Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
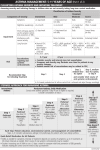
PATIENT & FAMILY ASSESSMENT Presented by: Michelle Harkins, MD This lesson will cover: • Medical history • Physical exam • Objective measures Initial Assessment & Diagnosis of Asthma Determine that: • Patient has a history or presence of episodic symptoms of airflow obstruction or hyperreactivity (wheeze, chest tightness, shortness of breath or cough). • Airflow obstruction is at least partially reversible. • Alternative diagnoses are excluded. NAEPP. EPR-3, page 40. Initial Assessment & Diagnosis of Asthma Methods for establishing diagnosis: • Detailed medical history (airway hyper-reactivity, recurrence, reversibility) • Physical exam • Spirometry to demonstrate reversibility • Additional studies as necessary to exclude alternative diagnoses NAEPP. EPR-3, page 40. Medical History Symptom history and Quality of Life Questionnaires: • History of symptoms of airflow obstruction – Cough – Wheeze – Chest tightness/pain – Shortness of breath • Episodic symptoms • Response to treatment Medical History • • • • Identify symptoms Pattern of symptoms Precipitating/aggravating factors Development of disease and treatment • Family history – Atopy, asthma NAEPP. EPR-3, page 69. Medical History • • • • Social history History of exacerbations Impact of asthma on patient/family Patient/family perception of the disease NAEPP. EPR-3, page 69 Interviewing the Individual with Asthma In the past 12 months, have you had: • A sudden, severe episode or recurrent episodes of coughing, wheezing or shortness of breath? • Colds that go to the chest or take more than 10 days to get over? • Coughing, wheezing or shortness of breath (SOB) during a particular season or time of the year? • Coughing, wheezing or SOB in certain places or when exposed to certain things, such as animals, tobacco smoke, perfumes? NAEPP. EPR-3, page 70 Interviewing the Individual with Asthma In the past 12 months, have you had: • Do you have symptoms of heartburn or awaken with an acid taste in back of your throat? • Do you have symptoms of post-nasal drip or sinus congestion? • Has wheezing, cough, chest tightness, shortness of breath – • Awakened you at night? • In the early morning? • After running, moderate exercise or other physical activity? NAEPP. EPR-3, page 70. Interviewing the Individual with Asthma In the past 12 months, have you had: • Have you used any medicine that has helped you breathe better? How often? • Are your symptoms relieved when these medicines are used? NAEPP. EPR-3, page 70. Early Asthma Signs & Symptoms Symptoms that indicate an asthma episode is occurring • • • • • Coughing Wheezing Shortness of breath Chest tightness and/or pain Peak-flow numbers usually 50% to 80% of personal best Other Early Warning Signs & Symptoms • Itchy throat or chin • Runny or stuffy nose • Sneezing • Headache • Funny feeling in the chest • Stomach ache/poor appetite • Glassy eyes • Feeling tired Late or Severe Asthma Symptoms Severe asthma symptoms are a life-threatening emergency. They indicate respiratory distress. Examples of severe asthma symptoms include: • Patient experiences severe coughing, wheezing, shortness of breath or tightness in the chest • Patient experiences difficulty talking or concentrating; mental deterioration may occur. • Walking causes shortness of breath. Severe Asthma Symptoms • Breathing may be shallow and fast, or slower than usual; paradoxical breathing in small children • Shoulders may be hunched. • Nasal flaring may be present. • Accessory muscle use and retractions may be present. – Retractions: Neck area and between or below the ribs moves inward with breathing Severe Asthma Symptoms • Skin may be gray or bluish tint, beginning around the mouth or fingernail beds (cyanosis). • Peak-flow numbers may be in the danger zone (usually below 50% of personal best). • Wheezing may be moderate, loud or absent. – The absence of wheezing implies severely compromised airflow. Severe Asthma Symptoms Pulses Paradoxus: • There is normally a decrease in systolic pressure during inspiration, When that difference is greater than 10 mmHg, it is called pulsus paradoxus. • A paradox is caused by a fall in cardiac output as a result of increased negative intrathoracic pressure. High-Risk Asthma Patients • • • • • • Past history of sudden, severe exacerbations Prior intubation for asthma Prior ICU admission for asthma >2 asthma hospitalizations in past year >3 asthma ER visits/year. Hospitalized/ER asthma visit in past month NAEPP. EPR-3, page 377. High-Risk Asthma Patients • • • • • • • >2 albuterol MDIs/month Low SES or inner city residence Poor perception of symptoms/severity Comorbidities Complex psychiatric/psychosocial problems Illicit drug use Sensitivity to Alternaria mold NAEPP. EPR-3, page 377. Physical Examination • The physical examination may be normal. • Absence of symptoms at the time of the examination does not exclude the diagnosis of asthma. NAEPP. EPR-3, page 377. Physical Examination The upper respiratory tract, chest, and skin are the focus of the physical exam for asthma. Physical findings that increase the probability of asthma include: • Hyper-expansion of the thorax, especially in children • Use of accessory muscles, appearance of hunched shoulders, chest deformity NAEPP. EPR-3, page 42. Physical Examination • Sounds of wheezing during normal breathing or a prolonged phase of forced exhalation (typical of airflow obstruction) -- In intermittent asthma, or between exacerbations, wheezing may be absent. • Increased nasal secretions, mucosal swelling, and/or nasal polyps • Atopic dermatitis/eczema or any other manifestation of an allergic skin condition NAEPP. EPR-3, page 43. What Is Your Differential Diagnosis? • What are some alternative diagnoses in adults that may present with similar symptoms? Alternative Diagnoses in Adults Chronic obstructive pulmonary disease – chronic bronchitis or emphysema Congestive heart failure Cough secondary to drugs (angiotensinconverting enzyme [ACE] inhibitors) NAEPP. EPR-3, page 46. Mechanical obstruction of the airways – benign and malignant tumors Vocal cord dysfunction Diagnosis of Asthma in Children • Signs and symptoms of asthma can vary widely and may mimic other common childhood illnesses. Diagnosis may be difficult. • Asthma is frequently under diagnosed. Not all wheeze and cough are caused by asthma. • Coughing may be the only symptom present. • Recurrent episodes of cough suggest asthma, but other causes must be ruled out. Alternative Diagnoses in Children Allergic rhinitis Sinusitis Gastroesophageal reflux Laryngotracheomalacia Bronchopulmonary dysplasia Cystic Fibrosis NAEPP. EPR-3, page 46. Alternative Diagnoses in Children Bronchiolitis Foreign body aspiration Congenital heart disease NAEPP. EPR-3, page 46. Vascular ring or laryngeal web Vocal cord dysfunction Objective Measures In addition to the physical exam, other measures include: • • • • • Radiology studies Spirometry Peak-flow monitoring Arterial Blood Gas /oxygen saturation Allergy testing Interpret the Findings from: • • • • Family, clinical and past medical history Physical examination Vital signs Pulmonary function, radiology and laboratory results Determine Diagnosis & Severity of Asthma Based on: • History and QOL questionnaire • Physical exam • Objective measures Classifying Asthma Severity: 0 – 4 years Components of Severity Persistent Intermittent Mild Moderate Severe Symptoms 2 days/week >2 days/week but not daily Daily Throughout the day Nighttime awakenings None 1-2x/ month 3-4x/month >1x/ week 2 days/week >2 days/week but not daily Daily Several times per day None Minor Limitation Some Limitation Extremely Limited Impairment B-agonist use (not prevention of EIB) Activity limits Risk Exacerbations requiring OSC 0-1/yr 2 exacerbations in 6 months requiring oral systemic corticosteroids, or 4 wheezing episodes/ 1 year lasting >1 day AND risk factors for persistent asthma Classifying severity in children who are not currently taking longterm control medication. Classifying Asthma Severity: 5 – 11 years Components of Severity Impairment Risk Persistent Intermittent Mild Moderate Severe Symptoms 2 days/wk >2 days/wk but not daily Daily Throughout the day Nighttime awakenings 2x/month 1-2x/month 3-4x/month >1x/wk B-agonist use 2 days/wk >2 days/wk but not daily Daily Several times per day Activity limits None Minor limitation Some Limitation Extremely limited Lung Function FEV1 FEV1/FVC >80% 80% 60 – 80% <60% >85% >80% 75 - 80% <75% Exacerbations requiring OSC 0-1/yr (not prevention of EIB) Classifying severity in children who are not currently taking longterm control medication. 2/year Classifying Asthma Severity: 12 and older Components of Severity Impairment Normal FEV1/FVC: 8-19yrs 85% 20-39yrs 80% 40-59yrs 75% 60-80yrs 70% Risk Persistent Intermittent Mild Moderate Severe Symptoms 2 days/wk >2 days/wk but not daily Daily Throughout the day Nighttime awakenings 2x/month 3-4x/month >1x/wk but not nightly Often 7x/week >2 days/wk but not daily, and not more than 1x on any day Daily Several times per day B-agonist use (not prevention of EIB) 2 days/week Activity limits None Minor limitation Some Limitation Extremely limited Lung Function FEV1 FEV1/FVC >80% 80% >60 -80% <60% normal normal reduced 5% reduced >5% Exacerbations requiring OSC 0-1/yr Classifying severity for patients who are not currently taking longterm control medication. 2/yr Spirometry Objective assessments of pulmonary function are necessary for the diagnosis of asthma because: • History and physical exam alone are not reliable for excluding other diagnoses or characterizing the status of lung impairment in the clinician’s office, • Spirometry is necessary for diagnosis, and • Peak-flow is used for monitoring control only NAEPP. Epr-3, page 43. Objective Measures: Spirometry • Spirometry measures how much and how quickly air can be expelled following a deep breath. • The patient breathes out forcefully into a device called a spirometer. • Pre- and post-bronchodilator spirometry should be done when a diagnosis of asthma is being considered. Spirometry Components • Forced Vital Capacity (FVC) The maximal volume of air forcibly exhaled from the point of maximal inhalation • Forced Expiratory Volume in 1 second (FEV 1) The volume of air exhaled during the first second of the FVC • Ratio of FEV1 to FVC (FEV1/FVC) Expressed as a percentage • Peak Expiratory Flow (PEF) Maximum air flow (rate) during forced exhalation Spirometry Results Airflow obstruction is indicated by reduced FEV1 and FEV1 /FVC values relative to reference or predicted values • The predicted values depend on the individual’s age, gender, height and race. • The numbers are presented as percentages of the average expected in someone of the same age, height, sex and race. This is called percent predicted. Calculating % Predicted FEV1 Predicted: 4.00L Patient’s FEV1: 3.00L What is the percent predicted for this patient? 3.00 = 3 = 75% 4.00 4 Objective Measures: Spirometry Abnormalities of lung function are categorized as restrictive and obstructive defects. • A reduced ratio of FEV1 / FVC, as compared to the predicted value, indicates obstruction to the flow of air from the lungs. • A reduced FVC with a normal FEV 1 /FVC ratio suggests a restrictive pattern. Interpreting Spirometry • Normal values for FEV1 and FVC are expressed in both absolute numbers and percent predicted of normal. • Values for FVC and FEV1 that are above 80% of predicted are defined as within the normal range. (The FEV1/FVC ratio is at least 80% of patient’s vital capacity in one second.) • FEV1/FVC ratio declines as a normal part of aging. Flow Volume Loop A normal flow volume loop has a rapid peak expiratory flow rate with a gradual decline in flow back to zero. Spirometry Results Showing Obstruction Measured Predicted Percent (%) Predicted FVC 4.09 4.25 96 FEV1 1.95 2.88 68 FEV1/FVC 48 68 PEF 6.27 8.06 78 Obstruction • Obstructive lung disease changes the appearance of the flow volume curve. • As with a normal curve, there is a rapid peak expiratory flow, but the curve descends more quickly than normal and takes on a concave shape. Normal vs. Obstructed Normal Obstruction Restrictive Lung Disease Both the FEV1 and FVC are reduced proportionately. FEV1/FVC ratio is normal or even elevated. Measured Predicted Percent (%) Predicted FVC 0.96 2.75 35 FEV1 0.94 1.90 49 FEV1/FVC 98 69 PEF 2.98 5.40 55 Restrictive Flow Volume Loop The shape of the flow volume loop is relatively unaffected in restrictive disease, but the overall size of the curve will appear smaller when compared to normals on the same scale. Objective Measures: Spirometry Is airflow obstruction present and is it at least partially reversible? Use spirometry to establish airflow obstruction FEV1 < 80% predicted FEV1/FVC below the lower limit of normal, as compared to the individual’s own predicted value Use spirometry to establish reversibility FEV1 increases >12% and > 200 mL after using a shortacting inhaled beta2-agonist 2- to 3-week trial of oral corticosteroid therapy may be required to demonstrate reversibility Calculating Change in FEV1 Pre BD FEV 1 = 2.00 L Post BD FEV 1 = 2.40 L What is the % improvement in FEV1? Example 1: 2.40 L – 2.00 L= .40 = 20% improvement 2.00L 2.00 Does this meet the NAEPP criteria? There is > 12% improvement. Calculating Change in FEV1 Post BD FEV1 minus Pre BD FEV1 Pre BD FEV 1 Pre BD FEV1 = 1.50L Post BD FEV1 = 1.80L What is the % improvement in FEV1? Example 2: 1.80L – 1.50L= .30 = 1 = 20% improvement 1.50L 1.50 5 Does this meet the NAEPP criteria? Calculating Change in FEV1 Post BD FEV 1 minus Pre BD FEV1 Pre BD FEV 1 Pre BD FEV 1 = 3.00L Post BD FEV1 = 4.00L What is the % improvement in FEV1? Example 3: 4.00L – 3.00L= 1.00 = 33% improvement 3.00L 3.00 Does this meet the NAEPP criteria? Calculating Change in FEV1 Second requirement is >200ml increase 1.15 L minus 1.00 L is improvement of 0.15 L or 150 ml Does this meet the NAEAPP requirement? (Post BD minus Pre BD = >200ml) Reliability of Spirometry • Spirometry is an effort-dependent maneuver that requires understanding, coordination and cooperation by the patient, who must be carefully instructed. • Technicians must be trained and maintain a high level of proficiency to assure optimal results. • Spirometry should be performed using equipment and techniques that meet standards developed by the American Thoracic Society. Reliability of Spirometry • Correct technique, calibration methods and maintenance of equipment are necessary to achieve consistently accurate test results. • Maximal patient effort in performing the test is required to avoid important errors in diagnosis and management (reproducibility). • Spirometry is generally valuable in children over age 4; however, some children cannot conduct the maneuver adequately until after age 7. Reliability of Spirometry Criteria for acceptability include: 1. Lack of artifact induced by coughing, glottic closure or equipment problems (primarily leak); 2. Satisfactory start to the test without hesitation; and 3. Satisfactory exhalation with six seconds of smooth continuous exhalation, or a reasonable duration of exhalation with a plateau. Unacceptable Efforts Cough Variable Effort Preparing Patients for Spirometry • Painless procedure • Noninvasive • Outpatient Spirometry Maneuvers • Normal breathing prior to test • Maximum forced exhalation during test • Maneuver repeated until results are consistent Discussing Results with Patients • Connect spirometry results to the broader picture of the patient’s asthma. • Explain that spirometry results can improve with effective asthma management. • Stress that effective asthma management can lead to less severe disease. NAEPP Recommends Spirometry 1. At the time of the initial assessment; 2. After treatment is initiated and symptoms and peak flow have stabilized to document attainment of (near) “normal” airway function; 3. During periods of loss of control; 4. When assessing response to a change in pharmacotherapy; and 5. At least every 1 to 2 years to assess the maintenance of airway function. NAEPP. EPR-3, pages 53, 59. Spirometry May Be Done More Frequently Depending on clinical severity, spirometry is also useful: • As a periodic check on the accuracy of the peak-flow meter, • When more precision is desired in evaluating response to therapy and • When peak flow results are unreliable. NAEPP. EPR-3, page 59. Peak Flow* • Measured as the largest expiratory flow achieved with a maximally forced effort from a position of maximal inspiration, expressed in liters/minute. • Spirometry documents PEFR in L/sec, so multiply this number by 60 to get L/min for noting personal best on the patient’s PFM. Peak-Flow Monitoring Long-term daily peak flow monitoring is helpful in managing patients with moderate-to-severe persistent asthma to: • Detect early changes in disease status that require treatment, • Evaluate responses to changes in therapy, • Provide assessment of severity for patients with poor perception of airflow obstruction and • Afford a quantitative measure of impairment. NAEPP. EPR-3, page 120 Radiological (CXR) Results • Not routine. • Usually normal yet hyperinflation may be present • Identify complications – – – – Pneumonia Pneumothorax Pneumomediastinum Tumor Arterial Blood Gas (ABG) Arterial blood gases are useful in assessing acutely ill patients. • Hypoxemia is generally not severe but does decline with worsening airflow obstruction. • CO2 is low in mild exacerbations and rises with severity of obstruction. • A normal CO2 in an acutely ill asthmatic can be a very serious finding. If the exacerbation progresses unabated, respiratory failure may result. • “Normal” 7.40/40/70 Periodic Assessments of Asthma Control • • • • • • Signs and symptoms Pulmonary Function Test QOL survey History of exacerbations Pharmacotherapy Patient satisfaction NAEPP. EPR-3, page 53. Assessing Control: 0 – 4 years Components of Control Impairment Well Controlled Not Well Controlled Very Poorly Controlled Symptoms 2 days/wk >2 days/wk Throughout the day Nighttime awakenings 1x/month >1x/month >1x/week Activity limits None Some limitation Extremely limited B-agonist use 2 days/week >2 days/week Several times per day 0-1/year 2-3/year >3/year • Maintain current treatment • Regular F/U every 1 – 6 mos • Consider step down if well controlled for at least 3 mos • Step up (1step) and • Reevaluate in 2 -6 wks • If no benefit in 6 wks, consider alternative diagnoses • Consider short course of OSC • Step up (1 – 2 steps) and • Reevaluate in 2 wks (not prevention of EIB) Risk Classification of Asthma Control Exacerbations requiring OSC Recommended Action for Treatment Asthma Control: 5 – 11 years Components of Control Symptoms Nighttime awakenings Impairment Well Controlled Not Well Controlled Very Poorly Controlled 2 days/wk but not >2 days/wk or multiple more than once on times 2 days/wk each day Throughout the day 1x/month ≥2x/month ≥2x/week Activity limits None Some limitation Extremely limited B-agonist use 2 days/wk >2 days/wk Several times per day (not prevention of EIB) Lung function • FEV1 or PF • FEV1/FVC Exacerbations requiring OSC Risk Classification of Asthma Control Reduction in lung growth Treatment-related adverse effects 80% >80% 60 – 80% 75-80% 0-1/year <60% <75% ≥2/year Evaluation requires long-term follow-up Medication side effects can vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk. Asthma Control: 12 and older Components of Control Impairment Well Controlled Not Well Controlled Very Poorly Controlled Symptoms 2 days/week >2 days/week Throughout the day Nighttime awakenings 2x/month 1-3x/week >4x/week Activity limits None Some limitation Extremely limited B-agonist use 2 days/week >2 days/week Several times per day (not prevention of EIB) Risk Classification of Asthma Control Lung function FEV1 or PF >80% QOL indicator ACT ≥20 Exacerbations requiring OSC 0-1/year FEV1 or PF = 60 -80% FEV1 or PF <60% ACT =16-19 ACT ≤15 > 2/ year Reduction in lung Evaluation requires long-term follow-up growth Treatmentrelated adverse effects Medication side effects can vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk. Occupational Asthma • Potential for workplace-related symptoms • Patterns of symptoms in relation to exposure • Documentation of work-relatedness of airflow limitation NAEPP. EPR-3, page 189. Classifying Severity of Asthma Mild Moderate Severe Subset: Life Threatening Symptoms and Signs Initial PEF (or FEV1) Dyspnea only with activity (assess tachyphena in young children) PEF ≥ 70 % predicted • Prompt relief with inhaled SABA or personal best Dyspnea interferes with or limits usual activity PEF 40-69 % • Relief from frequent inhaled SABA predicted or personal • OSC; some symptoms last for 1-2 best days after treatment is begun Dyspnea at rest; interferes with conversation Too dyspneic to speak; perspiring Clinical Course • Usually cared for at home • Possible short course of OSC • Usually requires office or ED visit PEF < 40 % predicted or personal best • Usually requires ED visit and likely hospitalization • Partial relief from frequent inhaled SABA • OSC; some symptoms last for >3 days after treatment is begun •Adjunctive therapies are helpful PEF <25 % predicted or personal best •Requires ED/hospitalization; possible ICU • Minimal or no relief from frequent inhaled SABA • Intravenous cortosteroids •Adjunctive therapies are helpful Referral to Specialist When: • A life-threatening asthma exacerbation exists, • Patient is not meeting goals of asthma therapy after 3-6 months of treatment, • Signs and symptoms are atypical or there are problems in differential diagnosis, • Comorbid conditions complicate asthma or its diagnosis and • Additional diagnostic testing is needed. Referral to Specialist When: • Additional education needed (about complications of therapy, adherence, allergen avoidance); • Patient is considered for immunotherapy; • Adult patient requires Step 4 or higher care – consider referral if patient requires Step 3; and • Pediatric patient requires Step 3 or higher care – consider referral if child 0-4 yrs requires Step 2 care. NAEPP. EPR-3, page 68. Case Reviews Review the pulmonary function results, then select the correct basic interpretation. Choose from the following answers: 1. Normal 2. Mild to moderate obstruction 3. Severe obstruction 4. Severe obstructive ventilatory defect, cannot exclude a concomitant restrictive defect 5. Restrictive ventilatory defect, large volumes necessary for confirmation 6. Cannot be interpreted; does not meet acceptability criteria. Acknowledgements • Sally W. Southard, PNP, BC, AE-C Pediatric Nurse Practitioner, Carilion Pediatric Pulmonology Clinic We will breathe easier when the air in every American community is clean and healthy. We will breathe easier when people are free from the addictive grip of cigarettes and the debilitating effects of lung disease. We will breathe easier when the air in our public spaces and workplaces is clear of secondhand smoke. We will breathe easier when children no longer battle airborne poisons or fear an asthma attack. Until then, we are fighting for air.