisions. Purpose • To report the clinical and microbiological profiles of pediatric patients with infectious keratitis requiring corneal scraping for diagnosis in Vancouver, British Columbia (a moderate oceanic climate) Methods • Observational case series • Microbiology results and medical records of 17 eyes with microbial keratitis in 16 children aged 17 years or younger were retrospectively reviewed. • All patients had corneal scraping performed between May 2006 and April 2011. Results: Demographics and Clinical Features • 17 corneal scrapings in 16 children – One child with Stevens-Johnson Syndrome (SJS) developed a second corneal ulcer during the study period; both ulcers have been included. • Mean age: 11 ±5.7 years (range 1-17) • Ulcers most commonly large (>4mm) and mid- peripheral in location • Most common presenting symptom was pain (65%) Results: Predisposing Factors • 9/17 cases had pre-existing ocular surface condition – Blepharokeratoconjunctivitis (BKC); n=3 – Stevens-Johnson (SJS); n=3 – Complex ocular history with previous surgery; n=3 • 6/17 cases related to contact lens wear • 1 case foreign body • 1 case previous HSV keratitis Results: Microbiology Microorganism Incidence Gram Positive Bacteria Gram Negative Bacteria Fungus Parasite Culture negative Polymicrobial Microorganism CL Wearer Non-CL Wearer Bacillus 1 Coagulase-negative S. epidermidis 1 4 Corynebacterium 1 1 S. pneumoniae 1 S. viridans 1 1 H. influenzae 1 P. aeruginosa 2 Aspergillus fumigatus 1 Acanthamoeba 4 4 2 2 Results: Antibiotic Sensitivity Antibiotic Susceptibilities and Resistance Class Antibiotic Ciprofloxacin Levofloxacin Fluoroquinolone Moxifloxacin Ofloxacin Glycopeptide Vancomycin Gentamicin Aminoglycoside Tobramycin Amphenicol Chloramphenicol Susceptibility Gram +ve Gram -ve 2 2 1 2 3 2 7 4 2 3 2 5 1 Resistance Gram +ve Gram -ve 1 1 1 Results: Outcome • Visual acuity ≥20/60 in 9/16 patients = 56% • 3 patients required subsequent surgery for corneal scarring: – 2x penetrating keratoplasty – 1x DALK Discussion • Most common isolate was coagulase negative S. epidermidis; similar to other studies • Acanthamoeba in 4/6 contact lens wearers – Related to use of contact lens solution later recalled by FDA in 2007 • Pseudomonas in 2/6 contact lens wearers – Important to ensure antibiotic coverage in CL keratitis Conclusion • Contact lens wear and pre-existing ocular surface conditions are important risk factors for the development of infectious keratitis in our population. • Knowledge of regional patterns of infection and antibiotic sensitivity/resistance allow for effective management and better visual outcomes for children. • We recommend other groups perform profiling of this condition in their respective localities. References 1. Zaidman G. The pediatric corneal infiltrate. Current Opinion in Ophthalmology. 2011;22:261–266. 2. Ameet S, Sachdev A, et al. Geographic variations in microbial keratitis: an analysis of the peer-reviewed literature. Br J Ophthalmol. 2011;95:762-767. 3. Lisa AJ, Walline JJ, et al. Purchase of contact lenses and contact-lenses-related symptoms following the Contact Lenses in Pediatrics (CLIP) Study. Contact Lens & Anterior Eye. 2009;32:157– 163 4.Wagner H, Chalmers RL, et al. Risk Factors for Interruption to Soft Contact Lens Wear in Children and Young Adults. Optometry and Vision Science. 2011; Vol. 88, No. 8. 5. Al Otaibi AG, Allam K. Childhood microbial keratitis. Oman Journal of Ophthalmology. 2012; Vol. 5, No. 1. 6. Singh G, Palanisamy M. Multivariate Analysis of Childhood Microbial Keratitis in South India. Ann Acad Med Singapore. 2006;35:185-9 7. Hsiao CH, Yeung L, et al. Pediatric Microbial Keratitis in Taiwanese Children A Review of Hospital Cases. Arch Ophthalmol. 2007; Vol. 125. 8. Wong VWY, Lai TYY, et al. Pediatric Ocular Surface Infections: A 5-year Review of Demographics, Clinical Features, Risk Factors, Microbiological Results, and Treatment. Cornea. 2011; Vol. 30, No. 9. 9. Song X, Xu L, et al. Pediatric microbial keratitis: a tertiary hospital study. Eur J Ophthalmol. 2011;22(2) 136-141. 10. KM Holland. Cornea 3rd edition, Chapter 77, 919. 11. Al-Otaibi AG. Non-viral microbial keratitis in children. Saudi Journal of Ophthalmology. 2012;26:191–197. 12. Fraser MN, Wong Q, et al. Characteristics of an Acanthamoeba Keratitis Outbreak in British Columbia between 2003 and 2007. Ophthalmology. 2012;119:1120–1125. 13. Butler AL, Sasaki S, et al, Epidemiology of infectious corneal ulcers in Vancouver, BC. The Canadian ophthalmology meeting 2012, Toronto, Canada. 14. Stapleton F. Keay LJ. et al. Relationship Between Climate, Disease Severity, and Causative Organism for Contact Lens–Associated Microbial Keratitis in Australia, Am J Ophthalmol 2007;144:690–698. 15. Stapleton F, Carnt N. Contact lens-related microbial keratitis: how have epidemiology and genetics helped us with pathogenesis and prophylaxis. Eye. 2012;26:185–193. 16. Hammersmith KM, Cohen EJ, et al. Blepharokeratoconjunctivitis in Children. Arch Ophthalmol. 2005;123:1667-1670. 17. Jones SM, Nischal KK, et al. Visual Outcome and Corneal Changes in Children with Chronic Blepharokeratoconjunctivitis. Ophthalmology. 2007;114:2271–2280. 18.Ormerod LD, Murphree AL, Gomez DS, Schanzlin DJ, Smith RE. Microbial keratitis in children. Ophthalmology. 1986;93:449-455. 19. Cruz OA, Sabir SM, Capo H, Alfonso EC. Microbial keratitis in childhood. Ophthalmology. 1993;100:192-196. 20. Clinch TE, Plamon FE, Robinson MJ, Cohen EJ, Barron BA, Laibson PR. Microbial keratitis in children. Am J Ophthalmol. 1994;117:65-71. 21. Di Pascuale MA, Espana EM, Liu DT. Correlation of Corneal Complications with Eyelid Cicatricial Pathologies in Patients with Stevens–Johnson Syndrome and Toxic Epidermal Necrolysis Syndrome. Ophthalmology. 2005;112:904–912. 22. Keay LJ, Gower EW, Lovieno A. Clinical and Microbiological Characteristics of Fungal Keratitis in the United States, 2001–2007: A Multicenter Study. Ophthalmology. 2011;118:920–926. 23. Schultz DG. (2007, May 31). FDA Preliminary Public Health Notification: Acanthamoeba Keratitis Infections Potentially Related to Complete MoisturePlus Multipurpose Contact Lens Solution Manufactured by Advanced Medical Optics (AMO). Retrieved from http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/PublicHealthNotifications/ucm062063.htm.