Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
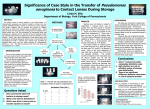
A Presentation of Pseudomonas aeruginosa Keratitis Secondary to Contact Lens Overwear Stephanie M. Sloan, OD Abstract Microbial Keratitis due to contact lens overwear can be a serious vision threatening condition. We present a case involving the central cornea which was found to be secondary to Pseudomonas aeruginosa. I. Case History - 54 y.o. African American female - Sudden, worsening pain with yellow discharge and extreme photophobia OS x 3 days - Ocular/Medical Hx: contact lens related red eye – unknown diagnosis, breast cancer - Meds: ibuprofen, visine; NKDA - “trial period” for contact lenses, 2 week lens, current pair 3-4 weeks old, sleeps in lenses, h/o swimming in lenses but hasn’t for over 2 months, using unknown generic contact lens solution II. Pertinent findings - BCVA: 20/20 OD, 1/400 – PH: NI OS - SLE (photos): OS: 3+ lid edema c thickened margins, lashes matted together, 4+ conjunctival injection, 4+ chemosis, 2.4mmx2.7mm central ulcer c infiltrate, discharge, peripheral corneal neovascularization 360, 1.8mm hypopyon, 4+ cell, 2+ flare - IOP: deferred 2’ corneal pathology - DFE: no view 2’ corneal pathology - Pt referred same day to Corneal Specialist for corneal culture - Laboratory studies: eye culture and stain, acanthamoeba culture and stain, eye fungal culture - Results: moderate Pseudomonas aeruginosa, few Staphylococcus epidermidis III. Differential diagnosis - Bacterial keratitis - Acanthomeba keratitis - Herpes Simplex Virus keratitis IV. Diagnosis and discussion: - Diagnosis: Bacterial Keratitis secondary to Pseudomonas aeruginosa - Pseudomonas aeruginosa is a virulent and rapidly progressing Gram-negative bacterium that can be found in soil and water - Produces proteases which invade or kill corneal cells - Coordinate expression of virulence factors - Activate immune system pathways via toll-like receptors (TLRs) which consequently causes continued destruction - P. aeruginosa has a more severe presentation when compared to a cohort of microbial keratitis - Large and deep infiltrate - Significant decrease in visual acuity - Suppurative - Associated hypopyon - 30,000 cases of microbial keratitis in the US every year - P. aeruginosa responsible for up to 39% of microbial keratitis cases in the US - 3-5 per 10,000 contact lens wearers per year affected - Low Dk contact lenses can cause corneal hypoxia which can be exacerbated under closed-eye conditions - Reduced epithelial cell turnover with contact lens wear creates opportunity for infection V. Treatment, management - Vision threatening, severe keratitis - Deep stromal involvement or infiltrate larger than 2mm with extensive suppuration - Fluoroquinolone loading dose after obtaining culture - Every 5-15 minutes for the first 30-60 minutes, then, every 30-60 minutes for 24 hours - Cycloplegic agent to decrease synechia formation and pain - Fortified tobramycin or gentamicin (15mg/mL) q1hr altered with fortified cefazolin (50mg/mL) or vancomycin (25mg/mL) q1hr - Taper antibiotics as directed, based on clinical situation - Adjunct corticosteroid recommended when infection is controlled - Potentially decrease scarring - SCUT trial - Contact lens wear must be discontinued - Systemic antibiotics necessary if adjacent tissues become infected or impending or frank perforation of the cornea is evident - Follow-up examinations performed daily unless hospitalization is required due to concern for noncompliance or need for intravenous antibiotics - This patient was cultured and then empirically treated with tobramycin 1.53% q2hr OS which was alternated every hour with vancomycin 5% q2hr OS, as well as cyclopentolate 1% BID OS. - Medications then altered after pathology confirmation of Pseudomonas aeruginosa - Fortified tobramycin 1.53% q2hr OS, ciprofloxacin gtts q2hr OS and ung qhs OS, cyclopentolate BID OS - Antibiotics tapered as infection resolved - Pred Forte TID OS added 2 weeks after initial onset VI. Conclusion - Understanding the array of clinical presentations of microbial keratitis increases effectiveness of empirical treatment and management - The incidence of microbial keratitis can be minimized with increased patient education of risk factors and preventative measures - Bibliography - American Academy of Ophthalmology Cornea/External Disease Panel. Preferred Practice Pattern Guidelines. Bacterial Keratitis. San Francisco, CA: American Academy of Ophthalmology; 2013. Available at: www.aao.org/prp. - Ray KJ, Srinivasan M, Mascarenhas J, Rajaraman R, Ravindran M, Glidden DV, Oldenburg CE, Sun CQ, Zegans ME, McLeod SD, Acharya NR, Lietman TM. “Early addition of topical corticosteroids in the treatment of bacterial keratitis.” JAMA Ophthalmol. 2014 Jun;132(6):737-41. doi: 10.1001/jamaophthalmol.2014.292. PubMed - Schornack, Muriel M., OD, Lisa J. Faia, MD, and Gregory J. Griepentrog, MD. "Pseudomonas Keratitis Associated With Daily Wear of Silicone Hydrogel Contact Lenses." Eye & Contact Lens 34.2 (2008): 124-28. - Srinivasan M, Mascarenhas J, Rajaraman R, Ravindran M, Lalitha P, Glidden DV, Ray KJ, Hong KC, Oldenburg CE, Lee SM, Zegans ME, McLeod SD, Lietman TM, Acharya NR; Steroids for Corneal Ulcers Trial Group. “Corticosteroids for bacterial keratitis: the Steroids for Corneal Ulcers Trial (SCUT).” Arch Ophthalmol. 2012 Feb;130(2):143-50. doi: 10.1001/archophthalmol.2011.315. Epub 2011 Oct 10. PubMed. - Stapleton, Fiona, PhD, Katie Edwards, PhD, Lisa Keay, PhD, Thomas Naduvilath, PhD, John K. Dart, DM, Garry Brian, and Brien Holden, DSc. "Risk Factors for Moderate and Severe Microbial Keratitis in Daily Wear Contact Lens Users." American Academy of Ophthalmology 119 (2012): 1516-521. - Willcox, Mark D., PhD. "Pseudomonas Aeruginosa Infection and Inflammation During Contact Lens Wear: A Review." Optometry and Vision Science 84.4 (2007): 273-78.