Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Infection control wikipedia , lookup
Vaccination policy wikipedia , lookup
Hepatitis B wikipedia , lookup
Whooping cough wikipedia , lookup
Hepatitis C wikipedia , lookup
Typhoid fever wikipedia , lookup
Immunocontraception wikipedia , lookup
Polio vaccine wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
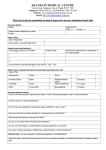
Travel Vaccine Questionnaire Personal detail Name Date of birth Telephone number Male [ ] female [ ] Date of trip Date of departure Return date or overall length of trip Itinerary and purpose of visit Countries to be visited Length of stay Away from medical help at destination, if so how remote? 1. 2. 3. Please tick as appropriate below to best describe your trip 1. Type of trip 2. Holiday type 3.Accomodation 4. Travelling 5. Staying in area which is 6. planned activities 7. Religious Pilgrimage Business package camping Hotel alone Urban safari Pleasure Self-organised Other Backpacking Cruise ship Relatives/family home With family /friend Rural Trekking other In a group Altitude Personal history Have you ever had a serious reaction to a vaccine given to you before? Have you recently undergone radiotherapy , chemotherapy or steroid treatment Women only: Are you pregnant or planning pregnancy or breast feeding? Have you taken out travel insurance and if you have medical condition informed the insurance company about this? Vaccine History- have you had any of the following vaccines before Tetanus Polio Typhoid Hepatitis A Meningitis Yellow fever Rabies Jap B enceph Other Diphtheria Hepatitis B Influenza Tick borne Malaria tablets Malaria tablets- for discussion when risk assessment is performed within your appointment. I have no reason to think that I might be pregnant. I have received information on the risks and benefits of the vaccines recommended and have had the opportunity to ask questions. I consent to the vaccines being given. Signed____________________________________ date______________________________________ PTO FOR OFFICIAL USE Patients name: Travel risk assessment performed yes [ ] no [ ] Travel vaccine recommended for this trip Disease protection Hepatitis A Hepatitis B Typhoid Cholera Tetanus Diphtheria Polio Meningitis ACWY Yellow fever Rabies Japanese B encephalitis other Yes No Patient declined vaccine Travel advice & leaflets given as per travel protocol Food, water & personal Travellers’ hygiene advice diarrhoea Insect bite prevention Animal bites Insurance Air travel Websites Travel record card supplied other Further information Blood and bodily fluid infection risks e.g. Hep B Accidents Sun & Heat protection Authorisation for patient specific direction (PSD) use Assessor’s name: ___________________________________signature_____________ date___________ Prescriber’s name:___________________________________signature_____________date____________ APPT REQUIRED : details APPT MADE : date/time/clinician