Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
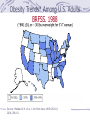
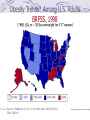
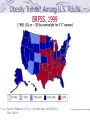
Part I – Eating Disorders: General Trends/Issues Early Eating Disorders Anorexia Nervosa Bulimia Nervosa Prevalence/Patterns Prevalence Increases in prevalence over past 4 years; changing norms regarding size and shape of women* Historically confined to middle to upper SES In college-age American women, 10 % or more have some symptoms of an eating disorder Estimated to occur in 0.5% to 3% of all teenagers Among athletes and performers, range from 15% to 60%. Gender & Age Differences 90-95% of affected individuals are female Little is known about nature of disorder in males Less frequently occurs before adolescence or after age 25 *Prorated Trend of Women’s Actual Body Weights Compared with the Trend for Playboy Centerfolds & Miss America Contestants General Risk Factors Self-Ideal Body Image Discordance General sociocultural norms idealizing extremes of thinness in women in Western cultures This pressure may lead to development of intrusive and pervasive perceptual biases regarding how fat they are Lead women to believe that men prefer more slender shapes than they in fact do Related to decreases in self-esteem usually apparent during mid-adolescence in girls While women’s actual weight has been increasing over past four decades, the weight of cultural beauty icons has decreased at the same rate Barbie Doll Interesting Facts In 1945 Ruth and Elliot Handler form Mattel. In 1957 Ruth conceives of a three dimensional adultlike doll. The body is based on German doll called "Lilli" which is sold as a sex toy for men. If Barbie was human sized, she would stand 5 foot 6 inches tall, weigh 110 pounds, and have a 39 inch bust, 18 inch waist and 33 inch hips. General Risk Factors Developmental Risk Factors Continuum of “eating pathology” from pickiness and dieting to clinical syndromes Early eating habits: stability of problem eating in young children (e.g., pickiness, binging, pica (eating non-food items)) Drive for thinness: key motivational factor underlying dieting and body image (e.g., “losing weight will make them like me more”) Dieting: between grades 5-8, 1/3 students diet and 45% want to lose weight Biological Resistance to weight change Bodies will resist, and try to compensate, for marked variation from one’s “set point” (individual norm) Physiological compensations include enhanced hunger drive and slowing of metabolism at decreased caloric intake Early Eating Disorders Feeding Disorder of Infancy or Early Childhood Sudden or marked deceleration of weight gain in an infant or young child and a consequent slowing of emotional and social development. Relatively common (up to 1/3 of infants affected); more often found in high-risk families, where abuse or neglect may be present Outcome depends on timing and level of intervention Failure to Thrive Weight below 5th percentile for age, and/or deceleration in rate of weight gain from birth to present of at least 2 standard deviations Been associated with poor attachment, poverty, family disorganization, limited social support Outcome highly related to child’s home environment Pica Early Eating Disorders Ingestion of inedible substances for period at least 1 month Affects mostly very young kids and those with MR Causes: poor stimulation and supervision in the home; in some cases of MR also genetic/biological factors Severity often related to degree of environmental deprivation and intellectual impairment Most clinical interventions emphasize operant conditioning Shaping and reinforcement of appropriate eating behavior Anorexia Nervosa Core Characteristics Refusal to maintain body weight at or above a minimally normal weight for age and height (less than 85%) Intense fear of gaining weight of becoming fat, even though under-weight Disturbance in experience of body weight or shape by selfevaluation, or denial of seriousness of current low weight Amenorrhea (absence of 3 consecutive menstrual cycles) Two Types: Restricting Type Binge-Eating/Purging Type Anorexia Nervosa Associated Features Comorbid Conditions Depression OCD & extreme self-control (in restricting types) Substance abuse disorders (in binge-eating/purging type) Personality disorders (esp. anxious-fearful) Behavioral Patterns Isolation from peers; social awkwardness Severe dietary restriction, excessive exercise (RT) Misuse of laxatives, diuretics, enemas, self-induced vomiting (B-E/PT) Anorexia Nervosa Specific Risk Factors Personality Characteristics Emotionally reserved and cognitively inhibited Preference for routine, order, and predictable environments; poor adaptation Show heightened conformity and deference to others Avoid risk and react to stressful events with strong feelings of distress Focus excessively on perfectionism Maturity fears Family Patterns Mothers described as: excessively dominant, intrusive, overbearing, and less affectionate, discouragement of autonomy Fathers described as: emotionally absent Families described as: limited tolerance of disharmonious affect or tension, poor conflict resolution skills, preoccupation with desirability of thinness, dieting, and good physical appearance Anorexia Nervosa Treatment Goals Stabilize Patient Restoring hormonal function and bone density Maximize chances for full and lasting recovery Treatment Components Hospitalization Renourish and reestablish weight to ensure survival Psychological Treatment (Out/Inpatient) Family therapy Cognitive-behavioral therapy Nutritional counseling Anorexia Nervosa Prognosis: Long-term Physical Effects Heart disease Most common medical cause of death in people with severe anorexia. Heart develops dangerous rhythms, blood flow is reduced and blood pressure may drop, heart muscles starve, losing size Cholesterol levels tend to rise Electrolyte Imbalances Anemia Reproductive and Hormonal Abnormalities Low levels of reproductive hormones& changes in thyroid hormones Neurological Problems Nerve damage and seizures, disordered thinking, loss of feeling, or other nerve problems in the hands or feet. Structural changes and abnormal activity during anorexic states; some damage may be permanent. Anorexia Nervosa Prognosis At this time, no treatment for anorexia is completely effective. Many remain very thin and displayed characteristics of the disorder, including perfectionism and drive for thinness, that keep them at risk for recurrence of the eating disorder. Recovery can take between 4 and nearly 7 years. Comorbid disorders increase for poor outcome. Risk of Death Death rates ranging from 4% to 20%. The risk for early death is twice as high in bulimic anorexics as it is in the anorexic-restrictor types. Increased suicide rates. Bulimia Nervosa Core Characteristics Recurrent episodes of binge eating Eating in a discrete period of time (i.e. 2hrs) an amount of food that is definitely larger than most people would in similar circumstances A sense of lack of control over eating during the episode Recurrent inappropriate compensatory behavior to prevent weight gain, such as self-induced vomiting, misuse of laxatives, diuretics, enemas, or medications, fasting, or excessive exercise Both behaviors occur on average at least twice a week for 3 mos Self-evaluation unduly influenced by body shape and weight Two Types: Purging Type Non-purging type Bulimia Nervosa Associated Features Comorbid Conditions Anxiety disorders (esp. GAD) Substance use disorders Personality disorders (esp. Cluster B – emotional, dramatic, emotional, erratic) Behavioral Patterns Purging types show greater physical and psychological dysfunction Preoccupation with efforts to conceal disorder and master impulse to binge Binge episodes usually involve intake of about 1000 calories approx. 14 times per week Bulimia Nervosa Specific Risk Factors Personality Characteristics Long-standing pattern of excessive perfectionism Negative self-evaluation Maturity fears Impulsivity Family Patterns High parental expectations Other family members dieting Higher criticism by family members about shape, weight, or eating Decreased allowance for autonomy Bulimia Nervosa Treatment Antidepressants Cognitive-Behavioral Therapy Clearly superior to medication Emphasis on normalizing eating patterns Temporal regularity Social eating Focus on distorted cognitive patterns Dichotomous thinking Bulimia Nervosa Prognosis Less major health problems associated with bulimia, where normal weight is maintained In general, the outlook is better for bulimia than for anorexia. Mortality rate about 1% for those in treatment; 20% have life-long patterns of disorder Physical Effects Teeth erosion, cavities, and gum problems Loss of fluid and low potassium levels Acute stomach distress, rupture of the esophagus, or food pipe Boys and Body Image Growing awareness regarding the pressure men and boys are under to appear muscular. Many males are becoming insecure about their physical appearance as advertising images raise the standard and idealize well-built men. Alarming increase in obsessive weight training and the use of anabolic steroids and dietary supplements that promise bigger muscles or more stamina for lifting. Number of boys affected is increasing and that many cases may not be reported, since males are reluctant to acknowledge any illness primarily associated with females. Part II - Obesity: An Epidemic Current Treatments A New Approach: BCT Obesity Trends* Among U.S. Adults BRFSS, 1985 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1986 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1987 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1988 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1989 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1990 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1991 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1992 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1993 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1994 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1995 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1996 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1997 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1998 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 1999 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 2000 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. Obesity Trends* Among U.S. Adults BRFSS, 2001 Source: Mokdad A H, et al. J Am Med Assoc 1999;282:16, 2001;286:10. A National Crisis The rates of overweight and obese individuals have been steadily climbing. Rates of obesity alone have doubled in the last decade. 1998, the World Health Organization labeled Obesity “an Epidemic.” 65% of the population are now either overweight or obese (2004). The trend is continuing with no end in sight. Who is Overweight or Obese? Height-Weight Tables >120% desirable weight BMI (kg of body weight / height (in meters) squared) Normal < 25 kg/m2 Overweight Class I Obesity Class II Obesity Class III Obesity Percent Fat 25-30 30-34.99 35-39.99 >40 >25% males; >32% females Waist Circumference >40 in. males; >35 in. females Physical & Emotional Burdens Risk of major chronic diseases increases with increases in BMI and central obesity: Metabolic Syndrome Cardiovascular Diseases Type 2 Diabetes Cancers Osteoarthritis Sleep Apnea Gall bladder Disease Psychological Disorders Social and Employee Discrimination The Financial Burden $100 billion dollars spent annually on obesity-related health care utilization. $329.2 billion dollars spent in 2002 on CVDrelated illness. $50 billion dollars spent annually on diet related products. The Ultimate Cost Direct link between Obesity and Years of Life Lost (Fontaine et al, 2003) Young adults with morbid obesity had a 22% reduction in life span. Ethnic differences in optimal BMI 23 to 25 for Caucasian (men and women) 23 to 30 was optimal for African American (men and women). Obesity-related illness accounts for >280k deaths annually (Manson, 2003) Obesity mortality is positively correlated with CVD mortality 950,000 people die each year from cardiovascular disease (CDC, 2003) Deaths in the Thousands US Cardiovascular Disease Rates 520 Men Women 500 480 460 440 420 400 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 0 Years Cardiovascular disease mortality trends for males and females in the United States, 1979-2000. Reprinted from the American Heart Association. Explanation Biological Psychological Social Engel, 1977, 1980; Schwartz, 1982