Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
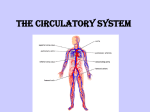
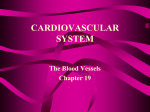
The Cardiovascular System: Blood Vessels and Hemodynamics Blood vessels provide structures for the flow of blood, exchange of nutrients and wastes in tissues. They also play a role in adjusting the velocity and volume of blood flow. The cardiovascular system contributes to homeostasis of the body by transporting and distributing blood throughout the body in order to deliver materials and carry away wastes. Blood vessels, which form a closed system of tubes carries blood away from the heart to the tissues and then returns the blood to the heart. In this topic, we focus on the structure and function of the various types of blood vessels and on hemodynamics, the forces involved in circulating blood throughout the blood vessels of the body. Structure and Function of Blood Vessels The five main types of blood vessels are arteries, arterioles, capillaries, venules and veins. Arteries carry blood away from the heart to other organs. Large, elastic arteries leave the heart divide into medium-sized, muscular arteries that branch out into the various regions of the body. Medium-sized arteries divide into small arteries, turn divide into smaller arteries, the arterioles. Arterioles branch into capillaries. The thin walls of capillaries allow the exchange of substances between the blood and body tissues. Capillaries within a tissue reunite to form small veins, the venules; they merge to form progressively larger blood vessels, the veins. Veins carry blood from the tissues back to the heart. Larger blood vessels are served by their own blood vessels, the vasa vasorum, and nerves, the nervi vasorum, located within the walls of the vessels. Arteries The wall of an artery has three coats or tunics: 1. Tunica Interna (Intima) Tunica interna the inner most coat, contains a lining of simple squamous epithelium, the endothelium, a basement membrane, and a layer of elastic tissue, the internal elastic membrane (lamina). The endothelium is a continuous layer of cells that line the inner surface of the entire CV system. The endothelium is the only tissue that contacts the blood. The tunica interna is closest to the lumen, the space through which blood flows. 2. Tunica Media The tunica media is the middle coat and is usually the thickest layer. It consists of elastic membranes, formed by fusion of the elastic fibers and smooth muscle fibers that extend circularly around the lumen. The tunica media also has an external elastic membrane (lamina) composed of elastic tissue. Due to their elastic membranes, arteries normally have high compliance, which means that their walls stretch easily or expand without tearing in response to an increase in pressure. 3. Tunica Externa The tunica externa is the outer most coat and is composed mainly of elastic and collagenous fibers. Sympathetic neurons of the autonomic nervous system are distributed to the smooth muscle of the tunica media (nervi vasorum). Increase in sympathetic stimulation stimulates the smooth muscle to contract, narrowing the lumen. Decrease in the diameter of the lumen of a blood vessel is called 1 vasoconstriction. Smooth muscle fibers relax when sympathetic stimulation decreases or when certain chemicals, such as nitric oxide (NO), H+ ions and lactic acid, are present. Increase in lumen diameter is called vasodilation. Elastic Arteries (Conducting Arteries) The largest diameter arteries are elastic arteries because the tunica media contains a high proportion of elastic connective tissue membranes. Elastic arteries have walls that are relatively thin in proportion to their overall diameter. Their internal elastic lamina is incomplete and their external elastic lamina is thin. Within the wall of the elastic arteries the elastic fibers fuse to form sheets, which appear in cross section of the elastic arteries as parallel broken bands of elastic membranes, the fenestrated membranes. Elastic arteries function to help propel blood onward while the ventricles are relaxing. As blood is ejected from the heart into elastic arteries, their walls stretch to accommodate the surge of blood, storing mechanical energy for a short time; the elastic membranes function as a pressure reservoir. Then, the elastic membranes recoil and convert the stored (potential) energy into kinetic energy, causing the blood to be pushed onward. Blood continues to move through the arteries even while the ventricles are relaxed. The elastic arteries conduct blood from the heart to medium-sized muscular arteries. The elastic arteries are the conducting arteries of the CV system. Muscular Arteries (Distributing Arteries) Medium-sized arteries are the muscular arteries because their tunica media contains more smooth muscle and fewer elastic membranes than elastic arteries. Muscular arteries are capable of greater vasoconstriction and vasodilation to adjust the rate of blood flow. Large amount of smooth muscle makes the walls of muscular arteries relatively thick. Muscular arteries have a thin complete internal elastic lamina and a prominent external elastic lamina. Muscular arteries are the distributing arteries because they distribute blood to various parts of the body. Arterioles (Resistance Arteries) An arteriole is a small artery that delivers blood to the capillaries. Tunica media is composed of smooth muscle and very few elastic membranes. Arterioles play a role regulating blood flow from arteries into capillaries by regulating resistance to blood flow. Resistance is caused mainly by friction between blood and the inner walls of blood vessels. When the blood vessel diameter is smaller, the friction is greater. Because contraction and relaxation of the smooth muscle in arteriole walls can change their diameter, arterioles are known as resistance vessels. Contraction of arteriolar smooth muscle causes vasoconstriction, which increases vascular resistance and decreases blood flow into capillaries. Relaxation of arteriolar smooth muscle causes vasodilation, decreases vascular resistance and increases blood flow into capillaries. A change in arteriole diameter can also affect blood pressure: vasoconstriction of arterioles increases blood pressure and vasodilation of arterioles decreases blood pressure. Capillaries (Exchange Vessels) Capillaries are microscopic vessels that connect arterioles to venules. The flow of blood through capillaries is called the microcirculation. Capillaries are placed near almost every cell in the body. 2 Capillaries are the exchange vessels because their prime function is the exchange of nutrients and wastes between the blood and tissue cells through the interstitial fluid. Capillary walls are composed of a single layer of endothelial cells and a basement membrane. Exchange of materials occurs only through the walls of capillaries, the walls of arteries, arterioles, venules and veins are too thick. Capillaries form extensive branching networks that increase the surface area available for exchange of materials. Regulation of blood Flow Through the Capillary Bed A metarteriole is a vessel that emerges from an arteriole and supplies a network of capillaries, the capillary bed. The proximal end of a metarteriole is surrounded by scattered smooth muscle fibers; the contraction and relaxation of the smooth muscle fibers help regulate blood flow through the capillary bed. At the junctions between the metarteriole and the capillaries of the capillary bed are rings of smooth muscle fibers called precapillary sphincters that control the flow of blood through the capillary bed. When the precapillary sphincters are relaxed (open), blood flows into the capillary bed. When precapillary sphincters contract (close) blood flow through the capillary bed ceases or decreases. The blood then bypasses the capillary bed and empties into the venule. Blood flows intermittently through a capillary bed due to contraction and relaxation of the smooth muscle of metarterioles and the precapillary sphincters. The intermittent contraction and relaxation is called vasomotion. Vasomotion is due to chemicals, such as nitric oxide, released by the endothelial cells. At any given time, blood flows through only about 25% of a capillary bed. The body contains three different types of capillaries; continuous capillaries, fenestrated capillaries, and sinusoids. Read on own. Venules (Collecting Vessels) When capillaries unite, they form small veins, the venules. The venules collect blood from capillaries and deliver it to the veins. Veins (Returning Vessels) The veins are composed of essentially the same three coats as the arteries. Tunica interna is thinner than that of the arteries. Tunica media is much thinner than in arteries with relatively little smooth muscle and elastic membranes. Tunica externa is the thickest layer and consists of collagenous and elastic connective tissue fibers. Veins lack internal and external elastic laminae as found in arteries. The veins are distensible enough to adapt to variations in the volume and pressure but are not designed to withstand high pressure. The lumen of a vein is larger than that of a comparable artery. Veins often appear collapsed (flattened) in histological section. Many veins, especially those in the limbs, have valves, thin folds of tunica interna that form flap-like cusps. Valve cusps project into the lumen, pointing toward the heart. The low blood pressure in veins allows blood returning to the heart to slow and back up. The valves aid in venous return by preventing the backflow of blood. 3 Anastomoses Most tissues receive blood from more than one artery. The union of the branches of arteries supplying the same body region is called an anastomosis. Anastomoses between arteries provide alternate routes for blood to reach a tissue or organ. If blood flow stops, the circulation to a part of the body is not necessarily stopped. Anastomose allows for an alternate route of blood flow. The anastomosis is a collateral circulation. Blood Distribution and Reservoirs The largest portion of the blood volume at rest is in systemic veins and venules. Because systemic veins and venules contain a large percentage of the blood volume, they function as blood reservoirs from which blood can be diverted quickly if the need arises. The principal blood reservoirs are the veins of the abdominal organs, liver, spleen and the veins of the skin. Capillary Exchange Mission of the entire cardiovascular system is to keep blood flowing through capillaries to allow capillary exchange of substances between blood and tissue cells through the interstitial fluid. Substances leave the capillaries and enter the capillaries by 3 mechanisms. Diffusion - Read on own. Transcytosis - Read on own. Bulk Flow: Filtration and Reabsorption Bulk flow is a passive process in which large numbers of ions, molecules, or particles in a fluid move together in the same direction. The substances move at rates far greater than can be accounted for by diffusion alone. Bulk flow occurs from an area of higher pressure to an area of lower pressure. Diffusion is more important for solute exchange between blood and interstitial fluid. Bulk flow is more important for regulation of relative volumes of fluid between the blood and interstitial fluid. Pressuredriven movement of fluid and solutes from blood capillaries into interstitial fluid is called filtration. Pressure-driven movement from interstitial fluid into blood capillaries is called reabsorption. The two pressures that promote filtration are blood hydrostatic pressure (BHP), the main pressure generated by the pumping action of the heart, and interstitial fluid osmotic pressure (IFOP). The two pressures that promote reabsorption are blood colloid osmotic pressure (BCOP), the main pressure, and interstitial fluid hydrostatic pressure (IFHP). The balance of these pressures, net filtration pressure (NFP), determines whether the volumes of blood and interstitial fluid remain steady or change. Volume of fluid and solutes reabsorbed is almost as large as the volume filtered. This near equilibrium is known as Starling’s law of the capillaries. The blood hydrostatic pressure (BHP) is about 35mm Hg at the arterial end of a capillary and about 16 mm Hg at the capillary’s venous end. BHP “pushes” fluid out of capillaries into interstitial fluid. Opposing pressure of the interstitial fluid, the interstitial fluid hydrostatic pressure (IFHP) “pushes” 4 fluid from interstitial spaces back into capillaries. IFHP is close to zero. Blood colloid osmotic pressure (BCOP) is a force caused by the colloidal suspension of these large proteins in plasma that averages 26 mm Hg in most capillaries. The effect of BCOP is to “pull” fluid from interstitial spaces into capillaries. Opposing BCOP is interstitial fluid osmotic pressure (IFOP), “pulls” fluid out of capillaries into interstitial fluid. Normally, IFOP is very small, 1mm Hg. Whether fluids leave or enter the capillaries depends on the balance of pressures. If the pressures that push fluid out of capillaries exceed the pressures that pull fluid into capillaries, fluid move from capillaries into interstitial spaces (filtration). If the pressures that pull fluid out of interstitial spaces into capillaries exceed the pressures that push fluid out of capillaries, then fluid will move from interstitial spaces into capillaries (reabsorption). The net filtration pressure (NFP) indicates the direction of fluid movement. Push Pull Pull Push NFP = (BHP + IFOP) – (BCOP + IFHP) Pressures that Promote filtration Overall “Pushes Out” At the arterial end of a capillary, Pressures that promote reabsorption Overall “Pulls In” NFP = (35 + 1) mm Hg – (26 + 0) mm Hg = 36 - 26 = 10mm Hg There is a net outward pressure of 10mm Hg and fluid moves out of the capillary into interstitial spaces (filtration). At the venous end of a capillary, NFP = (16 + 1) mm Hg – (26 + 0) mm Hg = 17 26 = -9mm Hg At the venous end of a capillary, the negative value (-9mmHg) represents a net inward pressure and fluid moves into the capillary from tissue spaces (reabsorption). On average, about 85% of the fluid filtered out of capillaries is reabsorbed. The excess filtered fluid and the few proteins that do escape from blood into interstitial fluid enter lymphatic capillaries and return to the blood. About 20 liters of fluid filter out of capillaries/day, 17 liters are reabsorbed, and 3 liters enter lymphatic capillaries. Hemodynamics: Factors Affecting Blood Flow Hemodynamics is a study of the interrelationship among blood pressure, blood flow in terms of volume and velocity and resistance to blood flow. Blood flow is the volume of blood that flows through any tissue in a given time period (in mL/min). Total blood flow is cardiac output (CO), the volume of blood that circulates through systemic and/or pulmonary blood vessels each minute. 5 Cardiac output (CO) = heart rate (HR) x stroke volume (SV). How the cardiac output becomes distributed into circulatory routes depends on two factors: 1. The pressure difference that drives the blood flow and 2. The resistance to blood flow in specific blood vessels. The blood flows from regions of higher pressure to regions of lower pressure; the greater the pressure difference, the greater the blood flow. The higher the resistance, the smaller the blood flow and slower the velocity. Blood Pressure The greater the pressure difference, the greater the blood flow. Contraction of the ventricles generates blood pressure (BP), which is the hydrostatic pressure exerted by blood on the walls of a blood vessel. BP is highest in the aorta and large systemic arteries; 110mm Hg during systole (ventricular contraction), 70mm Hg during diastole (ventricular relaxation). Systolic blood pressure is the highest pressure attained in arteries during systole, due to the pressure of the blood against the walls of the arteries. Diastolic blood pressure is the lowest arterial pressure during diastole due to the elastic recoil of the arteries on the blood. As blood leaves the aorta and flows through the systemic circulation, its pressure falls progressively as the distance from the left ventricle increases. Blood pressure decreases to about 35mm Hg in the capillaries, where the pressure fluctuations disappear. At the venous end of the capillaries, blood pressure has dropped to about 16mm Hg. Blood pressure continues to drop as blood enters the venules and then the veins because these vessels are farthest from the left ventricle. Blood pressure reaches 0mm Hg as blood flows into the right ventricle. Mean arterial pressure (MAP), the average blood pressure in arteries, is one-third of the way between the diastolic and systolic pressures. Pulse Pressure (PP) = systolic BP – diastolic BP MAP = diastolic BP + 1/3 (systolic BP – diastolic BP or Pulse Pressure) If a person’s BP is 110/70mm Hg, the MAP is MAP = = MAP is also equal to CO x R 70 + 1/3 (110 – 70) 70 + 13 = 83 mm Hg. MAP = CO x R. If cardiac output rises due to increase in stroke volume or heart rate, then the mean arterial pressure rises as long as resistance remains steady. A decrease in cardiac output causes a decrease in mean arterial pressure if resistance does not change. Another way to calculate cardiac output is to rearrange the terms of this equation by dividing the mean arterial pressure (MAP) by resistance (R). CO = MAP/R 6 Blood pressure also depends on the total volume of blood in the cardiovascular system. The normal volume of blood in an adult is about 5 liters. Any decrease in this volume, decreases the blood flow (the amount of blood that is circulated through the arteries each minute). A modest decrease in volume can be compensated for by homeostatic mechanisms that maintain blood pressure, but if the decrease in blood volume is greater than 10% of the total, blood pressure drops. Increases blood volume, such as due to water retention, increases blood pressure. Resistance Vascular resistance is the opposition to blood flow due to friction between blood and the walls of blood vessels. Vascular resistance depends on diameter of the blood vessel lumen, blood viscosity and total blood vessel length. 1. Diameter of the lumen – The smaller the lumen of a blood vessel the greater its resistance to volume of blood flow and slower the velocity of the blood flow. Resistance is inversely proportional to the fourth power of the diameter (d) of the blood vessel’s lumen. R 1/d4 Flow is directly proportional to the fourth power of the diameter of the blood vessel’s lumen. F d4 The smaller the diameter of the blood vessel, the greater the resistance to the blood flow and the smaller the blood flow volume and velocity. The larger the diameter of the blood vessel, the smaller the resistance to blood flow and the greater the blood flow volume and velocity. If the diameter of a vessel increases from 1mm to 2mm, the diameter of the vessel has increased two times, the flow increases 16 times. If the diameter of a blood vessel decreases by one-half, its resistance to blood flow increases 16 times. In small vessels nearly all of the blood is very near the wall of the vessel, so there is high resistance to blood flow and volume and velocity of the blood flow is slow. When the vessel has a larger diameter more of the blood is flowing in the center of the vessel’s lumen, where there is less resistance and the blood flow volume and velocity is faster. The diameter of the blood vessel’s lumen plays a very important role in determining the volume and velocity (rate) of blood flow through the blood vessel. Vasoconstriction narrows the lumen and vasodilation widens the lumen. Fluctuations in blood flow through a given tissue are due to vasoconstriction and vasodilation of the tissue’s arterioles. As arterioles dilate, resistance decreases and blood pressure falls. As arterioles constrict, resistance increases, and blood pressure rises. 2. Blood viscosity – The viscosity (thickness) of blood depends mostly on the ratio of red blood cells to plasma volume, and to concentration of proteins in plasma. The higher the blood’s viscosity, the higher the resistance. Condition that increases the viscosity of blood, such as dehydration or an unusually high number of red blood cells thus increases blood pressure. A depletion of plasma proteins or red blood cells decreases viscosity and thus decreases blood pressure. 3. Total blood vessels length – Resistance to blood flow through a vessel is directly proportional to the length of the blood vessel, the longer a blood vessel the greater the resistance. Blood flow is directly proportional to the 4th power of the d and inversely proportional to the viscosity and vessel length. 7 Systemic vascular resistance (SVR) or Total Peripheral Resistance (TPR) Total peripheral resistance (TPR), refers to all the vascular resistance by systemic blood vessels. Diameters of arteries and veins are large; their resistance is very small because most of the blood does not come into physical contact with the walls of the blood vessel. The smallest vessels – arterioles, capillaries, and venules –contribute the most resistance. A major function of arterioles is to control SVR and therefore blood pressure and blood flow to particular tissues by changing their diameters. Arterioles need to change their diameters only slightly to have a large effect on TPR. Venous Return Venous return is the volume of blood flowing back to the heart through systemic veins due to the pressure generated by contractions of the left ventricle. The pressure difference from venules (averaging about 16mm Hg) to the right ventricle (0mm Hg), although small is sufficient to cause venous return to the heart. If blood remains in the right atrium or right ventricle, venous return will decrease. Besides blood pressure generated by the heart to push the blood, two other mechanisms “pump” blood from the lower body back to the heart: 1. the skeletal muscle pump and 2. the respiratory pump. Both pumps depend on the presence of valves in the veins. 1. The skeletal muscle pump – Contraction of leg muscles compresses the vein. The compression pushes blood through the open proximal valve, an action called milking. Milking action refers to skeletal muscle contractions that drive venous blood toward the heart. Distal valve in the uncompressed segment of the vein closes as some the back flowing blood is pushed against it. 2. The respiratory pump – During inhalation the diaphragm moves downward, which causes a decrease in pressure in the thoracic cavity and an increase in pressure in the abdominal cavity. Abdominal veins are compressed and blood moves from the compressed abdominal veins into the decompressed thoracic veins and then into the right atrium. During exhalation the pressures reverse and valves in the veins prevent backflow of blood from the thoracic veins to the abdominal veins. Velocity of Blood Flow The speed or velocity of blood flow is inversely related to the cross-sectional area. Velocity is slowest where the total cross-sectional area is greatest. Each time an artery branches, the total cross-sectional area of all its branches is greater than the cross-sectional area of the original vessel. Blood flow’s velocity becomes slower and slower as blood moves further away from the heart and is slowest in the capillaries. When venules unite to form veins, the total cross-sectional area becomes smaller and blood flow’s velocity becomes faster. Thus, the velocity of blood flow decreases as blood flows from the aorta to arteries to arterioles to capillaries, and increases as it leaves capillaries and returns to the heart. The slow rate of flow through capillaries aids the exchange of materials between blood and interstitial fluid. Circulation time is the time required for a drop of blood to pass from the right atrium, through the systemic and pulmonary circulations back again to the right atrium. In a resting person, circulation time normally is about 1 minute. 8 Summary of Factors that Increases Mean Arterial Blood Pressure (MAP) Factors that increase CO and SVR will increase MAP. Control of Blood Pressure and Blood Flow Several negative feedback systems control blood pressure by adjusting heart rate, stroke volume, systemic vascular resistance, and blood volume. These negative feedback systems also adjust the distribution of blood flow by controlling the SVR. Some negative feedback systems allow rapid adjustments to sudden changes in blood pressure. Other negative feedback systems act more slowly to provide long-term regulation of blood pressure. Role of the Cardiovascular Center Cardiovascular (CV) center in the medulla oblongata helps regulate heart rate, stroke volume and vascular resistance to control blood pressure through negative feedback mechanisms. Neurons within the CV center receive information concerning heart rate, contractility (force of contraction) of the ventricles, and blood vessel diameter. Within the CV center there are the cardiostimulatory center and cardioinhibitory center. Also within the CV center there is the vasomotor center that controls blood vessel diameter by causing constriction (vasoconstrictor center) or dilation (vasodilator center). Sensory Input The CV center receives input from higher brain regions and from sensory receptors. Nerve impulses descend from the cerebral cortex, limbic system, and hypothalamus to affect the cardiovascular center. 9 Three main types of sensory receptors that provide input to the cardiovascular center are proprioceptors, baroreceptors, and chemoreceptors. Proprioceptors monitor movements of joints and muscles and provide input to the cardiovascular center during physical activity. Their activity accounts for the rapid increase in heart rate at the beginning of exercise. Baroreceptors monitor changes in pressure and stretch in the walls of blood vessels and chemoreceptors monitor the concentration of various chemicals in the blood. Motor Output Output from the CV center moves along sympathetic and parasympathetic neurons of the ANS to the heart. Sympathetic impulses reach the heart via cardiac accelerator nerves. Increase in sympathetic stimulation increases heart rate and contractility; a decrease in sympathetic stimulation decreases heart rate and contractility. Parasympathetic stimulation, conveyed along the vagus (X) nerves, decreases heart rate. Opposing sympathetic (stimulatory) and parasympathetic (inhibitory) influences control the heart. The CV center continually sends impulses to smooth muscle in the blood vessel walls via vasomotor nerves. These sympathetic preganglionic neurons exit the spinal cord through all thoracic and the first one or two lumbar spinal nerves to the sympathetic ganglia. From there, impulses propagate along sympathetic postganglionic neurons that innervate blood vessels in viscera and peripheral areas. The vasomotor center of the CV center continually sends impulses to arterioles throughout the body. The result is a moderate state of tonic contraction or vasoconstriction, called vasomotor tone that sets the resting level of systemic vascular resistance. Sympathetic stimulation of most veins causes constriction that moves blood out of venous blood reservoirs and increases blood pressure. Neural Regulation of Blood Pressure The nervous system regulates blood pressure via negative feedback loops by two types of reflexes; baroreceptor reflexes and chemoreceptor reflexes. Baroreceptor Reflexes Baroreceptors, pressure-sensitive sensory receptors located in the aorta, internal carotid arteries. They send impulses to the cardiovascular center to help regulate blood pressure. The two baroreceptor reflexes are the carotid sinus reflex and the aortic reflex. Carotid Sinus Reflex Baroreceptors in the wall of the carotid sinuses initiate the carotid sinus reflex, which helps regulate blood pressure in the brain. Blood pressure stretches the wall of the carotid sinus, which stimulates the baroreceptors. Nerve impulses propagate from the carotid sinus baroreceptors over sensory axons in the glossopharyngeal (IX) nerves to the CV center in the medulla oblongata. 10 Aortic Reflex Bar receptors in the wall of the ascending aorta and arch of the aorta initiate the aortic reflex, which regulates systemic blood pressure. Nerve impulses from aortic baroreceptors reach the CV center via sensory axons of the vagus (X) nerves. When blood pressure falls, the baroreceptors are stretched less, and they send nerve impulses at a slower rate to the CV center. In response, the CV center decreases parasympathetic stimulation of the heart by way of motor axons of the vagus nerves and increases sympathetic stimulation of the heart via cardiac accelerator nerves. Also increased sympathetic stimulation increases secretion of epinephrine and norepinephrine by the adrenal medulla. As the heart beats faster and more forcefully cardiac output increases, due to vasoconstriction systemic vascular resistance rise and blood pressure increases to the normal level. When an increase in pressure is detected, the baroreceptors send impulses at a faster rate. CV center responds by increasing parasympathetic stimulation and decreasing sympathetic stimulation. This decreases heart rate and force of contraction and reduces the cardiac output. The CV center also slows the rate at which it sends sympathetic impulses along vasomotor neurons. This causes vasodilation lowering systemic vascular resistance. Decreased cardiac output and decreased systemic vascular resistance lower systemic arterial blood pressure to normal level. Chemoreceptor Reflexes Chemoreceptors, sensory receptors that monitor the chemical composition of blood, are located in the carotid sinus and arch of the aorta in small structures called carotid bodies and aortic bodies. These chemoreceptors detect changes in blood level of O2, CO2, and H+ ions. Hypoxia (lowered O2 availability), acidosis (an increase in H+ ion concentration), or hypercapnia (excess CO2) stimulates the chemoreceptors to send impulses to the CV center. In response, the CV center increases sympathetic stimulation to arterioles and veins producing vasoconstriction and an increase in blood pressure. These chemoreceptors also provide input to the respiratory center in the brain stem to adjust the rate of breathing. Hormonal Regulation of Blood Pressure Several hormones help regulate blood pressure and blood flow by altering cardiac output, changing systemic vascular resistance, adjusting the total blood volume. 1. Renin – angiotensin – aldosterone (RAA) system. When blood volume or blood flow’s velocity to the kidneys decrease, juxtaglomerular cells in the kidneys secrete renin into the blood. Renin and angiotensin converting enzyme (ACE) act on their substrates to produce the active hormone angiotensin II, which raises blood pressure in two ways. 1. Angiotensin II is a potent vasoconstrictor; it raises blood pressure by increasing systemic vascular resistance. 2. Angiotensin II stimulates secretion of aldosterone, which increases reabsorption of Na+ ions and water by the kidneys. The water reabsorption increases total blood volume, which increases blood pressure. 2. Epinephrine and norepinephrine. In response to sympathetic stimulation, the adrenal medulla releases epinephrine and norepinephrine. These hormones increase cardiac output by increasing the 11 rate and force of heart contractions. They also cause vasoconstriction of arterioles and veins in the skin and abdominal organs and vasodilation of arterioles in cardiac and skeletal muscle which helps increase blood flow to muscle during exercise. 3. Antidiuretic hormone (ADH). ADH is produced by the hypothalamus and released from the posterior pituitary in response to dehydration or decreased blood volume. ADH causes vasoconstriction, which increases blood pressure. For this reason ADH is also called vasopressin. 4. Atrial natriuretic peptide (ANP). Released by cells in the atria of the heart, ANP lowers blood pressure by causing vasodilation and by promoting the loss of salt and water in the urine, which reduces blood volume and blood pressure. Autoregulation of Blood Pressure In each capillary bed, local changes can regulate vasomotion. When vasodilators produce local dilation of arterioles and relaxation of precapillary sphincters, blood flow into capillary networks is increased which increases O2 level. Vasoconstrictors have the opposite effect. The ability of a tissue to automatically adjust its blood flow to match its metabolic demands is called autoregulation. Two general types of stimuli cause autoregulatory changes in blood flow: 1. Physical changes. a. Warming promotes vasodilation, and cooling cause’s vasoconstriction. b. Myogenic response - Smooth muscle in arteriole walls exhibits a myogenic response i.e. contracts more forcefully when it is stretched and relaxes when stretching lessens. 2. Vasodilating and vasoconstricting chemicals. Several types of cells, WBCs, platelets, smooth muscle fibers, macrophages, and endothelial cells, release a wide variety of chemicals that alter blood vessel diameter. Vasodilating chemicals released by metabolically active tissue cells include K+ ions, H+ ions, lactic acid (lactate), and adenosine (from ATP). Another vasodilator released by endothelial cells is nitric oxide (NO). Tissue trauma or inflammation causes release of vasodilating kinins and histamine. Vasoconstrictors include thromboxane A2, superoxide radicals, serotonin (from platelets), and endothelins (from endothelial cells). A difference between the pulmonary and systemic circulations is their autoregulatory response to changes in O2 level. The walls of blood vessels in the systemic circulation dilate in response to low O2. During vasodilation, O2 delivery increases, to restore the normal O2 level. The walls of blood vessels in the pulmonary circulation constrict in response to low levels of O2. This response ensures that blood bypasses those alveoli (air sacs) in the lungs that are poorly ventilated by fresh air. Most blood flows to better ventilated areas of the lung. Shock and Homeostasis Shock is a failure of the cardiovascular system to deliver enough O2 and nutrients to meet cellular metabolic needs. There are four main types of shock are but all are characterized by inadequate blood flow to body tissues. Shock can be due to decreased blood volume (hypovolemic shock), poor heart function (cardiogenic shock), inappropriate vasodilation (vascular shock), and obstruction of blood flow (obstructive shock). 12 Homeostatic Responses to Shock The major mechanisms of compensation in shock are negative feedback systems that work to return cardiac output and arterial blood pressure to normal. 1. Activation of the renin – angiotensin – aldosterone system. Decreased blood flow to the kidneys causes the kidneys to secrete renin and initiates the reninangiotensin-aldosterone system. Angiotensin II causes vasoconstriction and stimulates the adrenal cortex to secrete aldosterone, a hormone that increases reabsorption of Na+ ions and water by the kidneys. The vasoconstriction and reabsorption of Na+ ions and water increases systemic vascular resistance and blood volume to help raise blood pressure. 2. Secretion of antidiuretic hormone. In response to decreased blood pressure, the posterior pituitary releases more ADH. ADH enhances water reabsorption by the kidneys, which conserves remaining blood volume. It also causes vasoconstriction, which increases systemic vascular resistance. 3. Activation of the sympathetic division of the ANS. As blood pressure decreases; the aortic and carotid baroreceptors initiate sympathetic responses throughout the body. There is marked vasoconstriction of arterioles and veins of the skin, kidneys, and other abdominal viscera but not the brain or heart. Constriction of the arterioles increases systemic vascular resistance and the constriction of the veins increases venous return to maintain an adequate blood pressure. Sympathetic stimulation also increases heart rate and contractility and increases secretion of epinephrine and norepinephrine by the adrenal medulla. These hormones intensify vasoconstriction and increased heart rate and contractility to raise blood pressure. 4. Release of local vasodilators. In response to hypoxia, cells liberate vasodilators – including K+ ions, H+ ions, lactic acid, adenosine and NO – that dilates arterioles and relaxes precapillary sphincters. Vasodilation increases local blood flow and restore O2 level to normal in local body part. Hypertension Hypertension is persistently high blood pressure. Hypertension is linked to an increased risk of cardiovascular disease. Normal blood pressure is systolic pressure < 120mm Hg and diastolic pressure < 80mm Hg. Major Consequences or Effects of Untreated Hypertension High blood pressure causes considerable damage to the blood vessels, heart, brain and kidneys. In blood vessels hypertension causes thickening of the tunica media, accelerates development of atherosclerosis and coronary artery disease and increases systemic vascular resistance. In the heart, hypertension increases the afterload, which forces the ventricles to work harder to eject blood from the heart. An increased afterload leads to myocardial hypertrophy that is accompanied by muscle damage and a buildup of collagenous fibers between the muscle fibers (fibrosis). The myocardial hypertrophy causes the left ventricle to enlarge, weaken and dilate. In the brain prolonged hypertension causes the arteries in the brain to rupture resulting in a stroke. 13 In the kidneys hypertension damages the arterioles, causing the walls of these arterioles to thicken and narrows their lumens. The blood supply to the kidneys is reduced; the kidneys secrete more renin, which elevates the blood pressure even more. Hypertension Treatment Strategies Lifestyle Changes to Reduce Hypertension Lifestyle changes that can effectively manage hypertension are: Lose weight, limit alcohol intake, exercise, reduce intake of Na (salt), maintain recommended dietary intake of K, Ca, and Mg, don’t smoke and manage stress. Drug Treatment of Hypertension Drugs have different mechanisms of action to effectively lower blood pressure. Diuretics decrease blood pressure by decreasing blood volume because they increase elimination of water and salt in the urine. ACE (angiotensin converting enzyme) inhibitors block formation of angiotensin II, thus promote vasodilation and decrease the secretion of aldosterone. Beta blockers reduce blood pressure by inhibiting the secretion of renin and decreases heart rate and contractility. Vasodilators relax the smooth muscle in the arterial walls, causing vasodilation. This lowers blood pressure by lowering systemic vascular resistance. Ca channel blockers are vasodilator drugs, which slows the inflow of Ca+2 ions into vascular smooth muscle fibers. These drugs reduce the heart’s workload by slowing Ca+2 ions entry into pacemaker and regular myocardial fibers, decreasing heart rate and force of myocardial contraction. Atherosclerosis and Coronary Artery Disease (CAD) CAD results from the effects of accumulation of atherosclerotic plaques in coronary arteries (and other arteries) leading to a reduction in blood flow to the myocardium. Development of Atherosclerotic Plaques Thickening of the walls of arteries and loss of elasticity are the main characteristics of arteriosclerosis, hardening of the arteries. One form of arteriosclerosis is atherosclerosis, a progressive disease characterized by the formation in the walls of large and medium-sized arteries of lesions called atherosclerotic plaques. Atherosclerotic plaques are deposits of fatty material in the wall of the blood vessel. Cholesterol is insoluble in water; it must become water soluble in order to be transported in the blood. To accomplish this, the cholesterol combines with lipoproteins in the plasma. Two major lipoproteins are low-density lipoproteins (LDLs) and high-density lipoproteins (HDLs). LDLs transport cholesterol from the liver to body cells where the cholesterol is used. However, excessive amounts of LDLs promote atherosclerosis. The cholesterol carried in the LDLs is known as “bad cholesterol”. HDLs remove excess cholesterol from body cells and transport it to the liver for elimination. Because HDLs decrease blood cholesterol level, the cholesterol in the HDLs is known as “good cholesterol”. On analysis of HDL to LDL concentration, HDLs should to high and LDLs should be low. 14 The formation of atherosclerotic plaques begins when excess LDLs from the blood accumulate in the inner layer of an artery wall and the lipids and proteins in the LDLs undergo oxidation. In response to the oxidation the endothelial cells and smooth muscle fibers of the artery secrete substances that attract monocytes from the blood and convert them into macrophages. The macrophages then ingest and become filled with the oxidized LDL particles and have a foamy appearance (foam cells) under the microscope. T lymphocytes follow the monocytes into the inner lining of the artery where they release chemicals that intensify the inflammatory response. Together, the foam cells, macrophages and T cells form a fatty streak, the beginning of an atherosclerotic plaque. Macrophages secrete chemicals that cause smooth muscle fibers in the tunica media of the artery to migrate to the top of the atherosclerotic plaque, to form a cap over it and walling the plaque off from the blood. Most atherosclerotic plaques expand away from the lumen of the blood vessel rather than into it so blood flow can occur through an artery with relative ease. A few heart attacks do occur when plaque in a coronary artery expands into the lumen of the blood vessel and restricts blood flow. Most heart attacks occur when the cap over the plaque breaks open in response to chemical s produced by the foam cells. Also T cells induce the foam cells to produce tissue factor (thromboplastin) that begins the cascade of reactions that cause blood clot formation. If the clot in a coronary artery is large enough, it can decrease or stop blood flow and result in a heart attack. 15