Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
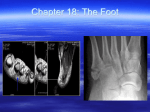
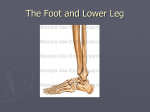
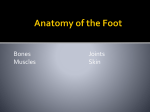
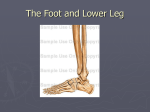
The foot • The foot – bony architecture, muscles, how it can be both pliable to walk on rough ground but also act as a solid lever at push off • The importance of the arches of the foot • The foot in normal gait and posture and its influence in abnormal alignment of the lower limb • Common conditions – hallux valgus (bunions), heel pain, hammer toes, plantar fasciitis Extreme functions of the foot Propulsion to jump Balance and propulsion for stairs From ballet dancer to elite athlete • 3 main functions • Weight transmission of the body weight to the ground in walking • Balance – maintains equilibrium of posture when walking and jogging • Assistance in ambulation – propulsion to move the body forwards during walking • It has to be both pliable to accommodate to rough ground and rigid in propulsion so that energy is utilised efficiently to propel the body forwards • The toes are designed to give a wider base for balance and for propulsion The bones of the foot • • • • Hind foot - talus and calcaneus Mid foot - navicular, cuboid and 3 cuneiform bones Forefoot – 5 metatarsals and the phalanges Note the ‘S’ shaped joint line between the talonavicular joint and the calcaneocuboid joint – important later • The base of the 2nd metatarsal sits in a mortice between the 1st and 3rd metatarsals and the cuneiforms – this can cause problems if the 2nd toe is longer than the first leading to stress #’s of the base of the metatarsal – March # Lateral view of the foot • Lateral arch of the foot consists of the calcaneus, cuboid and 5th metatarsal • The shape of the bones, ligaments and tendons, particularly peroneus longus, give support Ligaments of the lateral aspect of the foot • Dorsal ligaments between bones of the midfoot and the metatarsals • Y shaped bifurcate ligament – calcaneocuboid and calcaneonavicular • Long plantar ligament – supporting the longitudinal arches of the foot • Note peroneus brevis tendon inserting onto the base of the 5th metatarsal Medial view of the foot • The medial arch of the foot is comprised of the calcaneus, navicular, medial cuneiform, and 1st metatarsal • The bony arch is maintained partly by the shape of the bones • The navicular is considered to be the keystone of the arch • The arch is also supported by the tendons of tibialis posterior and flexor hallucis longus Ligaments of the medial aspect of the foot • Note the deltoid ligament of the ankle • Spring ligament – from the sustentaculum tali – a bony protuberance on the calcaneus to the navicular • This ligament is crucial in supporting the head of the talus as it articulates with the navicular rd 3 arch of the foot Ligaments of the forefoot • Metatarsophalangeal joints (MTP) – and interphalangeal joints have collateral ligaments • The heads of the metatarsals are held together by the deep transverse metatarsal ligament and by muscles (Cf later) Roman arch • Bony structure of the arches of the foot likened to a Roman arch Any questions Layers of muscles in the sole of the foot Plantar aponeurosis • Plantar aponeurosis – made of dense fascia consisting of white fibres. It has great strength • It starts from the calcaneus and spans the sole of the foot inserting into the proximal phalanx of each toe • When the toes are extended the longitudinal arch of the foot is raised through the windlass effect as the fascia is tensioned and pulls the calcaneus closer to the toes • Intrinsic muscles • Extend from the calcaneus to the toes • Assist in maintaining the concavity of the foot and flexing the toes • The tendons of flexor digitorum brevis insert into the intermediate phalanx of the 2nd to 5th toes • Abductor hallucis – originates from the calcaneus and inserts into the medial side of the base of the proximal phalanx of the big toe • The muscle is activated when spreading the toes • Abductor digiti minimi – from the calcaneus to the outside of the base of the proximal phalanx of the 5th toe • Active when spreading the toes nd 2 Layer of intrinsic muscles • Lumbricals – 4 small muscles accessory to the tendons of flexor digitorum longus • They arise from the tendons of flexor digitorum longus • The tendons pass to the medial side of the 4 lesser toes and attach to the dorsal expansion (Cf later) • These muscles lift the heads of the metatarsals along the transverse arch when they contract rd 3 layer of muscle • Flexor hallucis brevis – originates from a Y shaped tendon from the cuboid and the lateral cuneiform • The muscle divides into 2 bellies which insert onto each side of the base of the proximal phalanx of the great toe • There are sesamoid bones associated with the insertions which act like pulleys to improve the line of pull • Adductor hallucis – 2 heads oblique and transverse • Oblique arises from the bases of the 2nd to 4th MTs • Transverse from the ligaments of the 3rd to 5th toes • The portions of the muscle are attached to the lateral sesamoid and base of the first phalanx • Contraction of the muscle adducts the big toe • Flexor digiti minimi brevis – arises from the base of the 5th MT. Its tendon inserts into the lateral side of the proximal phalanx of the 5th toe • Contraction of the muscle flexes the little toe • Dorsal and plantar interossei - 4 muscles arising from the metatarsals • 1st inserts on the medial aspect of the proximal phalanx of the second toe • Other 3 on lateral side of the 2nd to 4th toes. They also insert into the dorsal digital expansion (Cf later) • 3 plantar interossei situated below the MT, base of the 3rd – 5th MT • Attached to the medial sides of the bases of the proximal phalanges • The dorsal interossei abduct the toes. The plantar adduct the toes The dorsal aspect of the foot • Extensor digitorum brevis – arises from the superior surface of the calcaneus. It extends medially across the dorsum of the foot ending in 4 tendons • The most medial portion of the muscle is termed the extensor hallucis brevis, inserting into the base of the proximal phalanx of the great toe • The other 3 tendons attach to the lateral side of the tendons of extensor digitorum longus to the 2nd-4th toes • Note the dorsalis pedis artery close to the medial side of EHB – important indicator of peripheral vascular disease if pulse absent • Note the arrangement of the extensor hood associated with each toe Arrangement of the extensor tendon and dorsal expansion • Note the central slip of the extensor tendon to the base of the intermediate phalanges • The insertion of the lumbrical into the dorsal expansion flexes the MTP joint whilst keeping the toe straight – cupping the sole of the foot The course of the tibial nerve • The tibial nerve runs down the centre of the posterior calf under the soleus muscle • At the ankle it passes around the medial malleolus • A branch of the nerve supplies the back of the heel – this can be involved in heel pain Medial and lateral plantar nerves • The tibial nerve divides into medial and lateral plantar nerves under the flexor retinaculum at the medial side of the ankle • In the foot the medial plantar nerve lies between the abductor hallucis and flexor digitorum brevis • It further divides into digital branches which supply the medial 3 ½ toes • The lateral plantar nerve supplies the lateral 1 ½ toes • Nerves are vulnerable where they divide so pain over the instep can sometimes be related to compression or irritation of the nerve • The digital nerves can also be problematic (Cf later) The talocalcaneonavicular joint • The talus acts like a ball bearing between the ankle, the calcaneus below and the navicular in front • The axis of the joint is inclined upwards 40 degrees and 30 degrees medially • The bones and joints forwards of the TCN joint form a single elastic unit which move in response to movement of the talus and calcaneus • The transverse tarsal joint includes the calcaneocuboid joint • Form and ‘S’ shaped joint line • When the foot is weight bearing there is relatively little movement between the naviculo-cuboid unit • As the TCN joint supinates the shape of the joint surfaces and ligaments pulls the transverse tarsal joint into a locked position to form a rigid lever for propulsion The midtarsal joint during pronation Summary of movements at the ankle, subtalar and midfoot • Inward ( medial) rotation of the tibia and talus, everts the heel via the subtalar joint which in turn causes the midfoot to pronate or the medial arch to flatten • In order for the toes to remain in contact with the ground the forefoot – tarsometatarsal joints undergo a compensatory twist into supination Visualising the foot as a twisted sheet of paper • The anterior margin runs along the line of the heads of the metatarsals and is flat to the ground • The posterior margin is vertical representing the calcaneus • The twist imposes arches of the foot • Loading of the foot tends to flatten the arches • Removal of body weight returns the arches The foot and muscle activation during walking Supination and pronation during walking • Heel strike occurs along the lateral border of the heel, therefore the foot is slightly supinated • As the body weight transfers along the lateral border of the foot the heel everts and the foot pronates to become more flexible to accommodate to the surface of the ground • When the foot is flat on the ground the heel is in a neutral position, as is the rest of the foot • As the heel starts to lift at push off it inverts and the midfoot and forefoot supinate to become a rigid lever Running gait • Running requires greater balance, muscle strength and range of movement • Greater balance because a lack of the double support phase and a float phase when neither foot is in contact with the ground • As the speed of running increases so does the float time • Muscles generate greater energy as the head, arms and trunk are raised higher than in normal gait • Muscles and joint structures have to absorb more energy Running in shoes v running barefoot Different types of foot strike during running Pes Planus – flat foot • Congenital flat foot – often raises concerns in children but if the arch returns when non-weight bearing it is not generally a problem • Adult acquired flat foot deformity – related to dysfunction of the tibialis posterior muscle and tendon but can also be related to problems with the spring ligament • Tibialis posterior can be stretched or ruptured. Leaves the primary and secondary everters of the foot, the peroneus brevis and the peroneus longus, relatively unopposed leading to flattening of the medial arch • Obesity and diabetes can predispose the tendon to rupture • Traumatic rupture of the spring ligament or plantar fascia can also lead to medial arch collapse Consequences of a pronated foot • Over pronation of the foot leads to relative leg shortening and a valgus deformity at the knee • This can tilt the pelvis downwards leading to side flexion of the lumbar spine • Lumbar spine side flexion tilts the shoulder girdle down on the unaffected side • The cervical spine side flexes in the opposite direction to the lumbar spine to keep the eyes level Management • Examination of the foot to determine whether the joints of the foot are stiff, range of movement, muscle function within the foot, in the calf, at the knee and hip, palpation of tibialis posterior tendon to ascertain whether this is the issue • Use of an orthotic to correct the heel position and support the medial arch • Strengthening exercises at the hip to correct lower limb alignment • Offloading the tendon, not walking with bare feet, weight loss Plantar fasciitis • Pain under the heel caused by over stretching of the plantar fascia • Caused by an over pronated foot • A high arched foot (Cf later) • Sudden increase in activity • Obesity, pregnancy • Poorly fitting shoes which do not support the foot sufficiently • Can be particularly painful first thing in the morning, or after rest, as the plantar fascia has contracted to its normal position • Management – address the cause, over pronation – use an orthotic, increase muscle function around the hip • Weight loss • Wear a heel cup to cushion the heel, avoid running on hard ground Hallux valgus - Bunion • Can be a genetic tendency • Over pronation of the foot pushing the big toe out of position • Habitually wearing tight fitting, pointed shoes • Inflammation of the bursa, arthritis of the 1st MTP joint • Management – wear shoes with a deeper toe box, Type of splint and spacer • If the problem is mild a splint and spacer between the first and second toes may help to manage the symptoms Surgical procedure to correct hallux valgus • Correction of the position of the metatarsal • In this example osteotomy of the phalanx to achieve good alignment Conditions affecting the toes • Claw toe can affect any toe other than the big toe • Caused by tightness of ligaments and tendons causing the toe to flex • A flexible claw toe can be corrected manually • A rigid claw toe may be associated with arthritis • Hammer toe – Flexed at the PIP joint due to muscle imbalance – poor function of the lumbrical muscles • Can affect any toe other than the big toe • Mallet toe – the DIP joint becomes flexed pushing the toe down into the sole if the shoe • Can occur after toe fracture, stubbing the toe • Management – various products to reduce pressure on the toes • Correct footwear with a deep toe box to reduce rubbing • Intrinsic foot exercises, stretching of tight structures, strengthening extrinsic muscles • Surgical intervention Metatarsalgia • • • • • Pain over the heads of the metatarsals Overuse such as running, jumping Wearing high heeled shoes Being overweight Stiffness of the ankle increasing pressure on the foot Management • Wearing flatter shoes • Use of a metatarsal pad placed behind the heads of the metatarsals Morton’s metatarsalgia • Swelling of the digital nerve as it passes between the heads of the metatarsals • Cause is unknown but thought to be due to wearing tight shoes which compress the nerve • Often described as feeling like a pebble under the base of the toe • Burning pain sometimes numbness • May be relieved by changing footwear • Sometimes requires surgery Pes Cavus • Higher arch than normal, excessive supination of the foot • Associated with metatarsalgia and claw toes or hammer toes • Tightness of the plantar fascia, and tendoachillies • Orthotics may be helpful • Stretching of tight structures Next week • Shoulder girdle and glenohumeral joint • Anatomy with a focus on muscle function • What can go wrong with the shoulder joint • Conditions such as tendinitis, rotator cuff tears • Management of these conditions