Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
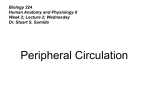
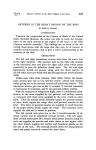
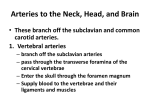
2008 THE AUTHORS. JOURNAL COMPILATION Reconstructive and Paediatric Urology 2008 BJU INTERNATIONAL ARTERIES OF THE SCROTUM CARRERA et al. BJUI Arteries of the scrotum: a microvascular study and its application to urethral reconstruction with scrotal flaps BJU INTERNATIONAL Anna Carrera, Alfredo Gil-Vernet*, Pau Forcada, Rosa Morro, Manuel Llusa and Octavio Arango† Department of Human Anatomy, Faculty of Medicine, University of Barcelona, * Department of Urology, Centro Médico Teknon, and †Department of Urology, Hospital del Mar, Barcelona, Spain Accepted for publication 10 July 2008 Study Type – Aetiology (case series) Level of Evidence 4 cases to evaluate the number, distribution and anastomosis of the cutaneous arteries of the scrotum. OBJECTIVE RESULTS To study scrotal microvascularization and apply the findings to the design of reliable skin flaps for reconstructive surgery of complex urethral or panurethral stenoses. Scrotal skin is irrigated by two main vascular systems, through the inferior external pudendal arteries and the perineal arteries, which branch into multiple scrotal arteries. These arteries are distributed in three cutaneous territories, two lateral and one central, which are widely inter-anastomosed. Each lateral territory receives an inferior external pudendal artery which accesses at the midpoint of the scrotal root and fans out to cover the entire corresponding hemiscrotum. The central cutaneous territory is vascularized through the branches of two main scrotal arteries which are a continuation of the perineal arteries and which access via the posterior face, running deeply on both sides of the septum. CONCLUSIONS MATERIALS AND METHODS In 15 cryopreserved male cadavers, scrotal skin vascularization was explored using macro- and microdissections, and the scrotal sac made transparent using the Spalteholtz method. A meticulous descriptive analysis of the arterial network was conducted out in all INTRODUCTION In any reconstructive surgery, axial flaps are more reliable than grafts, as the blood supply is always guaranteed when vascular continuity is well preserved [1]. Many penile and scrotal skin flaps to reconstruct complex urethral stenosis have been described, but most were not supported by previous microvascular studies, which could explain their variable outcomes. Scrotal skin is well vascularized due to the confluence of two main arterial systems, the external iliac and the internal iliac, as described in classic anatomical texts and atlases [2–7], and specialized books and texts on microvascular anatomy [8–10]; however, recent and well-detailed descriptions are scarce or unavailable. Our aim was to study the arterial microvascular distribution of the 820 scrotum and apply the findings to improving the results of complex urethral surgery. MATERIALS AND METHODS Fifteen cadavers of men aged 53–92 years, cryopreserved and with arterial black latex injected through the internal and external iliac arteries, were studied using a combination of different techniques. The bilateral inguinal regions and the perineoscrotal area were dissected to identify the origin of the main arterial vessels that vascularize the scrotum. Microdissections of scrotal cutaneous arteries using magnifying lenses (×2.5) were carried out from inside and outside the scrotal wall, with each layer identified and raised successively. The special anatomical distribution of scrotal branches stemming from perineal arteries enables the construction of adequate reliable longitudinal median island scrotal flaps for the reconstructive surgery of panurethral stenosis, as profuse axial vascularization is ensured. KEYWORDS arteries, blood supply, scrotum, surgical flaps, urethral stricture, urethroplasty To evaluate specific characteristics, disposition and anastomosis of the skin arteries, the scrotum was made transparent using the Spalteholtz technique [11] in which tissue is cleared by alcohol dehydration and impregnation with benzyl benzoate/methyl salicylate mixture. Sections were made in the frontal or sagittal planes in some of these preparations to attain better visualization of the vascular disposition. RESULTS Scrotal blood supply from the external iliac system: Two external pudendal arteries (superior and inferior) were found stemming from the femoral artery at a mean distance of 5 cm below the inguinal ligament in 95% of cases. One arterial trunk dividing into these © JOURNAL COMPILATION © 2008 THE AUTHORS 2 0 0 8 B J U I N T E R N A T I O N A L | 1 0 3 , 8 2 0 – 8 2 4 | doi:10.1111/j.1464-410X.2008.08167.x ARTERIES OF THE SCROTUM FIG. 1. Dissection of the inguinal region. 1. Femoral artery. 2. Superior external pudendal artery. 3. Inferior external pudendal artery. 4. Femoral vein. 5. Great saphenous vein. 6. Inguinal ligament. FIG. 2. Spalteholtz technique. A, Lateral view of scrotal sac. Scrotal arteries are long, tortuous and follow a descending course in scrotal layers. They fan out into branches emerging at acute angle from the main trunk. B, Superior view of the scrotal sac after removing the testes. Anastomosis is visible between great branches of scrotal vascularization from the external iliac and internal iliac systems. 1. Inferior external pudendal artery. 2. Great branch of perineal artery. 3. Corpus spongiosum. A FIG. 3. Landmarks of the emergence point of the perineal artery (lithotomy position). A, As indicated with the red ellipse, 75% of perineal arteries emerge at the middle third of the line between median raphe and ischial tuberosity. The remaining arteries emerge in the lateral third of this line but with a clear tendency to move away from the ischial tuberosity, as indicated by the green circle. B, Dissection of the course of perineal arteries to the scrotum. During their course, these arteries give off branches towards neighbouring anatomical structures. In the root of the scrotum, both perineal arteries are attached to the septum. 1. Perineal artery. 2. Superficial transverse perineal muscle. 3. Ischiocavernosus muscle. 4. Bulbospongiosus muscle. A two branches was found in 65% of cases (Fig. 1). B Scrotal vascularization was exclusively through branches of the inferior external pudendal artery in 89.5% of cases. Both external pudendal arteries or a single external pudendal artery were responsible for scrotal blood supply in the remaining cases. These arteries enter the scrotal sac laterally at the mid-point of its base or root, then bifurcate and are distributed throughout the entirety of the skin of each hemi-scrotum (Fig. 2). Scrotal blood supply from the internal iliac system: A perineal artery (superficial perineal artery) branching from the internal pudendal artery was located bilaterally in the perineal area in all cases. All these vessels gain access in the perineal region, perforating the perineal membrane in the triangular space formed in front of the superficial transverse muscle of the perineum, and between the ischiocavernosus and bulbospongiosus muscles. This emergence point was found at a mean distance of 1.9 cm lateral to the median perineal raphe, along the line joining the two ischial tuberosities passing through the anterior margin of the anal orifice. In depth, the arterial emergence point was at a mean of 4.5 cm from the cutaneous surface. Both superficial perineal arteries traced an anterosuperior route towards the rear face of the scrotum (lithotomy position), being located deep in the space between the ischiocavernosus and bulbospongiosus © B muscles (Fig. 3). At the root of the scrotum, each perineal artery splits into fine branches that are distributed in the skin of this area, and a main branch, of larger diameter, which continues a deep course towards the interior of the scrotal sac (Fig. 4). This main branch runs ventrally along the urethral corpus spongiosum at each side of the scrotal septum insertion, following an anterior direction, and branching out into several arteries that descend obliquely over the septum (Fig. 5). When these septal arteries reach the superficial end of the septum, they turn towards the skin of each hemiscrotum at the median line where they are distributed (Figs 6,7). In addition, in 70% of cases the skin of the superolateral region of the scrotum had supplementary irrigation from a lateral artery originating in the medial femoral circumflex artery (83% of cases) or in the obturator artery (17%). There were 2008 THE AUTHORS JOURNAL COMPILATION © 2008 BJU INTERNATIONAL 821 C A R R E R A ET AL. FIG. 4. The great branch of the perineal artery only gives off small, scant branches to the skin of the scrotal root. A, Microdissection of the posterior aspect of the scrotum (lithotomy position). All the skin has been removed laterally to the scrotal raphe. B, Spalteholtz technique. Posterior view of the scrotum. C, Spalteholtz technique. Frontal section and internal view of the posterior aspect of the left hemiscrotum. 1. Great branch of perineal artery on its route inside scrotal sac. 2. Branches of perineal artery to the skin of the scrotal root. 3. Scrotal septum. 4. Corpus spongiosum. 5. Skin. A B FIG. 5. A, Internal microdissection of scrotal sac. The scrotal septum and skin are in the same plane. Scrotal arteries run at different levels of the subcutaneous tissue of the scrotum. B, Transillumination of scrotal septum in the internal microdissection of the scrotal sac. C, Spalteholtz technique and frontal section of scrotum. The scrotal septum has two arterial planes with fine, scant communications between them. 1. Great branch of perineal artery. 2. Septal arteries. 3. Branches from inferior external pudendal artery. 4. Corpus spongiosum. 5. Scrotal septum. A C B The use of scrotal and penile skin flaps in reconstructive surgery of bulbar urethral stenosis has declined since the advent of free buccal mucosa grafts. However, there are cases of complex bulbar stenosis (very extensive, multi-operated and with chronic urinary infection) or panurethral disease in which reconstruction with a scrotal skin flap is an option to be considered before a definitive perineal urethrostomy. suitability and reliability. As classically described, scrotal skin has a dual blood supply through branches from the external and internal iliac systems, respectively, distributed in anterior and posterior faces of the scrotum [2,3,8]. However, our results show the existence of three cutaneous territories; two lateral and one central (Fig. 8). Classically and in recent texts, perineal arteries were considered to only irrigate the posterior face of the scrotum [9,10,16]; however, the present study showed that all the skin from the scrotal midline to its insertion into the mid penile raphe receives its vascularization via the perineal arteries and their branches. Different urethroplasty techniques with scrotal flaps have been described [12–16]; however, the design of most was based on the understanding of classical anatomy and not on microvascular studies, which might support the existence of axial-type vascularization and thus assure their Understanding of the exact anatomical location of these vessels is necessary to ensure their inclusion in the skin flap and avoid surgical manoeuvres that could harm them. In this respect, several surgical landmarks should be considered throughout their route. anastomoses between the arteries of each scrotal vascular region. DISCUSSION 822 C Regarding the exit point of these arteries in the perineal region, incisions at the base of a flap of the scrotal midline must move away laterally from ischial tuberosities to avoid injury. Fortunately, the characteristic deep exit site of both perineal arteries prevents them from being injured in their main trunk when a superficial skin incision is made. To ensure inclusion in the scrotal flap of the main trunk of both perineal arteries © JOURNAL COMPILATION © 2008 THE AUTHORS 2008 BJU INTERNATIONAL ARTERIES OF THE SCROTUM FIG. 6. Spalteholtz technique. A, Cutaneous surface of the scrotal midline. B,C, Frontal section of the scrotal septum and midline skin. Anastomoses are visible between vessels from septal arteries and vessels from inferior external pudendal artery. There are many vessels in the midline skin of the scrotum. 1. Septal arteries. 2. Branches from inferior external pudendal artery. 3. Septum. A FIG. 7. Spalteholtz technique. Inferior view of scrotum. Anastomoses are apparent among the arterial territories of the scrotum. 1. Branches from inferior external pudendal artery. 2. Branches from septal arteries. B C FIG. 8. Vascular scrotal territories. Branches from inferior external pudendal artery (in red) and branches from septal arteries (in orange). A, Anterior face of scrotum. B, Posterior face of scrotum. situated between the ischiocavernosus and bulbospongiosus muscles, it will be necessary to raise them within the plane of the fascia of these muscles or, even more safely, subfascially, while taking special care in the intermuscular space, as indicated in a perineally based scrotal flap urethroplasty [15]. The particular ventral route of both perineal arteries with respect to the corpus spongiosum of the urethra and exit of its branches towards the scrotal septum, advocate the routine inclusion of the septum in scrotal flap construction, and thus preserve this important vascularization. However, anatomical findings have shown that perineally based flaps of the scrotal midline © can be adequately designed in length and width without their vascularization being compromised. As the median line of scrotal skin, on the posterior and anterior faces, depends on vascularization through perineal arteries, posterior scrotal midline flaps are not limited in length and could be raised, with no risk, up to the anterior face of the scrotum. Thus, this permits long cutaneous island flaps to be obtained that can be moved and sutured free from tension. Confirmation of the existence of anastomosis between the arteries of the two lateral arterial territories with a central territory, forming a true scrotal network as described by several authors [8–10], permits the design of flaps of the scrotal central line with variable amplitude, without endangering the vascularization of their lateral zones. Finally, direct connections between the arteries of the right- and left-hand sides at the level of the scrotal skin of the median line could ensure vascularization of the whole flap in the event of lesions to the vascular supply of one of the sides of the septum. 2008 THE AUTHORS JOURNAL COMPILATION © 2008 BJU INTERNATIONAL 823 C A R R E R A ET AL. Some authors have described flaps for complex urethral reconstruction based on the distribution of perineal artery branches in other territories [14,16,17] or exclusively on the septal blood supply [13]. Without doubt, according to our results, a raised flap in the posterolateral scrotal skin is vascularized by fine branches of the ipsilateral perineal artery that are distributed in the area. Such a flap must be considered as a ‘random’ flap, given that it will remain nourished through arterial interconnections of the dartos, but will not count on an axial vessel making its vascularization totally predictable. Septum pedicled scrotal skin flaps are randomly vascularized by fine septal arteries that can be easily damaged when surgical incisions are deepened in the scrotal septum to obtain an adequate mobilization of the flap. the base of the penis) and variable width, thereby guaranteeing axial vascularization. The surgical execution of these flaps must respect certain important surgical landmarks and preferentially include the septum. 8 ACKNOWLEDGEMENTS 10 The authors thank Christine O’Hara for valuable help with the English version of the manuscript. 11 9 CONFLICT OF INTEREST 12 None. 13 REFERENCES In no case did we find a distribution of perineal artery branches in the superficial fascia of the internal thigh laterally contiguous to the inguinal fold, as described in diagrams of a urethroplasty technique for complex cases [16,17]. In conclusion, the scrotum receives a good arterial supply from two main arterial systems that determine the existence of three cutaneous territories; two lateral, each dependent on an inferior external pudendal artery, and one central, dependent on perineal arteries, which includes the anterior and posterior faces and the septum. The three territories are widely interconnected by a veritable scrotal arterial network. Microvascular anatomical study of the distribution of scrotal branches of the perineal artery permits the design of skin flaps of the central scrotal territory, sufficiently long (from the scrotal root to 824 1 2 3 4 5 6 7 McGregor IA, Morgan G. Axial and random pattern flaps. Br J Plast Surg 1973; 26: 202–13 Rouvière H, Delmas A. Anatomía Humana, 10th edn, Vol. II. Barcelona: Masson, 1999 Testut L, Latarjet A. Anatomía Humana, 8th edn, Vol. II/IV. Barcelona: Salvat, 1940 Gray H, Bannister LH, Berry MM, Williams PL. Gray’s Anatomy. The Anatomical Basis of Medicine and Surgery, 38th edn. London: Churchill Livingstone, 1995 Pernkopf E. Atlas of Topographical and Applied Human Anatomy, 3rd edn. Baltimore: Williams & Wilkins, 1989 Moore KL, Dalley AF. Clinically Oriented Anatomy, 5th edn. Philadelphia: Lippincott, Williams & Wilkins, 2005 Netter FH. The Netter Collection of Medical Illustrations – Musculoskeletal 14 15 16 17 System, Vol. 8, Part I. Philadelphia: WB Saunders, 1988 Salmon M. Arteries of the Skin. Taylor GI ed. London: Churchill Livingstone, 1988 Cormack GC, Lamberty GH. The Arterial Anatomy of Skin Flaps, 2nd edn. London: Churchill Livingstone, 1994 Quartey JKM. Microcirculation of penile and scrotal skin. Atlas Urol Clin N Am 1997; 5: 1–9 Culling CF. Handbook of Histopathological and Histochemical Techniques (Including Museum Techniques), 3rd edn. London: Butterworth, 1974 Blandy JP, Singh M. The technique and results of one-stage island patch urethroplasty. Br J Urol 1975; 47: 83–7 Yachia D. A new, one-stage pedicled scrotal skin graft urethroplasty. J Urol 1986; 136: 589–92 Gattegno B, Cohen L, Coloby P et al. Le traitement des sténoses de l’urètre par patch pédiculé de peau scrotale. Ann Urol 1990; 24: 43–7 Gil-Vernet JM, Arango O, Gil-Vernet A, Gil-Vernet JM Jr, Gelabert-Mas A. A new biaxial epilated scrotal flap for reconstructive urethral surgery. J Urol 1997; 158: 412–20 Jordan GH. Scrotal and perineal flaps for anterior urethral reconstruction. Urol Clin N Am 2002; 29: 411–6 Zinman L. Perineal artery axial fasciocutaneous flap in urethral reconstruction. Atlas Urol Clin N Am 1997; 5: 91–108 Correspondence: Anna Carrera Burgaya, Department of Human Anatomy, Faculty of Medicine, University of Barcelona, Calle Casanova, 143, 08034 Barcelona, Spain. e-mail: [email protected] © JOURNAL COMPILATION © 2008 THE AUTHORS 2008 BJU INTERNATIONAL