Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
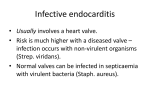
Infective Endocarditis: A Disease Not To Be Missed 1 Infective Endocarditis: a Disease Not To Be Missed Ann Krinks, RGN, BA (Hons), Trainee Advanced Nurse Practitioner (MSc Advanced Practice) Infective endocarditis is a serious disease of the heart; despite this cardiac infections such as endocarditis are viewed as the Cinderella of cardiac diseases often falling into a place of secondary importance with conditions such as Acute Coronary Syndrome (ACS) enjoying most clinical attention. The presentation of infective endocarditis is diverse and the condition can masquerade as many other illnesses causing the patients to present to essentially any clinical specialities. While tremendous successes have been made in the detection and management of ACS the same cannot be said for infective endocarditis. Indeed, for infective endocarditis mortality remains high with more than a third of patients dying within the first year after diagnosis. Despite advances in the diagnostic and therapeutic strategies, the fatality rate of the disease has not decreased in the last 30 years. Coupled with this the fundamental nature of infective endocarditis is changing and new epidemiological genesis is emerging driven primarily by advances in medical therapies. Like with many conditions early identification of patient’s with infective endocarditis is crucial to survival but the complexities of the pathophysiology of the disease coupled with a lack of awareness of the condition means that the diagnosis is all too often delayed. It is essential then to promote awareness of infective endocarditis in order that clinicians can recognise signs and symptoms and know how to respond. 2 Epidemiology Infective endocarditis is a deadly disease with a high mortality rate; over 30% of patients will die within the first year of diagnosis (Thuny et al. 2012). Despite the evolution in antibiotic therapy and sepsis prevention, the incidence of infective endocarditis has not declined in the last 30 years (European Society Cardiology Guidelines 2009). Infective endocarditis is a microbial infection of the endothelial surface of the heart and heart valves with serious even fatal consequences. It occurs when bacteria enter the bloodstream and attach to a damaged portion of the endocardium, the inner lining of the heart or heart valves where they multiply and form vegetation. This vegetation can break off and cause emboli to occlude blood vessels within the body. If the vegetation breaks off from the right side of the heart emboli can travel to the pulmonary circulation and cause Pulmonary Embolism and lung abscess formation. If the vegetation breaks away from the left side of the heart, the emboli can travel to the brain causing stroke, to the kidneys, spleen or coronary arteries resulting in infarction. The causative organisms are mainly bacteria and fungi, of which staphylococcus aureus, staphylococcus epidermis, streptococcus viridians, enterococci and candida albicans are most commonly associated with this infection (Carmela et. al 2012). Historically endocarditis was 100 percent fatal and was associated with heart valve damage from rheumatic heart disease, now uncommon in westernised counties (Prendergast, 2006). The pioneering work of the 19th century physician William Osler, identified that endocarditis was a disease to be suspected in all cases of fever with heart murmur along with this his discovery of the painful erythematous nodes on patient’s hands and feet now known as Oslers nodes made him an eponym of the disease today. (Grinberg & Solimene 2011). 3 Since Olslers first description the fundamental nature of the disease has changed as has its target recipients. The emergence of new constellation of at risk groups include: Those with pre-existing heart defects and degenerative heart disease ( Thanavaro & Nixon 2014) People who inject drugs and risky social behaviour such as body piercing and tattoos (Furat et al. 2014) Recipients of prosthetic valves (Rekik et al. 2010) People with long term indwelling catheters or implanted devices (Baddour et al. 2015) Immunocompromised patients & previous endocarditis The increasing ageing population reflects a large ‘at risk’ group of patients susceptible to endocarditis from degenerative heart disease with more than 50% of all cases of endocarditis seen in over 60’s age group (Tornos et al. 2011). Nosocomial related infective endocarditis is emerging as a growing health concern due to increasing numbers of invasive procedures carried out in 21st century health care, with mortality within this group more than 50% (Fitzsimmons et al. 2010). Intravascular devices such as cardiac pacemakers, internal defibrillators as well as long term indwelling vascular catheters can predispose patients to developing infective endocarditis (Cunha 2011). Microorganisms originating from the skin (staphylococci) and urinary tract (enterococci) being the most common pathogenic cause account of up to 80% of all cases of infective endocarditis ( Moreillon 2010). It has been suggested that patients with infective endocarditis have an in hospital mortality rate as high as 26%, of which could be higher as deaths occurring after discharge have not been recorded. (Fedeli et al. 2011) 4 Almost any type of structural heart disease can predispose to infective endocarditis especially valveular heart disease. Infective endocarditis usually affects damaged valves in the left side of the heart, mitral valve prolapse and degenerative mitral and aortic regurgitation. Prosthetic valve endocarditis can be seen early onset within 60 days of surgery, caused by perioperative valve contamination with staphylococci or late onset due to native valve infection usually due to streptococci (Ashley &Niebauer 2004). Other predisposing conditions include hypertrophic cardiomyopathy, sub aortic stenosis and ventricular aneurysm as well as congenital defects such as coarctation of the aorta, ventricular septal defect and bicuspid aortic valve. Infective endocarditis in intravenous drug users is a fast growing problem due to increasing drug misuse. This group of patients tend not to have any preexisting cardiac disease and affects the right heart valves, their presentation also differs from classic infective endocarditis presenting with pneumonia or septic pulmonary emboli ( Furat et al. 2014) Infective endocarditis has existed for over 450 years; new trends in epidemiology related to changes in social behaviour have made it an emerging problem. A number of factors would account for the change in epidemiological characteristics of infective endocarditis, alongside this with increasing life expectancy and medical advances, the incidence of degenerative heart disease and implanted devices is increasing and as such, it is likely that there will be a rise in the incidence of infective endocarditis in the future. In the postantibiotic era, that now challenges health care providers, many infections are now caused by antibiotic resistant bacteria, which make the management of infective endocarditis even more challenging (Beynon et.al 2006). 5 Presentation Considered a ‘disease in disguise’ infective endocarditis can manifest with varied clinical presentations ranging from non-specific viral symptoms to catastrophic events such as embolic stoke and myocardial Infarction. Many patients may initially experience only general malaise, low grade fever and viral illness type symptoms making diagnosis difficult, some 25% of patients take over a month to be admitted to hospital after onset of their initial symptoms (Connaughton & Rivett 2010). A variety of dermatological signs may be seen, as a result of small emboli travelling to peripheral vessels, however this can be a late sign indicating that the disease has become established (Figure 1). Valve destruction from infective endocarditis will cause murmurs to develop and subsequently may lead to reduced cardiac output and heart failure, heart failure is the most common complication of infective endocarditis. Retinal haemorrhages may be seen on fundoscopy and petechial rashes on the body , inside eye lids and on oral mucosa may be seen as the result of travelled emboli. Anaemia and clinical signs of infection including raised inflammatory markers are common pathology findings. Patients can present to a variety of specialities who are likely to consider their own speciality diagnosis first. Infective endocarditis can present with explainable symptoms which fit with speciality diagnosis such as stroke, abscess formation or renal failure, which may however be a symptom of infective endocarditis and result in an incorrect diagnosis, common examples being malignancy, tuberculosis or other chronic disease. It has been suggested that the most important tool for recognising infective endocarditis is “suspicion”. Initial thorough clinical examination of patients is essential; a heart murmur with fever should alert suspicion to the presence of 6 infective endocarditis, 48% of patients have been found to initially present with a new heart murmur and 20% with a worsening known heart murmur. (Hoen & Duval 2013). The diagnosis of endocarditis is based on blood culture and echocardiographic findings. However, recognition of high risk patients combined with thorough clinical examination is paramount as microbiological findings and imaging studies are not always initially available at the onset of care. Figure.1 Dermatological signs of infective endocarditis Nail fold infarcts from systemic emboli Splinter haemorrhage – thin linear line haemorrhage under the nail bed Oslers nodes- small tender red to purple nodules on the pulp of distal digits of fingers and toes Janeway leisons-small painless macular lesions on palms and soles of feet 7 Defining and Exploring the Problem Significant advances in diagnostics and treatment for Coronary Heart disease within the last decade has resulted in improved survival rates and reduction in morbidity. Research and medical advances within cardiology have mainly focused around Acute Coronary Syndrome (ACS) with advances in early revascularisation strategies and secondary prevention given precedence (Bhatnager et al. 2015). Unfortunately, the tremendous advances made in ACS management have not mirrored cardiac infection, as its fatality rate has not decreased. The incidence of infective endocarditis is difficult to determine due to the variation in succession of the disease. The global burden of the disease is largely unknown and unlike other infectious diseases does not require mandatory reporting to public health agencies, as such a true picture of its epidemiology is not evident (Baddour et al.2015). Analytical data is often based on definitive cases of infective endocarditis therefore reflecting in a misleading relatively low incidence (Fowler et al.2004). However evidence suggests that if deaths from embolic complications of the disease where reported as infective endocarditis as the initial diagnosis, the mortality rate would be considerably higher (Durante-Mangoni & Utili 2014). Indeed, neurological and cardiac symptoms may precede a diagnosis of infective endocarditis and documented as such before the possibility of cardiac infection is considered. Studies have shown an increasing incidence of infective endocarditis over the last decade despite a substantial decrease in the prevalence of rheumatic heart disease as a predisposing factor (Sayan & Carter 2013). This calls to question that infective endocarditis is under diagnosed and is often masked by other conditions. 8 Several factors would suggest reasons for this under diagnosis. Studies have shown that Infective endocarditis is difficult to interpret and is often preceded by other diagnosis. Cerebral complications are the most severe extra cardiac complications of infective endocarditis, with up to 42% of patients experiencing cerebral emboli (Epaulard et al. 2009). Ischemic and haemorrhagic stroke precede the diagnosis of infective endocarditis in 60% of patients (Hoen et al. 2013). In contrast, however evidence from a USA study into the readmission for infective endocarditis after stroke was found to be negligible disbanding the above evidence, however this study was based on patients without clinical evidence of Infective endocarditis (Chu et al. 2015). Clinicians must consider infective endocarditis as a possible underlying diagnosis when confronted with a patient with stroke, perform echocardiography, and blood culture even if fever is lacking as it has been established that the risk of stroke falls rapidly after the initiation of effective antimicrobial therapy (Derex et al. 2009). Similarly, infective endocarditis can result in coronary artery emboli and present as acute myocardial infarction and conduction disorders mainly AV blocks, secondary due to atrial septal abscess formation (Brown et al .2015). Cardiac complications are commonplace in patients with infective endocarditis of which heart failure is recognised as the most frequent cause of death (Paterick et al. 2007). According to figures from the National Heart Failure Audit (2013), around 44,000 patients are admitted to hospital per year with heart failure. Considering these facts, it is questionable that a considerable amount of these patients may have an underlying infective endocarditis as their primary diagnosis. The initial cause of these findings may be overlooked especially given the time constraints of interventions such as thrombolysis in acute stroke and angioplasty during acute Myocardial Infarction (MI). Clinicians need to be aware of alternative causes of acute (MI) other than atherosclerotic 9 plaque rupture, especially in the absence of coronary heart disease risk factors. The suspicion of acute MI secondary to septic vegetation embolism must be considered in patients with prosthetic valves, as current strategies for treatment of acute MI such as percutaneous intervention or thrombolysis is highly dangerous in this instance (Luther et al. 2011). Furthermore other less obvious presentations have been reported with infective endocarditis as the primary cause ; Major vessel emboli due to infective endocarditis can present with lower limb and back pain and misdiagnosis can occur in this setting (Chung et al. 2014). Infective endocarditis often presents initially with pneumonia or septic pulmonary emboli in intravenous drug users (Furat et al. 2014). Although reported as a rare presentation retinal artery emboli manifested by sudden complete vision loss can arise from dislodged emboli secondary to infective endocarditis (Ziakas et al. (2014). It can be established then that infective endocarditis can exhibit as a diverse presentation of disease with live threatening outcomes. Lack of Infectious Endocarditis Ownership The established clinical presentation of patients with endocarditis is highly variable with multiple manifestations, resulting in delayed or missed diagnosis. Quick identification of patients at highest risk of death may offer the opportunity to change the course of the disease and improve prognosis. However, given the pressures of today’s NHS especially within emergency care, much of the emphasis on treating the patients presenting condition takes precedence over establishing the underlying cause. This calls into question which speciality and which physician should care for patients with infective endocarditis? Given the varied presentation of the disease, patients are 10 generally treated by an array of medical professionals with different experience in identifying and treating the condition. Emergency medical professionals within A&E are at the frontline of patient care; it is here that the initial ‘suspicion’ of infective endocarditis and the recognition of ‘at risk’ patients should begin. The initial diagnosis of infective endocarditis may not be at the forefront of the differential diagnosis for the junior clinician in A&E. However emergency physicians have an important role to play in the process of early recognition and to provide education to patients who are at a high risk of developing infective endocarditis, therefore strategies to improve management of patients with infective endocarditis are needed. A recent European study that looked at the management strategies for patients with endocarditis demonstrated a significant reduction in mortality when patients are managed by an established multidisciplinary team involving cardiologist, a specialist in infectious diseases, a microbiologist and a cardiac surgeon (Chirillo et al. 2013). However, evidence from the hospitalist model of care in the USA in which patients are under the care of the generalist physician from admission to discharge has been associated with improved patient outcomes (Meitzer et al. 2002). Patients with acute medical problems are generally admitted to medical assessment units via A&E and are under the care of the acute physician until triaged to a medical speciality, this model may not benefit certain subgroups of patients particularly those patients whose illness fails to align with a medical speciality (Fielding et al. 2013) The European Society of Cardiology guidelines for the management of infective endocarditis (2015) states that the disease needs a collaborative approach from the ‘Endocarditis Team’. It suggests that no single practitioner will solely be able to manage and treat these patients as infective endocarditis is not a single disease and that a multidisciplinary approach involving expertise from a 11 variety of specialists is paramount to positive patient outcome. This multidisciplinary approach is seen as best practice and has been shown to reduce one-year mortality by over 50%, however it is not commonplace for infective endocarditis patients (Chambers et al. 2014). The presence of the endocarditis team may be evident in large tertiary centre hospitals with cardiac surgeons to hand however it would appear that this collaborate approach to patient care is lacking in many smaller district general hospitals. In such cases, the general physician or cardiologist may care for the infective endocarditis patient. It is recommended that patients should be nursed in a specialist area by staff with competences required to recognise deteriorating valve function and other complications, ideally a Coronary care unit. However, advances in treatments for acute ST elevation myocardial Infarction (STEMI) such as primary angioplasty has led to a shift in role of the coronary care unit. With the majority of acute STEMI patients being treated at primary PCI centres the demographics of the district general coronary care unit has changed, from that of acute care setting to more generic general medical unit comprising of more elderly patients with multiple co-morbidities (Walker et al. 2012). Critical care trained cardiac nurses are now frequently caring for lower acuity patients resulting in deskilling and job dissatisfaction of an experienced workfare as well as compromising patient care and safety (Driscoll et al.2013). Chambers et al .( 2014) identified difficulties and impracticalities of setting up infective endocarditis teams in small hospitals and recommends that there are strong links and established means of communication with the endocarditis teams at specialist cardiothoracic centres. In summery it is evident that patients with infective endocarditis need care from multiple specialities but this can be difficult to implement in small district hospitals adding to poorer outcomes for this patient group. 12 Lack of Awareness The concept that infective endocarditis is an uncommon disease is one that is replicated in much of the past literature, this could be likened to severe sepsis which up until 1991 had no real definition and wasn’t recognised . It was not until recognition of Systemic inflammatory response syndrome (SIRS) that awareness campaign groups such as the Surviving Sepsis Campaign and Global Sepsis Alliance set out to raise awareness and provide guidance in recognition and management of severe sepsis (McClelland 2014). Currently throughout the UK, the Survive Sepsis Organisation has produced Sepsis Campaign guidelines for implementation within NHS Trusts focusing on the aggressive management of all patients with sepsis in order to ensure they receive optimal care. The misconception that infective endocarditis is a disease of the past may well deter the clinician into thinking that it is a condition that will not be encountered in daily clinical practice. The clinical presentation of patients with endocarditis is highly variable, often missed or not clinically suspected until diagnosed at post-mortem; this is evident from post mortem studies, which showed 38% of cases not diagnosed unit autopsy (Fowler et al. 2004). Although taught to all medical students as part of their curriculum, studies have shown a lack of knowledge and need for improved education about infective endocarditis. A recent study of 136 medical and dental students identified that only 25% had an acceptable levels of knowledge when questioned about the causative bacteria and underlining cardiac conditions that pre dispose patients to endocarditis, despite passing a theoretical course about endocarditis within a 2 years window ( Zarei et al 2008). A further recent study in Saudi Arabia replicated similar findings, which highlighted that more education in this field is required (Fawzan et al. 2014) 13 A significant problem in diagnosing infective endocarditis is that diagnosis is often made too late as initial symptoms such as fever and malaise can be mistaken for viral illness especially when patients present to their GP. The significance of this has been questioned in the media (Daily Mail 19 March 2014) reported that of a 42 year old man who died of infective endocarditis after first visiting his GP with symptoms of night sweats and lethargy, despite having a pre-existing congenital heart condition he was diagnosed and treated for a chest infection. After two courses of antibiotics and worsening symptoms and referral to a hospital consultant blood cultures failed to diagnose endocarditis (presumed false negative results), due to delays in echocardiogram the patient suffered a cardiac arrest and subsequently died. Many patients at risk form endocarditis such as those with congenital heart defects, prosthetic and degenerative valve disease are unaware of the serious implications of the disease and the preventative measures they should take for avoidance (Stucki et al. 2003). Patients should be aware not to take antibiotics for fever of unclear origin; further more patients in high-risk groups should inform their GP and insist that blood cultures are taken before being prescribed antibiotics. The need for good dental hygiene and prophylactic antibiotic therapy in certain dental procedures is imperative to avoid infection (Stucki et al. 2003). Risk-taking behaviours such as tattoos and body piercings have become common place in today’s society and evidence now suggests an associated risk of developing infective endocarditis in high risk groups i.e people with valve problems or congenital heart defects (Junior et al. 2014). Indeed high risk patients need to be aware of the clinical signs and symptoms of infective endocarditis and the need to seek early medical help. The need for patient education is addressed in the National Institute for Health and Clinical Excellence (NICE) 2008 guideline on the prophylaxis against infective 14 endocarditis in adults and children undergoing interventional procedures . The guideline recommends that health care professionals teach patients about the symptoms of infective endocarditis and the risks of non-medical invasive procedures such as body piercing and tattooing. The established key points can therefore be summarised; Understanding the predisposing factors that make a patient susceptible to infective endocarditis is critical to early recognition, diagnosis and aggressive treatment. Clinicians should be particularly attentive to possible diagnosis of endocarditis in patients with valve disease who present with fever, clinical deterioration and embolic events. Missed diagnosis is common due to lack of awareness of infective endocarditis. Bias exists against diagnosis of infective endocarditis, as it is perceived to be an uncommon disease. Neurological, cardiac or vascular diagnosis may precede infective endocarditis diagnosis. Management Early recognition and investigation is crucial in identifying infective endocarditis. Blood cultures should be taken on initial presentation and ideally before starting antibiotics, to prevent false negative results. Early echocardiogram is the test of choice although transthoracic echo can have inadequate views in up to 20% of patients and has a sensitivity of 60%. Therefore transoesophageal echo is seen as the gold standard test of choice especially for detecting smaller emboli <5mm, and has a sensitivity of over 15 90%. Serial imaging may be required in patients with initial normal study in whom diagnostic suspicion persists. Definitive diagnosis of endocarditis is based on the modified Duke criteria which combine the clinical, echocardiographic and microbiological findings of a suspected patient (Li et.al 2000). Although this tool provides high specificity and moderate sensitivity for the diagnosis of infective endocarditis clinical judgment is essential at the outset of care . Treatment of infective endocarditis includes supporting cardiac function, preventing complications and eradication of infection with lengthy intravenous antibiotics, up to six weeks duration. Despite antibiotic treatment up to half of patients with infective endocarditis will require surgery to repair or replace the valve. Prevention and early diagnosis therefore are the key to reducing morbidity and mortality from this disease. Vigilance is paramount, it can be said that the most important tool for recognising infective endocarditis is “suspicion”. Conclusion It has been established that infective endocarditis is a serious condition with often-fatal consequences if not recognised and treated early .Despite rapid development of advanced diagnostic methods, evolution of antimicrobial therapy and sepsis prevention infective endocarditis continues to create significant morbidity and mortality within today’s health care environment. The incidence of the disease has remained almost unchanged over the past few decades despite the substantial decline in rheumatic fever in the developed world. Infective endocarditis remains an illness that is difficult to diagnose and treat therefore poses a challenge to clinicians. Medical advances in coronary heart disease made over the last decade have resulted in improved survival rates for patients with acute coronary syndrome; 16 unfortunately, this has not translated into the gains for infective endocarditis, which appear to have taken a back seat as its fatality has not decreased . The expansion of the elderly population has given rise to an escalation in degenerative heart disease, now considered a major predisposing risk factor for infective endocarditis. An increase in intra cardiac devices, prosthetic valve replacement, nosocomial infections along with antibiotic resistance have been identified as key risk factors. It is likely that there will be a rise in the incidence of the disease in the future as new constellation of at risk groups are identified such as intravenous drug users and those with body piercings and tattoos. The clinical manifestations of infective endocarditis are so varied that they may be encountered in any of the medical specialities. The diverse nature and evolving epidemiological profile ensures it remains a diagnostic challenge to clinicians and subsequently often goes undiagnosed. Many cases of infective endocarditis are missed completely, patients may present with embolic events because of disease progression which is treated as the primary diagnosis. Lack of awareness of the disease exists as it is misconceived to be an uncommon entity in todays healthcare. Rapid identification of patients at risk of developing endocarditis may offer the opportunity to change the course of the disease and improve prognosis. Vigilance is the key to successful recognition of this ‘Cinderella’ of diseases. The recognition of infective endocarditis is everyone’s concern and building ownership is a top priority. It is inconceivable that in the 21st century patients are still dying from a treatable disease that was prominent in our grandparent’s era. It is time to unmask the camouflage of infective endocarditis, banish its enigma and raise its profile in order to save lives in the future. 17 REFERENCES Ashley,EA. Neibauer,J. (2004). Cardiology Explained. London. Remedica. Baddour,L. Freeman.K, Suri,R. Wilson,W. (2015). Cardiovascular Infections. In: Mann,D. Zipes.D, Libby,P, Bonow.R, Braunwald.E. ed. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine, 10th edition. USA: Saunders, pp1524-1447 Bhatnager.P, Wickramasinghe.K, Williams.J, Rayner.M, Townsend.N (2015) The epidemiology of cardiovascular disease in the UK 2014. Heart 101(15),pp1182-1189 Beynon,R. Bahl,V. Prendergast,B (2006). Infective Endocarditis. British medical Journal. 333(7563): 334-339. Brown,R. Chiaco,J. Dillon,J. Catherwood,E. Ornvold,K (2015). Infective Endocarditis presenting as Complete Heart Block with an Unexpected Finding of a Cardiac abscess and purulent pericarditis. Journal of Medcine Research. Vol;7 (11): 890-895. Carmela,T. Rodriguez,R. (2012) Endocarditis and Other Infections. Pathology of Infectious Diseases Procop, G.& Pritt,B. Saunders USA Chambers, J. B., Sandoe, J., Ray, S., Prendergast, B., Arden, C., Wilson, J., Campbell, B., Gohlke-Baerwolf, C., Mestres, C. A., Rosenhek, R., Pibarot, P. and Otto, C. M. (2014) ‘Response to comment on: The infective endocarditis team: Recommendations from an international working group by San Roman et al’, Heart, 101(2), pp. 162–162. Chirillo, F., Scotton, P., Rocco, F., Rigoli, R., Borsatto, F., Pedrocco, A., De Leo, A., Minniti, G., Polesel, E. and Olivari, Z. (2013) ‘Impact of a Multidisciplinary management strategy on the outcome of patients with native valve Infective Endocarditis’, The American Journal of Cardiology, 112(8), pp. 1171–1176. Chu,S. merkler,A. cheng,N. Kamel,H (2015). Readmission for infective Endocarditis After Ischemic Stroke or Transient Ischemic Attack. The Neurohospitalist. 5(2) 55-58 Chung- Esaki.H, Rodriguez.R. Alter.H, Cisse.B (2014). Validation of a prediction rule for endocarditis in febrile injection drug users. American Journal of Emergency Medicine.32. pp412-416 18 Connaughton.M, Rivitt.J. (2010) Practice easily missed? Infective endocarditis. British Medical Journal :341:6596 Cunha, B. (2011). Nosocomial methicillin-sensitive Staphyloccal aureus (MRSA) native valve acute bacterial endocarditis (ABE) due to radiofrequency catheter ablation procedure. Heart and Lung. Vol 40 pp563-565 Dayer,M. Jones,S. Predergast,B. Baddour,L. Lockheart,P. Thornhill,M. (2015) Incidence of infective endocarditis in England,2000-13: a secular trend, interrupted time-series analysis. Lancet Vol 385. pp1219-28 Derex,L. Bonnefoy,E. Delahaye (2010). Impact of stroke on therapeutic decision making in infective endocarditis. Journal of neurology 257: pp315-321 Driscoll, A., Currey, J., George, M. and Davidson, P. M. (2013) ‘Changes in health service delivery for cardiac patients: Implications for workforce planning and patient outcomes’, Australian Critical Care, 26(2), pp. 55–57. Durante-Mangoni,E and Utili,R. (2014). Nosocomial endocarditis: still a challenging diagnosis. Internal Emergency Medicine. Vol 9 pp715-716 Ellis,B. Kalvaitis,K. Swain,E. Taliercio,A. Januzzi, J. (2015) Incidence of Infective Endocarditis on the Rise in England. Cardiology Today. 18.1:22 Epaulard, O., Roch, N., Potton, L., Pavese, P., Brion, J.-P. Stahl, J. (2009) ‘Infective endocarditis-related stroke: Diagnostic delay and prognostic factors’, Scandinavian Journal of Infectious Diseases, 41(8), pp. 558–562. European Society of Cardiology Guidelines for the management of infective endocarditis (2015). European Heart Journal. 36, 3075-3123 European Society of Cardiology Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (2009). European heart Journal. 30, 2369-2413. Fawzam, A. Al Saeed,A. Abd Elmoniem,A (2014) Assesment of Awareness regarding prevention of Infective Endocarditis among Graduating Medical and dental Students at Qassim University,KSA. Global jiurnal of Medical research. Vol14No 2 19 Fedeli,U. Schievano,E. Buonfrate,D. Pellizzer,G. Sploaore,P. (2011) increasing incidence and mortality of infective endocarditis : a population –based study through a recordlinkage system. BMC infectious Diseases 11:48 pp 1-7 Fielding,R. Kause,J. Arnell-Cullen, J. Sandeman,D. (2013) The impact of consultantdelivered multidisciplinary inpatient medical care on patient outcomes. Clinical Medicine p 344-348 Fitzsimmons,A. Bamber,A. Smalley,B (2010). Infective endocarditis: changing aetiology of disease. British Journal of Biomedical Science 67(1) pp35-41 Fowler,V. Scheld,M. Bayer,A.. (2004). Endocarditis and Intravascular Infections. In: Mandell, Bennett & Dolin Principles and Practice of Infectious Diseases. London: Churchill Livingstone. Furat, C., Ilhan, G., Bayar, E., Ozpak, B., Kara, H. and Yilmaz, M. (2014) ‘Isolated tricuspid valve infective endocarditis in young drug abusers’, Therapeutic Advances in Cardiovascular Disease, 8(3), pp. 119–122. Furat,C. IIhaan,G. Bayar,E. Ozpak,B. Kara,H. Yilmaz,M. (2014). Isolated tricuspid valve infective endocarditis in young drug abusers. Therapeutic Advances in Cardiovascular Disease. Vol.8(3) pp119-122. Grinberg,M. Solimene,M (2011). Historical aspects of infective endocarditis. Journal of Brazilian Medical Association 57(2) 223-228 Hoen,B. Duval,X. (2013). Infective Endocarditis. The New England Journal of medicine. 368;15 pp1425-1433. Junior MML, Lima. MM, Granja. F (2014) Bacterial Endocarditis Following Genital Piercing. Journal Pioneer Medical Science. 4 (2): p79-80 Li,S.J. Sexton,D.J. Mick,N. Nettles,R. Fowler,V.G. Ryan,T. Bashore,T. Corey,R.G. (2000). Proposed Modifications to the Duke Criteria for the Diagnosis of Infective Endocarditis. Clinical Infectious Diseases. Vol 30 Issue4, pp633-638 20 Luther, V., Showkathali, R. and Gamma, R. (2011) ‘Chest pain with ST segment elevation in a patient with prosthetic aortic valve infective endocarditis: A case report’, Journal of Medical Case Reports, 5(1), p. 408. McClelland.H, (2014) Early identification and treatment of sepsis. Nursing Times Vol 110. No 4 pp14-17 Meitzer, D. Manning,WG. Morrison ,J. (2002) Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trail of hospitals. Annuals of Internal Medicine 137: p866-867 National heart Failure Audit (2013) British Society for Heart Failure. [on-line] Available at: https://www.bsh.org.uk/nicor/audits/heartfailure. Accessed 21st December 2015 O’Neill, L., Smith, K., Currie, P., Elder, D., Wei, L. and Lang, C. (2013) ‘Nurse-led early triage (NET) study of chest pain patients: A long term evaluation study of a service development aimed at improving the management of patients with non-sT-elevation acute coronary syndromes’, European Journal of Cardiovascular Nursing, 13(3), pp. 253– 260. Paterick, T. E., Nishimura, R. A. and Steckelberg, J. M. (2007) ‘Complexity and subtlety of Infective Endocarditis’, Mayo Clinic Proceedings, 82(5), pp. 615–621. Prendergast,B. (2006). The changing face of infective endocarditis. Heart 92(7): 879-885. Rekik, S., Trabelsi, I., Hentati, M., Jemaa, M. B., Hammami, A. and Kammoun, S. (2010) ‘179 clinical and echocardiographic predictors of mortality in prosthetic valve endocarditis’, Archives of Cardiovascular Diseases Supplements, 2(1), p. 57. Sayan.O, Carter.W.(2013) Endocarditis. In : Adams. A . Emergency Medicine. 2nd edition.USA Saunders. pp530-546 Stucki,C. Mury,R, Osmund,B (2003) Insufficient awareness of endocarditis prophylaxis in patients at risk. Swiss medical Weekly 133: 155-159 Swanton.H. Banerjee.S, (2008) Swanton’s Cardiology: A concise guide to clinical practice. 6th edition.Blackwell Publishing.Malden pp. 419–447. 21 Thanavaro, K. L. and Nixon, J. V. (Ian) (2014) ‘Endocarditis 2014: An update’, Heart & Lung: The Journal of Acute and Critical Care, 43(4), pp. 334–337. Thuny,F. Grisoli,D. Collart,F. Habib,G. Raoult,D. (2012) . Management of infective endocarditis: challenges and perspectives. The Lancet. Vol 379. Pp965-973 Tornos,P. Gonzalaz-Alujas,T. Thuny,F. Habib,G. (2011). Infective Endocarditis : The European Viewpoint. Current Problems in Cardiology. Vol 36: pp175-222 Walker,D. West,N. Ray,S (2012) From coronary care unit to acute cardiac care unit: the evolving role of specialist cardiac care. Heart. V98: p350-352. Welch, E. (2011) ‘Red flags in medical practice’, Clinical Medicine, 11(3), pp. 251–253. Zarei,M. Navabie,N. Chamani,G. (2008) Assessment of awareness of recommendations for prevention of bacterial endocarditis among a group of 136 Iranian dental and medical students.Acta Medica iranica, V.46 no.1 pp51-58 Ziakass,N. Kotsidits,S. Ziakas,A . (20140. Central retinal artery occlusion due to infective endocarditis. International Ophthalmology Vol34 pp315-319. 22 23