Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
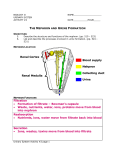
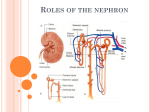
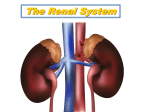
Chapter 25 Urinary System Urinary System • • • • Kidneys 2 Ureters 2 Urinary Bladder 1 Urethra 1 renal functions • • homeostasis of body fluids – – – – – chemical waste removal maintain blood volume maintain blood osmolarity maintain blood pH maintain electrolyte levels via: making urine gross anatomy • • • renal cortex outer renal medulla inner renal pelvis drains urine to ureter nephron anatomy • • • • nephron = functional unit of urine formation renal corpuscle – – glomerulus capillary network glomerular capsule = Bowman’s capsule renal tubules – – – PCT proximal convoluted tubule loop of Henle • descending and ascending limbs DCT distal convoluted tubule collecting duct (? part of nephron ) blood vessels • • • • • glomerulus capillary bed afferent arteriole into glomerulus efferent arteriole out of glomerulus peritubular capillaries – line convoluted tubules vasa recta – capillaries deep into medulla juxtaglomerular apparatus • juxtaglomerular cells produce renin surround afferent arteriole pressoreceptors • macula densa cells DCT/ ascending loop of Henle filtrate volume, osmolarity data • • • > 800 L /day blood into kidney 160 - 180 L/day blood filtered into nephrons 1 -2 L /day urine excreted (all other capillaries of body only 4 L/day) • filtrate fluid in nephron being processed • urine fluid out of nephron final product processes needed • • • • waste removal: – – a way to get wastes out of blood a way to get good stuff back into blood way to vary blood volume (BP) water way to vary blood osmolarity Na way to correct blood pH HCO3what happens where ? • • waste removal – – – early nephron filtration renal corpuscle bulk reabsorption PCT secretion of wastes PCT blood volume/osm control – – distal nephron varied reabsorption of Na DCT varied reabsorption of H2O collecting duct glomerular filtration • • • • filters fluid out of plasma into Bowman’s capsule glomerulus > 100x more permeable than other capillaries How big should the holes be? maintain BP must be high enough to force fluid into Bowman’s capsule – – 55 mmHg in glomerulus efferent arterioles thinner than afferent net filtration pressure • • • • • net filtration pressure NFP = force out - force in force out: – HPg glomerular hydrostatic pressure (BP) force in: – – OPg colloid osmotic pressure HPc capsular hydrostatic pressure NFP = HPg - (OPg + HPc) NFP = 55 - (30 + 15) = 10 glomerular filtration rate • • GFR = filtrate formed per minute – – (both kidneys) 120 – 125 ml / min 180 L / day factors: surface area membrane permeability NFP • NFP and GFR – – systemic BP NFP GFR dehydration NFP GFR GFR homeostasis • any change BP/Vol is a risk to GFR and waste elimination • GOAL: • – – constant GFR GFR too high lose nutrients , water GFR too low retain wastes note: constant GFR ≠ not constant urine volume Δ GFR ~ Δ NFP • • • to change GFR change glomerular BP 3 ways: – – – afferent arteriole ? efferent arteriole ? systemic BP ? afferent arteriole: – – vasodilate ? glomerular BP ? GFR vasoconstrict ? glomerular BP ? GFR GFR regulation • • intrinsic controls – afferent arteriole diameter extrinsic controls – – sympathetic hormones GFR intrinsic controls • • • GOAL: maintains constant GFR w/changing systemic BP • myogenic mechanism • = renal autoregulation Intrinsic corrects for extrinsic BP/volume changes – – – stretch smooth muscle - it contracts systemic BP afferent arteriole vasoconstriction “ “ vasodilation tubulo-glomerular feedback mechanism – – – GFR receptors = macula densa flow rate ; osmolality afferent vasodilation flow rate ; osmolality afferent vasoconstriction GFR extrinsic controls • • • • homeostasis of systemic BP , not renal BP GFR sympathetic n.s. – – vasoconstricts all blood vessels, afferent arteriole shunts blood to other organs for emergency GFR or unchanged renin-angiotensin mechanism – – – raises systemic BP juxtaglomerular cells produce renin angiotensin II systemic vasoconstriction GFR efferent vasoconstriction GFR autoregulation maintains minimal GFR changes tubular secretion • • • from peritubular capillaries into filtrate mostly in PCT adds stuff to filtrate : – – – wastes • creatinine , ammonia (NH4+) • urea , uric acid • medications and toxins to blood pH (DCT) H+ K + aldosterone (collecting ducts) tubular reabsorption • • • • • • reabsorbs the good stuff through tubular cells and capillary wall PCT most reabsorption here • all nutrients • electrolytes • water - glucose, AA, small proteins loop of Henle water DCT Na+ collecting ducts PCT - reabsorption of sodium • • diffusion into tubular cell (from filtrate) active transport from tubular cell to interstitial fluid – – Na / K pump provides energy for reabsorption of other solutes • diffusion into peritubular capillary • this creates: – – – osmotic pressure toward capillary electrical gradient anions follow + concentration gradient of all solutes • water follows Na • dilutes solute concentration in capillary PCT - passive reabsorption of solutes • • • anions – Cl- water – – follow Na HCO3osmosis obligatory water reabsorption lowers concentration of solutes in tubule cell and capillary solutes follow water – – – + toward low solute concentration = diffusion lipids urea cations K+ Ca++ Mg++ PCT - secondary active transport of solutes • cotransport with Na+ – – – Na+ active transport out of tubular cell Na+ diffuses into tubular cell solutes cotransport into tubular cell • fascilitated diffusion to capillary • transport maximum Tm • • – – max amt able to reabsorb each solute # carriers in cell membrane amino acids, cations, glucose glucose – – glucose Tm 375 mg/min hyperglycemia > Tm glucosuria PCT - other solutes • small proteins endocytosis • wastes not reabsorbed – – – urea from AA uric acid from nucleic acids creatinine from creatine loop of Henle - reabsorption • • reabsorbs some H2O and Na see countercurrent mechanism below early nephron review • • • • • • 25% of water , 10% of NaCl remain in filtrate at D CT wastes remain filtrate ~ 100 mOsm filtration and reabsorption is relatively constant in the not controlled by hormones early nephron distal nephron preview • • • • • we need to be able to: control blood volume (BP) control blood osmolarity this is done by varying: – – amount H2O reabsorbed amount Na reabsorbed this is controlled by: – – aldosterone ADH reabsorption in DCT and cortical Collecting Duct • • Na / K ATPase – – reabsorbs Na into blood secretes K into filtrate Aldosterone – – increases Na/K channels and ATPase stim by: low BP or BV (via angiotensin) low Na (via tubulo-glomerular mechanism) hyperkalemia effect of Aldosterone • result: increased blood osmolarity slight increase blood volume K loss • water reabsorbed only if ADH • same Na/K pump DCT vs PCT • – – PCT obligatory DCT only if Aldosterone water – – PCT obligatory DCT/CD only if ADH reabsorption in collecting duct • • • • • • water reabsorption = urine concentration DCT and Collecting ducts are impermeable to water require aquaporins ADH facultative water reabsorption osmosis no Na A.T. – water follows Na Na already in medulla why can’t we use Na pumps? effects of ADH • • • w/o ADH – – – : no water reabsorbed urine osmolarity ~ 100 mOsm maximum amt urine produced w/ ADH : – – water reabsorbed urine osmolarity varies facultative water reabsorption 300 – 1200 mOsm ADH • • • • • • • hypothalamus - posterior pituitary stim by: high blood osmolarity low BP via angiotensin affects tubule cells of CD G protein / cAMP system stim aquaporin production graded effect inhib by: alcohol diuretic drugs low osmolarity loop of Henle – a casual view • • • • reabsorbs Na and H2O from filtrate reabsorbs more Na than H2O leaves the excess Na in the medulla this high Na concentration has osmotic force at CD countercurrent mechanism • countercurrent mechanism flow in opposite directions • countercurrent multiplier loop of Henle • • – creates Na gradient in medulla countercurrent exchanger – vasa recta maintains Na gradient in medulla goal: Na gradient to reabsorb H2O from collecting ducts countercurrent multiplier • • • creates NaCl gradient in medulla ascending limb – – – active transport of NaCl to medulla impermeable to water maintains osmotic gradient of medulla descending limb – – NaCl out water out osmosis of water to medulla impermeable to NaCl • NaCl loss from ascending limb creates water loss from descending limb • Water loss from descending limb creates NaCl loss from ascending limb result of loop • • • decreased urine volume dilute urine ~ 100 mOsm creates Na gradient in medulla – for use by collecting duct countercurrent exchanger • • • • • • vasa recta maintains osmotic gradient of medulla reabsorbs NaCl and H2O from medulla leaves the extra NaCl in medulla NaCl – – descending vasa recta absorbs NaCl ascending vasa recta loses NaCl water – ascending vasa recta absorbs water via colloid oncotic pressure distal nephron review • increase blood osmolarity aldosterone • increase BV ; same OsM aldosterone + ADH • increase BV ; decrease OsM ADH • decrease BV and Osm ANP • dilute urine no hormones diuretics • • • • • • increase urinary output decrease blood volume decrease tissue edema glucosuria via osmotic diuresis alcohol inhibits ADH caffeine inhibits Na reabsorption (PCT) diuretic drugs inhibit Na pumps (DCT, ascending loop) – – Lasix diuril K sparing diuretics block K loss (DCT) allow Na reabsorption (PCT, Henle) renal clearance • • • • • • rate at which substance is removed from blood measures GFR and renal disease RC = UV / P U = concentration of substance in urine V = rate of urine formation P = concentration of substance in plasma renal clearance (part 2) • inulin amt excreted = amt filtered its RC = GFR ~ 125 ml/min used as standard • • RC < 125 substance reabsorbed RC > 125 substance secreted • glucose • drugs are secreted • contains: water wastes - urea, uric acid , creatinine urobilinogen electrolytes minerals • pH ~6 • abnormal glucose protein bacteria WBC RBC • pH balance RC = 0 completely reabsorbed RC used to determine dosage urine (4.5 – 8.0) other renal functions • • – H+ secretion / HCO3- reabsorption erythropoietin – RBC production Vit D – – – skin: cholesterol ergocalciferol kidney: ergocalciferol calciferol Ca absorption ++ (digestive) = active Vit D