Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
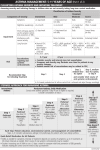
Easy Spirometry Interpretation Guide 5. A normal volume-time curve The most important tools for diagnosing COPD and asthma are medical history, physical examination, and spirometry. Interpreting your spirometry results correctly will help assure an accurate diagnosis and disease classification (severity). rises sharply from the baseline and reaches a flat plateau. A gradual curve that never plateaus suggests airway obstruction. Sample V/T curves 00 3 4 5 6 7 8 2. Look at the curve patterns and numbers to8 help guide your 5 6 7 olume (L) interpretation. 1 FEV1=4.0 L FEV1=1.8 L 2 Time (sec) that the quality of the spirometry test is good. Poor quality tests can cause diagnostic misclassifications. For more information, see 10 Steps to Good Results on our website. 3. A normal flow-volume curve looks like a sail, rising rapidly to a peak then descending at about a 45-degree angle. 4. A concave flow-volume curve 5 FVC=4.2 L FVC=5.0 L 6 Volume (L) suggests mild to moderate airways obstruction, while a prolonged finish “rat’s tail shape” suggests severe obstruction. Note: If the effort stops before 6 seconds in adults (3 seconds in children) the FVC may be underestimated. Normal Moderate Obstruction Severe Obstruction Sample F/V curves 14 13 12 11 10 9 8 7 6 respiratory symptoms and normal spirometry, consider performing a post-BD test to identify intermittent or mild asthma which is confirmed by a >12% improvement in FEV1, despite normal pre-BD spirometry results. 9. Adult onset airway obstruction in the long-term smoker (>10 to 20 pack year history) is usually due to COPD. 10. Once a diagnosis of asthma or COPD has been determined, disease classification and approTo view additional curve samples, priate treatment can be easily 1 2 3 4 5 6 7 8 00 see Sample Spirometry Tracings established by utilizing the Normal on our website. Severe Obstruction corresponding tables on the 1 6. A low (< 70% pred) FEV1% following page. FEV1=4.0 L (FEV1/FVC) indicates FEV1=1.8 L airway If a diagnosis is still uncertain, obstruction. A low (< 80% pred) 2 consider referral to a specialist FVC and FEV1 with a normal for consultation or co-manageFEV1% suggests restriction with3 ment. out obstruction. However, to make a definitive diagnosis of restrictive lung 4disease, the patient should be referred to a pulmonary lab for additional lung 5 Jones Medical Instrument Company volume testing. FVC=5.0 L 200 Windsor Drive, Oak Brook, IL 60523 FVC=4.2 L Time (sec) 5 airway obstruction should receive a post-BD (bronchodilator) spirometry test. After administration of a bronchodilator (i.e., albuterol, 2-4 puffs of 90 mcg/puff), allow 10-15 minutes prior to performing the post BD spirometry test. An increase of 12% (and more than 0.2 liters) in the measured FEV1 suggests reversible airways disease, such as asthma. COPD can be as much as 5-6% reversible, but not much more. For more information, see Differential Diagnosis on our website. 8. In patients with intermittent 3 4 4 Flow (L/sec) 2 Normal Severe Obstruction 1. The first step is to make sure 4 3 2 1 0 1 7. Patients with symptoms and 1 2 3 4 Volume (L) 5 6 7 8 (800) 323-7336 • www.jonesmedical.com 6 ©2008 Jones Medical Instrument Company. All Rights Reserved. Volume (L) Classification: First, identify the appropriate classification chart below. Then simply reference the patients’ post-BD spirometry results to determine an accurate classification and treatment regimen. CLASSIFYING ASTHMA SEVERITY IN CHILDREN 5 - 11 YEARS OF AGE STEPWISE APPROACH FOR MANAGING ASTHMA IN CHILDREN 5 - 11 YEARS OF AGE Assessing severity and initiating therapy in children who are not currently taking long-term control medication Classification of Asthma Severity (5 - 11 years of age) Components of Severity Symptoms Nighttime awakenings Short acting beta2-agonist use for symptom control (not prevention of EIB) Interference with normal activity Moderate Severe ≤2 days/week >2 days/week but not daily Daily Throughout the day ≤2x/month 3 - 4x/month >1x/week but not nightly Often 7x/week Daily Several times per day >2 days/week but not daily ≤2 days/week None Minor limitation • FEV1 >80% predicted • FEV1/FVC >85% • FEV1 = >80% predicted • FEV1/FVC >80% 0 - 1/year Exacerbations requiring oral systemic corticosteroids Some limitation • FEV1 = 60-80% predicted • FEV1/FVC = 75-80% • FEV1 <60% predicted • FEV1/FVC < 75% Step 3, medium- Step 3, medium-dose dose ICS option ICS option or Step 4 and consider short course of oral systemic corticosteroids Step 2 In 2 - 6 weeks, evaluate level of asthma control that is achieved, and adjust therapy accordingly CLASSIFYING ASTHMA SEVERITY IN YOUTHS ≥12 YEARS OF AGE AND ADULTS Preferred: Step 3 Preferred: High-dose ICS + LABA Step 2 Preferred: Medium-dose ICS + LABA Alternative: Preferred: EITHER: Alternative: High-dose ICS + either LTRA or Theophylline Step 1 Low-dose ICS Preferred: Alternative: SABA PRN Cromolyn, LTRA, Nedocromil, or Theophylline Low-dose ICS + either LABA, LTRA, or Theophylline OR Medium-dose ICS Medium-dose ICS + either LTRA or Theophylline Preferred: High-dose ICS + LABA + oral systemic corticosteroid Alternative: High-dose ICS + either LTRA or Theophylline + oral systemic corticosteroid Each Step: Patient education, environmental control, and management of comorbidities. Steps 2 - 4: Consider subcutaneous allergen immunotherapy for patients who have allergic asthma. Step up if needed (first, check adherence, inhaler technique, environmental control, and comorbid conditions) Assess control Step down if possible (and asthma is well controlled at least 3 months) Quick-Relief Medication for All Patients • SABA as needed for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at 20-minute intervals as needed. Short course of oral systemic corticosteroids may be needed. • Caution: Increasing use of SABA or use >2 days a week for symptom relief (not prevention of EIB) generally indicates inadequate control and the need to step up treatment. STEPWISE APPROACH FOR MANAGING ASTHMA IN YOUTHS ≥12 YEARS OF AGE AND ADULTS Assessing severity and initiating treatment for patients who are not currently taking long-term control medications Classification of Asthma Severity ≥12 years of age Mild Moderate Severe ≤2 days/week >2 days/week but not daily Daily Throughout the day Nighttime awakenings ≤2x/month 3 - 4x/month >1x/week but not nightly Often 7x/week Short acting beta2-agonist use for symptom control (not prevention of EIB) ≤2 days/week Daily Several times per day Symptoms Impairment Normal FEV1/FVC: 8 - 19 yr 85% 20 - 39 yr 80% 40 - 59 yr 75% 60 - 80 yr 70% Interference with normal activity None Lung function • Normal FEV1 between exacerbations • FEV1 >80% predicted • FEV1/FVC normal Risk Minor limitation • FEV1 >80% predicted • FEV1/FVC normal Some limitation • FEV1 >60%, but <80% predicted • FEV1/FVC reduced 5% Extremely limited • FEV1 <60% predicted • FEV1/FVC reduced >5% Step 3 Step 1 Step 2 II: Moderate FEV1 ≥ 80% predicted • • FEV1/FVC < 0.70 50% ≤ FEV1 < 80% predicted Step 2 Step 1 Step 4 or 5 and consider short course of oral systemic corticosteroids III: Severe • • FEV1/FVC < 0.70 30% ≤ FEV1 < 50% predicted IV: Very Severe • • FEV1/FVC < 0.70 FEV1 < 30% predicted or FEV1 < 50% predicted plus chronic respiratory failure Alternative: SABA PRN Cromolyn, LTRA, Nedocromil, or Theophylline Low-dose ICS + LABA OR Medium-dose ICS Alternative: Preferred: Step 4 Preferred: Preferred: High-dose ICS + LABA Medium-dose ICS + LABA AND AND Consider Omalizumab for patients who have allergies Consider Omalizumab for patients who have allergies Alternative: Medium-dose ICS + either LTRA, Theophylline, or Zileuton High-dose ICS + LABA + oral corticosteroid Low-dose ICS + either LTRA, Theophyline, or Zileuton Steps 2 - 4: Consider subcutaneous allergen immunotherapy for patients who have allergic asthma. (first, check adherence, environmental control, and comorbid conditions) Assess control Step down if possible (and asthma is well controlled at least 3 months) • SABA as needed for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at 20-minute intervals as needed. Short course of oral systemic corticosteroids may be needed. • Use of SABA >2 days a week for symptom relief (not prevention of EIB) generally indicates inadequate control and the need to step up treatment. Visit the Links page on our website for complete versions of the asthma and COPD guidelines. Note: This information is intended to augment, not replace, a physician’s independent professional judgment. NHLBI/WHO. GOLD COPD Guidelines; 2006 Revised NHLBI. Guidelines for the Diagnosis and Management of Asthma: Expert Panel Report 3: 2007 Add inhaled glucocorticosteroids if repeated exacerbations Add long-term oxygen if chronic respiratory failure. Consider surgical treatments Step up if needed Quick-Relief Medication for All Patients 2 Add regular treatment with one or more long-acting bronchodilators (when needed); Add rehabilitation Preferred: Step 6 Each Step: Patient education, environmental control, and management of comorbidities. 1 Active reduction of risk factor(s); influenza vaccination Add short-acting bronchodilator (when needed) Low-dose ICS Preferred: ≥2/year Consider severity and interval since last exacerbation. Frequency and severity may fluctuate over time for patients in any severity category. Relative annual risk of exacerbations may be related to FEV1. COPD CLASSIFICATION AND TREATMENT I: Mild Step 5 Preferred: In 2 - 6 weeks, evaluate level of asthma control that is achieved, and adjust therapy accordingly FEV1/FVC < 0.70 Consult with asthma specialist if Step 4 care or higher is required. Consider consultation at Step 3. Step 3 >2 days/week but not daily, and not more than 1x on any day 0 - 1/year Exacerbations requiring oral systemic corticosteroids Recommended Step for Initiating Therapy • • Persistent Asthma: Daily Medication Intermittent Asthma Persistent Intermittent 1 Step 4 Step 6 ≥2/year Step 1 Components of Severity COPD Step 5 Extremely limited Consider severity and interval since last exacerbation. Frequency and severity may fluctuate over time for patients in any severity category. Relative annual risk of exacerbations may be related to FEV1. Recommended Step for Initiating Therapy ASTHMA2 Mild • Normal FEV1 between exacerbations Lung function Risk Consult with asthma specialist if Step 4 care or higher is required. Consider consultation at Step 3. Persistent Intermittent Impairment Persistent Asthma: Daily Medication Intermittent Asthma Jones Medical Instrument Company 200 Windsor Drive, Oak Brook, IL 60523 (800) 323-7336 • www.jonesmedical.com ©2008 Jones Medical Instrument Company. All Rights Reserved.