Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
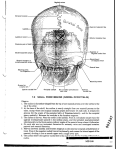
Greater Occipital Nerve Block John B. Ward, M.B., B.Ch.1 ABSTRACT The occipital nerve block is used to diagnose and treat occipital neuralgia. The clinical presentation of occipital neuralgia, the anatomy of the greater occipital nerve, and the technique of the occipital nerve block is described. KEYWORDS: Occipital neuralgia, occipital nerve block Objectives: Upon completion of this article, the reader will understand the clinical presentation of occipital neuralgia and the technique of greater occipital nerve block. Accreditation: The Indiana University School of Medicine is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. Credit: The Indiana University School of Medicine designates this educational activity for a maximum of 1.0 hours in category one credit toward the AMA Physicians Recognition Award. Each physician should claim only those hours of credit that he/she actually spent in the educational activity. Disclosure: Statements have been obtained regarding the author’s relationships with financial supporters of this activity. There is no apparent conflict of interest related to the context of participation of the author of this article. INDICATIONS The occipital nerve block has been traditionally used to diagnose and treat pain in the distribution of the occipital nerves (occipital neuralgia), which includes the greater and lesser occipital nerves. The International Headache Society specifically defines occipital neuralgia as the pain that is relieved by local anesthetic block of the involved nerve, thereby confirming the diagnosis. Other pathologies that may cause occipital nerve irritation and pain in its distribution include arthritis of the C2 cervical spine, myofascial spasm, and referred pain from the ipsilateral trigeminal distribution through interneuronal connections within the spinal cord. The trigeminal spinal nucleus and the C2 root are in close proximity so local anesthetic blocks to the occipital nerve may also decrease pain in the ipsilateral trigeminal distribution.1 CLINICAL PRESENTATION Occipital neuralgia as described by the International Headache Society is a paroxysmal jabbing pain in the distribution of the greater or lesser occipital nerves ac- companied by diminished sensation or dysesthesia in the affected area. It is associated with tenderness over the affected nerve. Criteria for diagnosis include: (1) pain in the distribution of the greater or lesser occipital nerves; (2) a stabbing quality pain that occurs in paroxysms, which may ache between paroxysms; (3) the affected nerve is tender to palpate; and (4) the condition is relatively easily treated with local anesthetic. The history and physical examination may elucidate the cause of the occipital neuralgia in a particular patient. If there is a strong history of myofascial irritation with trigger points in the back of the neck and trapezius muscles, it is likely that chronic muscle tension and spasm are contributing to the irritation of the occipital nerves. This presentation is commonly bilateral but can be unilateral. Occipital neuralgia may also present in the context of migraine headaches with associated signs and symptoms. This presentation usually lasts from 1 to 3 days and is typically unilateral. The pain may respond dramatically to vasoconstrictor therapy. Occipital neuralgia may be due to craniocervical junction disease, which may be degenerative or traumatic in origin. It is impor- Neurological Office Procedures; Editor in Chief, Karen L. Roos, M.D.; Guest Editor, Karen L. Roos, M.D. Seminars in Neurology, Volume 23, Number 1, 2003. Address for correspondence and reprint requests: John B. Ward, M.B., B.Ch., Department of Anesthesia, Indiana University School of Medicine, 1120 South Drive, FH 204, Indianapolis, IN 46202. 1Associate Professor of Clinical Anesthesia, Indiana University School of Medicine, and Director, Indiana University Chronic Pain Clinic, Indianapolis, Indiana. Copyright © 2003 by Thieme Medical Publishers, Inc., 333 Seventh Avenue, New York, NY 10001, USA. Tel: +1(212) 584-4662. 0271-8235,p;2003,23,01,059,062,ftx,en;sin00228x. 59 60 SEMINARS IN NEUROLOGY/VOLUME 23, NUMBER 1 2003 tant to obtain appropriate spinal imaging together with a careful neurological examination to confirm this diagnosis. ANATOMY The greater occipital nerve arises from the dorsal ramus of the second cranial nerve (Fig. 1).2 It provides cutaneous innervation to the major portion of the posterior scalp. It originates in the posterior neck, lateral to the lateral atlantoaxial joint and deep to the oblique inferior muscle where a communicating branch from the third cranial nerve may join the greater occipital nerve. The greater occipital nerve ascends in the posterior neck over the dorsal surface of the rectus capitis posterior major muscle, and then turns dorsally to pierce the fleshy fibers of the semispinalis capitis, after which it runs a short distance rostrally and laterally, and lies deep to the trapezius muscle. The greater occipital nerve becomes subcutaneous slightly inferior to the superior nuchal line by passing above an aponeurotic sling. This sling is composed of insertions from the trapezius and sternocleidomastoid muscles. At this point, the greater occipital nerve is immediately medial to the occipital artery. GREATER OCCIPITAL NERVE BLOCK TECHNIQUE The patient is usually positioned in the sitting position with the head either vertical or slightly flexed. The nerve is relatively easy to locate along the superior nuchal line, where it lies medial to the occipital artery, bilaterally. The pulsation of the occipital artery is easy to palpate. Palpation in this area may elicit a paresthesia or uncomfortable feeling in the distribution of the nerve. It is helpful if an assistant provides support for the head anteriorly. The scalp is prepped with alcohol. A mixture of local anesthetic and steroid is used, usually 2% lidocaine with either triamcinolone 10 to 20 mg or betamethasone 2 to 4 mg for a total volume of 3 mL of injectate. The technique is made easier if a control-type syringe is used for aspiration and injection, as this can be performed with one hand. Usually a 25 G needle, either 5⁄8 inch or 11⁄2 inch, can be used depending on the size of the patient. The needle is directed at 90 degrees toward the occiput until a bony endpoint is obtained. Aspiration is important to prevent intravascular injection, and in the case of a history of a cranial defect, to prevent injection into the cerebrospinal fluid. Approximately 1.0 cc is injected around the nerve and an additional 1.0 cc on either side of the nerve. When the needle is withdrawn, pressure should be maintained over the site of injection to both bathe the nerve trunk with the mixture and to achieve hemostasis as the scalp has a rich vascular supply. Ample time should be allowed for the local anesthetic to take effect, and the patient should be reevaluated in approximately 15 minutes. The lesser occipital nerves may be included by injecting more of the local anesthetic/steroid mixture lateral to the greater occipital injection along the superior nuchal line. If a small volume is used (approximately 1.0 cc) and is directed in the immediate vicinity of the greater occipital nerve, it is somewhat more definitive in distinguishing greater occipital neuralgia from surrounding myofascial-type pain, which will also be relieved by the injection of a larger volume. COMPLICATIONS There are relatively few complications because of the superficial location of the nerve. However, intravascular injection is a possibility. Careful aspiration is performed prior to injection to avoid toxicity. Also, in advance, one should elicit from the patient whether they have a cranial defect3 from prior surgery or trauma. Rarely, a patient may be rendered Cushingoid as a response to serial injections of corticosteroids.4 REFERENCES Figure 1 Anatomy of the greater occipital nerve. 1. Ploveran EJ, Kowacs PA, Tatsui CE, Lange MC, Ribas LC, Wernek LC. Referred pain after painful stimulation of the greater occipital nerve in humans: evidence of convergence of GREATER OCCIPITAL NERVE BLOCK/WARD cervical afferents on trigeminal nuclei. Cephalalgia 2001;21: 107–109 2. Anderson JE. Grant’s Atlas of Anatomy. 7th ed. Baltimore: Williams & Wilkins Co.; 1978 3. Okuda Y, Matsumoto T, Shinohara M, Kitajima T, Kim P. Sudden unconsciousness during a lesser occipital nerve block in a patient with the occipital bone defect. Eur J Anaesthesiol 2001;18:829–832 4. Lavin PJ, Workman R. Cushings syndrome induced by serial occipital nerve blocks containing corticosteroids. Headache 2001;41:902–904 61