Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
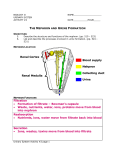
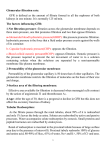
Renal Physiology & Fluid and Electrolyte Balance Keri Muma Bio 6 Functions of the Urinary System Kidneys – eliminate unwanted plasma constituents through the urine while conserving materials of value to the body Excrete nitrogenous waste – urea, uric acid, creatinine Regulate blood volumes – by regulating H2O balance and release of erythropoietin Regulates blood pressure – releases renin which triggers vasoconstriction and aldosterone secretion Regulates chemical composition of the blood – regulating ions and osmolarity Stabilizes pH – balances acids and bases Converting Vitamin D into its active form Anatomy of the Kidney Cortex – outer region Medulla – deep to the cortex Renal pelvis – flat funnel shaped cavity Microscopic Anatomy The functional unit of the kidney is the nephron Composed of vascular and tubular components Responsible for the filtration of blood and urine formation Tubular Component Bowman’s capsule – cup surrounding the glomerulus, collects filtrate Proximal convoluted tubule – extends from the Bowman’s capsule Loop of Henle – hairpin loop Tubular Component Distal convoluted tubule – leads away from the ascending loop of Henle to the collecting duct Collecting duct – receives filtrate from DCT of numerous nephrons Vascular Component Afferent arterioles – supply glomerulus Glomerulus – capillary knot Efferent arterioles – drains the glomerulus Peritubular capillaries – surround tubular portions of the nephron in the cortex Vasa recta – surround tubular portions of the nephron in the medulla Types of Nephron Cortical nephron – majority of the nephron is within the cortex with a short loop of Henle Juxtamedullary nephron – glomeruli is deep in the cortex and have a long loop of Henle that extends deep into the medulla Juxtaglomerular Apparatus (JGA) Region between the beginning of the DCT and the afferent arteriole Contains cells that regulate the rate of filtration and blood pressure Juxtaglomerular Apparatus (JGA) Macula densa – in the DCT, contain osmoreceptors that monitor solute concentration and flow rate of filtrate Granular cells – smooth muscle cells in the afferent arteriole, act as mechanoreceptors to monitor BP, synthesize and secrete renin Renal Processes The four basic processes of the nephrons are: glomerular filtration tubular reabsorption tubular secretion excretion Renal Processes Glomerular filtration is the first process. Plasma is filtered from the glomerulus into the Bowman’s capsule. Solutes and fluid are forced through the filtration membrane by hydrostatic pressure Blood cells and plasma proteins normally do not enter the filtrate Glomerular Filtration The glomerulus is more efficient at filtration than other capillary beds because: Its filtration membrane is significantly more permeable to solutes and water due to capillary pores Glomerular blood pressure is higher due to a larger afferent arteriole than efferent arteriole It has a higher net filtration pressure Glomerular Filtration Rate (GFR) Glomerular filtration rate - the total amount of filtrate formed per minute by the kidneys 125mL/min or 180L/day! Factors governing filtration rate at the capillary bed are: Net filtration pressure Total surface area available for filtration Filtration membrane permeability Forces Involved in Glomerular Filtration The glomerular capillary pressure (55 mm Hg) is the result of the blood pressure pushing on the inside of the capillary wall The plasma-colloid osmotic pressure (30 mm Hg) is due to the retention of plasma proteins in the blood of the glomerulus. The concentration of water is higher in the capsule, because proteins are absent there. Water tends to return to the glomerulus by osmosis There is also a hydrostatic pressure (15 mm Hg) tending to move fluid from the Bowman’s capsule into the glomerulus Forces Involved in Glomerular Filtration From the previous examples: The net pressure = glomerular blood pressure (plasma-colloid osmotic pressure + Bowman’s capsule hydrostatic pressure) 55 - (30 +15) = 10 The net filtration pressure is 10 mm Hg by this example. Regulation of Glomerular Filtration Uncontrolled shifts in the GFR can lead to fluid and electrolyte imbalances If the GFR is too high: Needed substances cannot be reabsorbed quickly enough and are lost in the urine If the GFR is too low: Everything is reabsorbed, including wastes that are normally disposed of Regulation of Glomerular Filtration Changes in GFR primarily result from changes in glomerular capillary blood pressure Three mechanisms control the GFR: 1. 2. 3. Renal autoregulation (intrinsic control) Sympathetic NS (extrinsic control) Hormonal mechanisms (the RAA system) Intrinsic Controls Autoregulation - regulates the GFR by factors within the kidneys. Under normal conditions, it prevents inappropriate changes in the GFR Intrinsic Controls Autoregulation entails two types of control: Myogenic – responds to changes in pressure in the renal blood vessels Tubuloglomerular feedback mechanism - senses changes in flow rate in the nephron’s tubular component Autoregulation of the GFR Myogenic mechanism – controlled by arteriole smooth muscle cells If the arterial pressure increases, the afferent arterioles constrict to lower GFR. If the arterial pressure decreases the afferent arterioles dilate to increase GFR. Autoregulation of GFR Tubuloglomerular feedback – involves the cells of the JGA Macula densa cells – detect change in flow-rate and osmolarity Increase in flow rate – releases vasoactive chemicals that cause vasoconstriction of afferent arteriole Decrease in flow rate – inhibits release of vasoactive chemicals causing vasodilation of afferent arteriole Tubuloglomerular Feedback Extrinsic Controls When the sympathetic nervous system is at rest or low levels then autoregulation mechanisms prevail and afferent arteriole is dilated However, the sympathetic nervous system can override the autoregulatory mechanisms to carry out long term adjustments for blood pressure if blood volume drops Extrinsic control of the GFR If arterial blood pressure severely drops, the baroreceptor reflex triggers vasoconstriction of systemic arterioles The afferent arterioles constrict by sympathetic innervation. Less blood flows through the glomeruli, lowering the blood pressure in these capillaries. The decrease in the GFR reduces urine volume. This helps to conserve plasma volume, increasing blood pressure. Extrinsic Controls The sympathetic nervous system also stimulates the renin-angiotensin-aldosterone mechanism Renin release is triggered by the following: Reduced stretch of the granular cells Stimulation of the granular cells by activated macula densa cells Direct stimulation of the granular cells via 1adrenergic receptors by renal nerves Renin-Angiotensin Mechanism Is triggered when the granular cells release renin Renin acts on angiotensinogen to produce angiotensin I Angiotensin I is converted to angiotensin II Angiotensin II: Causes systemic arteriole vasoconstriction Stimulates the adrenal cortex to release aldosterone As a result, both systemic blood pressure and blood volume increase Summary: Control of GFR Figure 25.10 Tubular Reabsorption Tubular Reabsorption - is the selective transfer of substances needed by the body from the filtrate back into the peritubular capillaries Reabsorption rates are high: 124 of 125 ml of filtered fluid per minute, 99% for water, 100% for glucose, and 99.5% for Na+ Tubular Reabsorption By transepithelial transport a reabsorbed substance must cross the tubule wall, enter the interstitial fluid, and pass through the wall of the peritubular capillaries, entering the blood. Epithelial cells of the nephron tubule have a luminal membrane and a basolateral membrane Sodium Reabsorption Sodium reabsorption is mostly driven by active transport Na+ enters the tubule cells at the luminal membrane by diffusion Then it is actively transported out of the tubules by a Na+-K+ pump at the basolateral membrane Sodium reabsorption 67% of sodium reabsorption occurs in the proximal tubule at a constant rate The reabsorption of sodium in the loop of Henle plays a role in the production of varying concentrations and volumes of the urine In the distal tubule, reabsorption of sodium is variable and depends on aldosterone More or less is reabsorbed, depending on the needs of the body. Sodium reabsorption Aldosterone increases Na+ absorption in the DCT and collecting ducts by promoting the insertion of: Additional Na+ channels in the luminal membrane Additional Na-K+ pumps into the basolateral membranes About 8% of the filtered Na+ is dependent on aldosterone for reabsorption If aldosterone is absent it is lost in the urine Action of Aldosterone Atrial Natriuretic Peptide Activity ANP inhibits Na+ reabsorption which: Decreases blood volume Lowers blood pressure ANP lowers blood volume and pressure by: Acting directly on collecting ducts to inhibit Na+ reabsorption Inhibits RAA pathway Dilates afferent arteriole triggering an increase in GFR which reducing water and sodium reabsorption ANP Reabsorption by PCT Cells The reabsorption of water, glucose, amino acids, and anions is linked to the active reabsorption of Na+ Active pumping of Na+ drives reabsorption of: Water by osmosis, aided by water-filled pores called aquaporins Anions follow by diffusion, down electrochemical gradient Glucose and amino acids by secondary active transport Tubular Reabsorption of Water The accumulation of sodium in the lateral spaces produces an osmotic gradient and hydrostatic pressure that drives the water into the peritubular capillaries. Tubular Reabsorption of Water 80% of water reabsorption is obligatory in the proximal tubule and loop of Henle Occurs by osmosis, no control 20% of water reabsorption is facultative in the distal tubule and collecting duct Based on the secretion of ADH, depends on body’s needs Role of ADH on Water Reabsorption ADH works on tubule cells through a cyclic AMP mechanism Promotes the insertion of aquaporins on the luminal membrane thus increasing water reabsorption Produces concentrated urine Tubular Reabsorption Glucose and amino acids are reabsorbed by secondary active transport and cotransported with sodium on the luminal membrane Nonreabsorbed Substances A transport maximum (Tm): Reflects the number of carriers in the renal tubules available Exists for nearly every substance that is actively reabsorbed When the carriers are saturated, excess of that substance is excreted Nonreabsorbed Substances Substances are not reabsorbed if they: Lack carriers Are not lipid soluble Are too large to pass through membrane pores Urea, creatinine, uric acid and other nitrogen containing wastes are usually excreted Renal Processes Tubular secretion is a selective process by which substances from the peritubular capillaries enter the lumen of the nephron tubule. Provides a mechanism to speed up the elimination of substances from the blood Tubular Secretion Tubular secretion is important for: Disposing of substances not already in the filtrate Eliminating undesirable substances such as urea and uric acid Ridding the body of excess potassium ions Controlling blood pH Tubular Secretion of K+ K+ is almost completely reabsorbed in the proximal tubule Aldosterone stimulates the tubular cells to secrete potassium if plasma levels are elevated K+ secretion occurs in the distal tubule As the basolateral pump transports sodium into the lateral spaces, it pumps potassium into the tubular cells where it diffuses into the lumen for elimination. Role of Aldosterone Acid-Base Balance Concentration of hydrogen ions is regulated sequentially by: Chemical buffer systems – act within seconds The respiratory center in the brain stem – acts within 1-3 minutes Renal mechanisms – require hours to days to effect pH changes Renal Mechanisms of Acid-Base Balance The most important renal mechanisms for regulating acid-base balance are: Conserving (reabsorbing) or generating new bicarbonate ions Excreting bicarbonate ions Losing a bicarbonate ion is the same as gaining a hydrogen ion; reabsorbing a bicarbonate ion is the same as losing a hydrogen ion Summary of Renal Response to Acidosis & Alkalosis Reabsorption of Bicarbonate Secreted hydrogen ions form carbonic acid with filtered bicarbonate Carbonic acid dissociates to release carbon dioxide and water Carbon dioxide then diffuses into tubule cells, triggering further hydrogen ion secretion and bicarbonate reabsorption Thus, bicarbonate disappears from filtrate at the same rate it is reabsorbed Figure 26.12 Generating New Bicarbonate Ions Dietary hydrogen ions must be counteracted by generating new bicarbonate Two mechanisms generate new bicarbonate ions: Both involve renal excretion of acid via secretion and excretion of hydrogen ions or ammonium ions (NH4+) The excreted hydrogen ions must bind to buffers in the urine (phosphate buffer system) Hydrogen Ion Excretion In response to acidosis: Kidneys generate bicarbonate ions and add them to the blood An equal amount of hydrogen ions are added to the urine H+ binds with buffers in the filtrate (monohydrogen phosphate) Figure 26.13 Ammonium Ion Excretion Another response to acidosis: This method uses ammonium ions produced by the metabolism of glutamine in PCT cells Each glutamine metabolized produces two ammonium ions and two new bicarbonate ions Bicarbonate moves to the blood and ammonium ions are excreted in urine Bicarbonate Ion Secretion When the body is in alkalosis, type B cells: Exhibit bicarbonate ion secretion Reclaim hydrogen ions and acidify the blood Varying Urine Concentration Kidneys excrete varying concentrations and volumes of urine depending on the body’s needs Can produce urine ranging from 0.3ml/min at 1200 mosm/L to 25 ml/min at 100 mosm/L Varying Urine Concentration This variation in reabsorption is made possible by a large, vertical osmotic gradient in the interstitial fluid of the medulla From 300 to 1200 mosm/liter This increase follows the juxtamedullary nephron’s loop of Henle deeper and deeper into the medulla. The gradient is established by means of the countercurrent system Varying Urine Concentration Countercurrent – the movement in opposite directions of filtrate through the ascending and descending limbs of the loop of Henle Also applies to the flow of blood through the vasa recta Countercurrent Mechanism Countercurrent multiplier – refers to the ability to increase the osmolarity of the interstitial fluid Due to the properties in the two limbs of the loop: The descending loop of Henle: Is relatively impermeable to solutes Is permeable to water The ascending loop of Henle: Is permeable to solutes Is impermeable to water Countercurrent Multiplier The ascending limb actively transports NaCl out of the tubular lumen into the surrounding interstitial fluid. It is impermeable to water. Therefore, water does not follow the salt by osmosis. The ascending limb produces an interstitial fluid that becomes hypertonic to the descending limb. This attracts the water by osmosis for reabsorption. Countercurrent Mechanism Countercurrent exchanger - The hairpin structure of the vasa recta allows the blood of the vasa recta to equilibrate with the interstitial fluid Prevents the dissipation of the medullary osmotic gradient Blood is isotonic when it enters and when it leaves the medulla Formation of Concentrated Urine ADH is the signal to produce concentrated urine Allowing the distal and collecting ducts to become permeable to water In the presence of ADH, 99% of the water in filtrate is reabsorbed Diuretics Osmotic diuretics include: High glucose levels – carries water out with the glucose Alcohol – inhibits the release of ADH Caffeine and most diuretic drugs – inhibit sodium ion reabsorption Lasix and Diuril – inhibit Na+-associated symporters Renal Processes Urine Excretion – elimination of what remains in the tubular lumen The unwanted filtrate material Transport and Storage of Urine Urine is transported from the kidney to the bladder by the ureters Due to gravity or peristaltic waves The bladder temporarily stores urine Micturition Reflex Micturition – act of emptying the bladder The filling of the bladder activates stretch receptors which trigger reflex contractions of the bladder and relaxation of the internal sphincter Urine is forced past the internal sphincter Must voluntary relax external sphincter to void the bladder of urine Micturition Reflex