Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
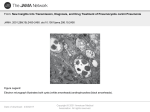
A case study of Pneumocystis Pneumonia 9517 Objectives Definition Epidemiology Pathophysiology Clinical Manifestations Diagnosis Treatments Prognosis Case study What is PCP? Pneumocystis Pneumonia is caused by the fungal organism Pneumocystis carinii which was recently renamed Pneumocystis jiroveci. PCP is found in many environments and does not cause illness in healthy people, however in immunosuppressed patients such as those with HIV or AIDS, PCP is opportunistic and often fatal. Current Opinion in Pulmonary Medicine Emerging Infectious Diseases Epidemiology PCP is thought to be spread by direct contact and has been found in almost all mammalian species. PCP is the most prevalent opportunistic infection in patients infected with the human immunodeficiency virus. It is the leading cause of death in HIV/AIDS patients and up to 80% of AIDS patients contract PCP. Most children are exposed to PCP in the first few years of life and it may contribute to SIDS Although PCP occurs all over the world, it is more of a threat to underdeveloped nations. Journal of Infectious Diseases The New England Journal of Medicine Pathophysiology Somewhat unclear since PCP cannot be cultivated easily. Occurs most frequently when the CD4+ cell count is less than 200 cells/mm3 The trophic form of the organism attacks the alveolar epithelium causing thickening of the alveoli and inflammation. Microscopically, the small predominantly haploid trophic forms are 1-4 µm in diameter while the cysts (up to 8 nuclei) are up to 8 µm in diameter. This decreases the alveolar-capillary membrane permeability leading to significant hypoxia and changes in lung capacities. The New England Journal of Medicine eMedicine Pathophysiology cont. Glycoprotein A was the first molecule identified from Pneumocystis and has an vital role in the attachment of Pneumocystis to host cells. Beta-1,3-glucan is part of the cyst wall providing stability and is responsible for the inflammatory response in the hosts lungs. Enhanced activity of the encoding gene mitogen-activated protein kinase (PCM) suggests trophic forms of Pneumocystis use this pathway in the life cycle of PCP. The New England Journal of Medicine Pathophysiology cont Panel A shows the trophic form adhering to the alveolar epithelium Panel B shows trophic forms attaching to each other which can be seen during infection Panel C shows a cyst The New England Journal of Medicine Clinical Manifestations Symptoms include SOB, fever, and a dry non- productive cough that may occur months before clinical presentation. Tachycardia and tachypnea A significant drop in PaO2 along with bilateral diffuse infiltrates originating in the perihilar regions as seen on the CXR. Seminars in respiratory and critical care medicine Diagnosis The primary definitive diagnosis for PCP is direct visualization through staining techniques Grocott-Gomori methenamine silver is most used. Others are available including Wright-Giemsa, calcoflour white, and the Papanicolaou. Immunoflourescent stains often produce false positives. PCR Increased lactase dehydrogenase (LDH) levels often associated with diagnosis. Seminars in respiratory and critical care medicine Treatments Although a fungus, PCP does not respond to antifungal treatment. There is accumulating evidence of mutations of certain genes in PCP arousing concern for potential resistance to certain medications. Recommended duration of treatment for and HIV/AIDS individual is 21 days and 14 days for all other patients. The New England Journal of Medicine Current Opinion in Pulmonary Medicine Treatments cont. Drugs to treat are TMP-SMX, Primaquine, Clindamycin, Dapsone, Atovaquone, Trimetraxate, and Pentamadine. Anti-inflammatory meds such as Prednisone and Solu-medrol. Oxygen therapy and mechanical ventilation. Current opinion in pulmonary medicine Prognosis If left untreated may cause death. The prognosis depends on the extent of infection and damage to lungs at time of diagnosis. Those with suppressed immune systems take longer to recover. Antibiotic treatment is about 80% effective. Seminars in respiratory and critical care medicine Case Study Objectives Source, reliability, and chief complaint History of present illness Past medical history Home medications Hospital medications Review of systems Social history Family history Physical exam Lab data Echocardiogram and chest x-ray Assessment Mechanical ventilation daily summaries Respiratory treatments Summary of hospital stay The Case Study Source: The patient and the patients chart Reliability: Felt to be mostly accurate Chief complaint: DOE and a dry cough getting progressively worse for 2-3 weeks. History of Present Illness The patient is a 42 year old African American female with AIDS complaining of DOE and worsening SOB over the past two weeks. Her daughter asked her to go to the ER because she looked sick, could not breath easy and kept coughing. Her daughter took her to the ER where she was then admitted to the floor and later the ICU. Past Medical History HIV/AIDS The patient was diagnosed in 1995 after the father of one of her children died. Starts antiretroviral meds, and is non-compliant. CD4 count went from 81 in 2000, to 24 in 2008 demonstrating very advanced AIDS Hepatitis B Diagnosed 1995, non-compliant with all meds Herpes S./Genital (HSV type 2) First diagnosed in mid 2007 Started treatment with Valtrex, but as of January 2008 is no longer taking the meds and has had no more outbreaks. HTN Diagnosed in 2000 with her BP reading 180/118. Tried several different meds, however patient is non-compliant. Chronic Anemia The patient had first started these issues in 2001 following a very heavy menstruation with a Hgb of 4.5, however asymptomatic. From 2001 to 2006 she has received multiple blood transfusions. She is non-compliant with all meds and refuses to go to her doctors appointments. Past Medical History cont. Cervical Malignancy and Menorrhagia The bleeding first started in 2004 when the patient had 6 days of heavy clots and was referred to a specialist whom she refused to see. Diagnosed with squamous cell carcinoma in 2005 with more bleeding; the patient claims to be getting a hysterectomy in two weeks. The patient canceled surgery and has not shown up for three appointments, states she is scared to schedule an appointment despite lengthy discussions on the seriousness of this disease. Finally had a total hysterectomy in 2007, ovaries remain intact. Thyroid Malignancy Diagnosed in 2002 After several surgical cancellations, the patient had a subtotal thyroidectomy in 2004 and continued on unithyroid irregularly. Hypothyroidism Diagnosed in 2005, the patient starts treatment (unithyroid) but takes irregularly. Home Medications Brand Generic Type Dose Use Bactrim Sulfamethoxazole and trimethoprim Sulfonomide and pyrimidine (to help activity of sulfonomide) DS QD (160 mg tromethoprim, and 800 mg sulfa.) To treat and prevent PCP Truvada Tenofovir and Emtricitabine Anti-HIV Nucleoside reverse transcriptase inhibitor 200/300 mg QD To treat HIV and HBV Tenormin Atenolol Beta blocker 100 mg BID To treat high blood pressure Valtrex Valacyclovir Antiviral 1 g QD To treat/prevent herpes Lexiva Fosamprenavir Protease inhibitor 700 mg BID Helps manage HIV when taken with other HIV meds Synthroid Levothyroxin Sodium Hormone replacement 100 mcg QD Thyroid replacement therapy In Hospital Medications Brand Generic Type Dose Use Zithromax Azythromycin Macrolide (inhibits protein synthesis) 500 mg QD To treat broad spectrum bacteria Cleocin Clindamycin Lincosamide (gram + and anaerobic) 600 mg/4 ml Q6H To treat PCP Primiquine phosphate Primaquine Antimalarial 26.3 mg QD To treat PCP and malaria Valtrex Valocyclovir Antiviral 500 mg QD To treat/prevent herpes Synthroid Levothyroxin Sodium Hormone replacement 100 mcg QD Thyroid replacement therapy Tenormin Atenolol Beta blocker 100 mg BID To treat high blood pressure Prinivil Lisinopril ACE inhibitor 20 mg QD To treat high blood pressure Cytovene Ganciclovir Guanine nucleoside analog 400 mg Q12H To treat CMV In Hospital Medications cont. Brand Generic Type Dose Use Haldol Haloperidol Antipsychotic 5 mg IM PRN To treat agitation Versed Midazolam Benzodiazapine 2 mg PRN To treat agitation Fentanyl Fentanyl Narcotic 50 mcg/ml drip To treat pain associated with ventilator Nexium Esomeprazole Protein pump inhibitor 40 mg PO QD To prevent aspiration Phenergran Promethazine Antiemetic 25 mg Q8H To treat nausea Solu-medrol Methylprednisolone Steroid 125 mg QD DCd 8/16 To treat inflammation Lasix Furosemide Loop diuretic 60 mg IV To treat pulmonary effusion Combivent Ipratropium and Albuterol Anticholinergic and Adrenergic agents 4 puffs Q4H To treat bronchospasm Review of Systems General: No fever/chills or night sweats Reproductive: No abnormal bleeding Respiratory: DOE, progressive for 2 weeks with dry non-productive cough Neuromuscular: General weakness and fatigue, no acute joint pain GI: No n/v/d, poor appetite for 2 months NKDA All other systems negative Social History Long history of non-compliance with medications, doctors appointments and surgical procedures frequently canceled. Patient denied any alcohol or illegal drug use. The patient is a non-smoker. The patient has never traveled overseas. No occupational history Family History Mother: Alive, overweight, arthritis, HTN Father: Died from lung cancer, smoker Brothers: The patient has 2 brothers that are alive with HTN Sisters: The patient has 4 sisters that are alive and well. Children: The patient has 3 children that are alive and well Father of children died in 1995 of AIDS The Physical Exam 8/19/08 General: An overweight AAF orally intubated on mechanical ventilation. Vitals: Temp = 37, RR = 24, BP = 124/82, P = 91, SaO2 = 95% on FiO2 of 65%. HEENT: No oral thrush, no oral herpes Chest: Normal to inspection with equal chest rise. Bibasilar decreased BS with few scattered crackles and rhonchi that clears with suctioning. The Physical Exam (cont.) Cardiovascular: No JVD. Abdomen: Soft and nontender with no organomegaly detected. Skin: No significant lesions are noted. Extremities: no peripheral edema Neurological: Verbally arousable with a distressed look, follows commands at times. Lab Data 8/6/08 ER Basic Metabolic Profile Na+ (136-145) K+ (3.5-5.0) Cl- (98-106) Bicarb (22-26) 120 L 3.3 L Complete Blood Count 87 L 26.2 BUN (3-20) 7 WBC (5-10) Hgb (12-16) HCT (37-47) Platelets (150-450) 11.2 H 8.1 L 5.6 L 381 Cr (0.9-1.5) Glucose (70-105) LDH (135-214) 0.6 L 94 332 H 8/13/08 ICU Basic Metabolic Profile Na+ K+ 125 L 4.7 Complete Blood Count Cl- Bicarb BUN Cr 97 19.5 L 11 0.6 L WBC Hgb HCT Platelets 19.8 H 12.2 36 157 Glucose 92 8/18/08 Basic Metabolic Profile Na+ K+ Cl- Bicarb BUN Cr Glucose 137 4.1 92 L 34.6 H 33 H 0.7 L 102 Complete Blood Count WBC Hgb HCT Platelets 19.2 H 9.5 L 28.7 L 183 8/27/08 Basic Metabolic Profile Na+ K+ Cl- Bicarb BUN Cr Glucose 146 5 110 H 25.3 63 H 0.8 146 H Complete Blood Count WBC 14.4 H Hgb 9.2 L HCT 28.5 L Platelets 151 Lab Data Sputum Cultures Collected via mini BAL on 8/14 Silver stain (+) PCP, (-) AFB, (+) CMV EKG and CXR Regular sinus rhythm, no ectopy Chest X-ray August 6th Diffuse interstitial infiltrates, patchy airspace infiltrates in the right lower lobe. (PA and lateral) August 13th Post intubation film confirmed proper tube placement with tip at T3 August 15th Mild cardiomegaly, mild effusions in both lungs, hypo-inflation in both lungs, interstitial reticularnodular changes in perihilar and lower lobes August 23rd No cardiomegaly, no effusions or edema. Improvement in aeration in both lungs as well as decreased infiltrates compared to previous studies. Example CXR Laurence Huang, MD Assessment Pulmonary Assessment Pneumonia likely PCP CAP Malignancies Consider metastatic etiology Tuberculosis Cytomegalovirus-can cause interstitial pneumonia in immunocompromised patients Cardiovascular Assessment Hypertension Mechanical Ventilation Daily Summaries Delivery device ER 8/6/2008 ICU 8/13/2008 ICU 8/13/2008 Vent day 1 ICU 8/14/2008 Vent day 2 PICC line Art-line 10LPM via NRB 15LPM via NRB Unable to saturate with NRB at 15LPM. Transferred to ICU for elective intubation. Avea mechanical ventilator #8.0 ETT at 22cm at lip Avea mechanical ventilator Mode Vt Rate FiO2 PEEP PIP MAP Mode Vent Settings ABG ABG and VS VS pH PCO2 7.56 31 BP HR PaO2 40 RR HCO3- 26 SpO2 ABG 202/104 114 VS pH PCO2 7.35 BP 33 HR 34 PaO2 49 85% HCO3- 19 Temp 36.8o ABG taken on room air Volume A/C 550ml 12 (21 over) 1.0 10 29 18 ABG 193/113 72 RR 30 SpO2 83% Temp 37o On FiO2 1.0 and 15 LPM NRB VS PaO2 7.23 49 69 HCO3- 21 pH PCO2 Volume A/C Rate ↑ 600ml ↑ 14 (8 over) FiO2 PEEP PIP MAP 1.0 10 38 13 Vt ABG BP 157/108 HR 91 RR 33 SpO2 90% Temp 37.1o This ABG was the basis for the vent change on day 2 pH PCO2 PaO2 HCO3- VS 7.34 35 83 19 BP 165/110 HR 88 RR 22 SpO2 96% Temp 37o Taken after the vent change Mechanical Ventilation Daily Summaries ICU 8/16/2008 Vent day 4 ICU 8/19/2008 Vent day 7 ICU 8/21-8/22/2008 Vent day 8 and 9 ICU 8/24-8/26/2008 Vent day 11, 12, and 13 Arousable and following commands, (+) cough reflex Avea mechanical ventilator #8.0 ETT at 22cm at lip Avea mechanical ventilator #8.0 ETT at 22cm at lip Pressure A/C 580ml 14(10 over) 1.0 Mode Volume A/C Vt ↓ 500ml Rate 14(15 over) FiO2 600ml 14(8 over) 1.0 Mode ~Vt Rate FiO2 PEEP ↑ 12 PEEP ↑ 14 PIP MAP 35 16 PIP MAP 37 22 Pressure A/C Arousable and following commands, (+) cough reflex Avea mechanical ventilator #8.0 ETT at 22cm at lip Mode ~Vt Rate FiO2 ICU 8/27/2008 Vent day 14 and 15 ↓ .80 (in increments) PEEP ↓ 12 PIP MAP 24 15 Avea mechanical ventilator #8.0 ETT at 22cm at lip Mode ~Vt Rate Avea mechanical ventilator #8.0 ETT at 22cm at lip Pressure A/C Mode PSV 500ml 12(8 over) ~Vt ~Rate FiO2 500ml 25 .50 ↓ .50 (in increments) FiO2 PEEP PIP MAP 12 30 18 16-8 (in increments) CPAP 12-10-5 (in increments) PS MAP ABG VS ABG VS ABG VS pH 7.42 PCO2 41 BP HR 142/65 pH 7.41 PCO2 46 BP HR 124/82 86 91 pH 7.38 PCO2 44 78 RR 22 PaO2 90 RR 24 PaO2 PaO2 HCO3- 26.4 SpO2 93% Temp 36o HCO3- 29 SpO2 97% Temp 37o Taken after vent change Taken before vent change 95 HCO3- 26 BP HR RR ABG VS pH 7.38 PCO2 45 BP HR 122/81 103 29 PaO2 RR 20 118/89 SpO2 97% Temp 36o Taken after vent changes 105 HCO3- 26 ABG 82 SpO2 99% Temp 36o Taken after vent changes 7 VS pH 7.39 BP 120/88 PCO2 44 HR 75 PaO2 109 RR 25 HCO3- 25 SpO2 99% Temp 36o Taken 30 minutes prior to extubation Respiratory Treatments Date Type Intubation 8/13/08 ET tube size 8mm @ 22 cm at the lip Mechanical Ventilation 8/13/08 Avea mechanical ventilator Bronchodilator 8/6-8/29/08 Combivent Suctioning Indications Patient Data Protection of the airway and impending failure pH 7.35 PaCO2 33 PaO2 49 HCO3 19 Initially put on Volume A/C with an FiO2 of 100% VOPS/Respiratory Failure (impending or acute) pH 7.35 PaCO2 33 PaO2 49 HCO3 19 4 puffs QID Bronchospasm Prophylaxis 8/138/27/09 PRN Secretions ~3 cc thick white mucus Incentive Spirometry 8/278/29/08 10 times an hour, every hour patient is awake To reverse and prevent further atelectasis from being on the vent Atelectasis Oxygen (0n floor) 8/278/29/08 10 LPM Hypoxemia SpO2 >90% Oxymizer Dose Summary of hospital stay ER Floor ICU DNR/Do not trach Floor 8/06/08 8/06 - 8/13/08 8/13 - 8/27/08 8/25/08 8/27 - 8/29/08 Discharged to Kindred 8/29/08 Plan is to send patient home in 1-2 weeks References . D’Avignon LC, Schofield CM & Hospenthal DR (2008). Pneumocystis Pneumonia. Seminars in respiratory and critical care medicine, 29(2), 132-140. Fei M & Huang L (2008). HIV – associated pneumonias. Retrieved September 4, 2008 from http://img.thebody.com/sfaf/2008/winter08_pneumonia2.jpg Kaplan JE, Hanson D, Dworkin MS, Frederick T, Bertolli J, Lindegren ML, et al (2000). Epidemiology of human immunodeficiency virus-associated opportunistic infections in the United States in the era of highly active antiretroviral therapy. Clinical of Infectious Diseases; 30 1:S5–14. Krajicek BJ, Limper AH, & Thomas CF (2008). Advances in the biology, pathogenesis and identification of Pneumocystis pneumonia. Current Opinion in Pulmonary Medicine, 14, 228-234. McLean J (2007). Pneumocystis (carinii) jiroveci Pneumonia. Retrieved August 27, 2008 from http://www.emedicine.com/med/topic1850.htm#section~AuthorsandEditors. Morris A, Wei K, Afshar K, & Huang L (2008). Epidemiology and clinical significance of Pneumocystis colonization. The Journal of Infectious Diseases, 197, 1-17. Morris A, Lundgren J, Masur H, Walzer P, Hanson D, Frederick T et al (2008). Current epidemiology of Pneumocystis pneumonia. Emerging Infectious Diseases, 10(10), 1713-1720. Thomas CF & Limper AH (2004). Pneumocystis Pneumonia. The New England Journal of Medicine, 350, 2487-2498.