Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
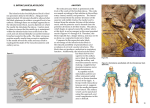
Infraclavicular block Written by Dr Khalid Syeed Anatomy The boundaries of the infraclavicular fossa are the pectoralis minor and major muscles anteriorly, ribs medially, clavicle and coracoid process superiorly and humerus laterally. Posterior to the brachial plexus in this region is the scapula. At this location, the brachial plexus is composed of cords, which are arranged around the second part of the axillary artery. The sheath surrounding the plexus is delicate and contains the subclavian/axillary artery and vein. The axillary vein is commonly located caudad and medial to the axillary artery. The axillary and musculocutaneous nerves leave the sheath at or before the coracoid process in 50% of patients. The plexus, which begins to spread around the axillary artery at this level, is not as compact as the more proximal trunks. Therefore, this block typically has longer latency, and may not be as dense as a supraclavicular nerve block. The infraclavicular nerve block was first described by Raj et al in 1973. A number of approaches have since been described but only 2 seem to have stood the test of time – the sub coracoid approach and the vertical infraclavicular block. The sub coracoid infraclavicular block is well suited for ultrasound guided local anaesthetic placement. This intermediate technique block approaches the brachial plexus at a level above the departure of the axillary and musculocutaneous nerves, thus providing “whole arm” anaesthesia without the need for additional, more distal, nerve blocks. Indications Surgery of the elbow, forearm, wrist and hand. Territories blocked At the level of the cords-Immediately medial to the coracoid process, the lateral cord of the plexus lies superior and lateral, the posterior cord lies posterior and the medial cord lies posterior and medial to the axillary artery. The Intercostobrachial nerve(T2) courses adjacent to the brachial plexus at the level of the cords. The infraclavicular block will usually produce analgesia in this nerve to cover the majority of tourniquet pain. Equipment • • • 8-10MHz linear probe + ultrasound machine Sterile probe cover 22G 50mm nerve block needle Local anaesthesia Volume between 20-30 mls, taking care not to exceed the toxic dose. The lowest volume that has been reportedly used is 14 mls. Approach Both in plane and out of plane approaches have been described Place the patient supine with arms at the side. After skin and transducer preparation, place the 8-10 Mhz linear probe immediately medial to the coracoid process, underneath the clavicle in a parasagittal plane. This allows us to obtain the best possible transverse view of the axillary vessels and cords. Optimize machine imaging capability by selecting the appropriate depth of field (usually within 3-5 cm), focus range and gain. Perform a systematic anatomical survey from superficial to deep. The most superficial structures noted are the pectoralis muscles-major and minor. Move the transducer cephalad to identify the clavicle and medially to identify the coracoid process. Identify the artery and vein deep to the pectoralis minor muscle. The artery will be seen as a round pulsating echo-lucent (dark) circle at a depth of about 3-4 cm. This can be further confirmed by colour Doppler. The vein is almost always caudad to the artery. The nerves of the brachial plexus are arranged radially around the axillary artery in the infraclavicular space and appear hyperechoic. Needle insertion The in plane cephalad to caudad approach is recommended to visualise the needle shaft and tip during needle advancement. Insert a 50 mm insulated needle below the clavicle at an angle of 45 degrees and advance the needle slowly from the cephalad end of the transducer along its long axis in the caudad direction. Aim the needle tip to the 6 o clock position (posterior cord) next to the artery. Aspirate then inject 10-15 mls of local anaesthetic around the axillary artery. The goal is to deposit local anaesthetic around all three cords of the brachial plexus, resulting in U shaped spread of local anaesthetic around the artery. Aspirate then inject further 10 mls as the needle is withdrawn to the 9 o clock position (lateral cord). If spread to the 3 o clock position (medial cord) is inadequate, it may be necessary to separately place the block needle between the axillary artery and vein to access the medial cord. Visualization of the block needle can be challenging due to a steep angle of insertion (> 45 degrees). One way to accurately locate the needle tip is to tilt the needle tip superficially (i.e., angle anteriorly in this case). If the needle tip is posterior to the axillary artery (6 o'clock position), one will see lifting of the artery anteriorly. If the needle tip is at the 9 o'clock position, tilting the needle will push the artery caudad. Side effects Rarely recurrent laryngeal nerve block, stellate ganglion block Complications • • • Vascular puncture Inadvertant intravascular injection Risk of Pneumothorax-less than 1:1000 in experienced hands References • • • • Marhofer P: Ultrasound Guidance for Nerve Blocks; Principles and Practical Implementation. Oxford University Press 2008. www.neuraxiom.com Sandhu,N.S, Capan,L.M: Ultrasound guided infraclavicular brachial plexus block.BJA, Vol 89, issue 2, pg 254-259 Russon,K, Pickworth T, Harrop-Griffiths, W:Upper limb blocks. Anaesthesia, Vol 65, Supp 1, April 2010