Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
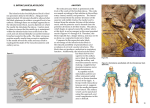
Infraclavicular Brachial Plexus Block The infraclavicular approach blocks the brachial plexus at the level of the cords (medial, lateral and posterior) in the infraclavicular fossa. This is a good approach to place a catheter for post operative pain control. Indication: Surgeries involving the humerus, elbow, forearm and wrist. Anatomy: The boundaries of the infraclavicular fossa are: Anteriorly the pectoralis major and minor muscles Medially the thorax Superiorly the clavicle and coracoid process Laterally the humerus. Note: The plexus is approached in close proximity to the coracoid process. Raj Approach Position: Supine with the head turned to contralateral side and the arm abducted to 90°. The anesthesiologist can either stand on the side opposite that to be blocked or at the head of the bed. Needle: 22G 100 mm insulated needle or Tuohy needle for ultrasound guided procedures Procedure: Locate the mid point of the clavicle (between the sternal and the acromial ends) Mark a point 2.5cm below the clavicle. Find the axillary artery at its highest point in the axilla and mark it on the pectoralis major muscle. After appropriate skin prep raise a wheal of local anesthetic 2.5cm below the mid clavicular point. Insert the needle at an angle of 45 - 60° to the sagittal plane directed away from the rib cage toward the axillary artery. At a depth of 1 – 3cm depth note the contraction of the pectoralis major muscle. The plexus is usually located at a depth of 3 – 7cm. The ideal evoked response is hand movement at < 0.3mA. Inject 30 – 50mL of local anesthetic. If no motor response can be elicited progressive needle redirection to 80° will yield a response. Comments: Contractions of the musculocutaneous nerve (biceps) or axillary nerve (deltoid) must be rejected since they are located outside the sheath at this level. The needle should not be directed medially toward the rib cage (pneumothorax). This is a painful block since the needle traverses a large muscle mass. Infiltrate local anesthetic well and deep, and sedate the patient accordingly. There is a risk of axillary artery hematoma with this approach since it is difficult to apply manual pressure. Be cautious in patients with potential for bleeding problems.