Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Bacterial cell structure wikipedia , lookup
Community fingerprinting wikipedia , lookup
Marine microorganism wikipedia , lookup
Molecular mimicry wikipedia , lookup
Triclocarban wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Infection control wikipedia , lookup
Neonatal infection wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Bacterial morphological plasticity wikipedia , lookup
Bacterial taxonomy wikipedia , lookup
Human microbiota wikipedia , lookup
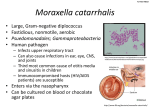
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, BANGALORE KARNATAKA PROFORMA FOR REGISTRATION OF SUBJECT FOR PROJECT. 1. NAME OF THE CANDIDATE SAVITHA RAVEENDRAN ADDRESS POST GRADUATE (M.Sc. M.L.T) DEPARTMENT OF MICRIBIOLOGY, ST.JOHN’S MEDICAL COLLGE AND HOSPITAL, BANGALORE- 34. 2. COURSE OF STUDY 1ST YEAR M.Sc. MLT 3. SUBJECT MICROBIOLOGY 4. DATE OF ADMISSION 3 SEPTEMBER 2012 5. TITLE OF THE TOPIC IDENTIFICATION AND ANTIBIOTIC SUSCEPTIBILITY PATTERN OF Moraxella catarrhalis. 1 6. BRIEF RESUME OF THE INTENDED WORK 6.1 NEED FOR THE STUDY Moraxella catarrhalis is an opportunistic pathogen. It is found as a normal commensal in respiratory tract of human. It is a common cause of bronchitis and bronchopneumonia seen in patients.(1)In infants it appears that seasonal nasopharyngeal colonization, peaking in winter is common. Infections are thought to represent extensions of colonized areas.(2).Studies have shown that organisms from the nasopharynx can spread easily to the middle ear and lungs. Since the late 1970s it has been clear that Moraxella catarrhalis is an important and common human respiratory pathogen. In immune compromised hosts, the bacterium can cause a variety of severe infections including pneumonia, endocarditis,septicemia and meningitis (5). Moraxella catarrhalisis frequently present in the sputum of adults with chronic obstructive pulmonary disease (COPD). COPD is the fourth most common cause of death in the world and is associated with enormous morbidity and health care costs (3).Adults with COPD develop variable humoral immune responses to Moraxella catarrhalis after exacerbations, including new serum IgG and new mucosal IgA to epitopes on the bacterial surface (4).Doren (1986) suggested that it is the third ranking pathogen in this particular patient population following streptococcal pneumoniae and Haemophilus influenzae. Moraxella catarrhali has also been reported to cause keratitis, suppurative arthritis, bacteremia, meningitis, endocarditis, urogenital infection, otitis media and sinusitis. Additionally it has been established as a nosocomial pathogen(2). 2 Moraxella catarrhalis is resistant to Penicillin due to the production of beta lactamase(1). The production of Beta -lactamase by Moraxella catarrhalis, was first reported in1977. Today, more than 90% of the strains isolated worldwide produce beta-lactamase.In Moraxella catarrhalis two types of Beta-lactamases can be found that are phenotypically identical: the BRO-1 and BRO-2 types. The enzymes are encoded by chromosomal genes, and these genes can be relatively easily transferred from cell to cell by conjugation. Beta-Lactamase from Moraxella catarrhalis not only protects the bacteria producing the enzyme but also is thought to inactivate penicillin therapy of concomitant infections by serious airway pathogens such as S. pneumonia and/or nontypeable H. influenzae. This phenomenon is referred to as the indirect pathogenicity of Moraxella catarrhalis. Indeed, in such circumstances, treatment failures have been reported (5). Therefore, taking in to consideration that Moraxella catarrhalis has evolved to become a beta lactamase producer it is important to isolate Moraxella catarrhalis and study their antibiotic susceptibility pattern for the management and prevention of the infections. 3 6.2 REVIEW OF LITERATURE History Moraxella catarrhalis has an interesting and checkered taxonomic history. (6) Initially Seifert (1882) described a case of purulent tracheobronchitis and penned the putative agent as Micrococcus catarrhalis defined as a species as Micrococcus (2).After having initially been named Micrococcus catarrhalis, the organism's name was subsequently changed to Neisseria catarrhalis, because of its similarities in phenotype and ecological niche to commensal Neisseria species. The bacterium was transferred to a new genus, Branhamella, in 1970, because of limited DNA homology with Neisseria species. Branhamella catarrhalis was subsequently placed in the genus Moraxella on the basis of biochemical and genetic relatedness, and Moraxella catarrhalis is now the widely accepted name. (6)Ghon and Pfeiffer (1902) recognized the species as a pathogen. Thereafter nvestigators in both Europe and the USA (Benzancon1905, Jordan 1908, Hissand Zinsser 1910) confirmed its pathogenic potential. In1921 Gordon attempted to define a relationship between the organism and common cold. Failing to find any association he submitted that Moraxella catarrhalis should be considered as a Commensal. Berger(1963) and Knapp etal(1984) realized that part of the problem in defining the pathogenic nature of Moraxella catarrhalis was the organisms frequent misidentification withthe respiratory commensal Neisseria cinerea(2).However, the bacterium was described as an “organism whose pathogenic propensities are known to be slight or non-existent” and was thus ignored for decades. Point prevalence studies indicate that Moraxella catarrhalis colonizes the respiratory tract of 5 to 32% of adults with COPD at any one time. (3) 4 More recently, the widespread use of pneumococcal conjugate vaccines has altered nasopharyngeal colonization patterns and caused an increased prevalence of colonization and infection by Moraxella catarrhalis. More than 90% of Moraxella catarrhalis produce a β-lactamase and are, thus, resistant to ampicillin. Two types of β-lactamases have been identified, BRO-1 and BRO-2. After the rapid acquisition of β-lactamase in the 1970s and 1980s, the antimicrobial susceptibility of Moraxella catarrhalis has remained relatively stable in surveys of worldwide collections of strains .Sensitive methods, such as polymerase chain reaction, to detect Moraxella catarrhalis and other bacterial pathogens in respiratory secretions are in development. The application of such sensitive assays is likely to contribute important new observations about the epidemiology and disease patternsof Moraxella catarrhalis, but they are not yet commercially available. (6) Taxonomy and Description of the Genus The Genus Moraxella is classified in family Moraxellaceae. Species belonging to Genus Moraxella are Gram negative,non-motile,coccobacilli (exception Moraxella catarrhalis are diplococci) with occasional formation of short chains. Cellular pleomorphisam is typical as the culture ages or with growth at increased temperature. All species have fimbriae and with exception of Moraxella bovisare encapsulated. They are asaccharolytic and negative for urease,indole and hydrogensulfide. Several species are weakly hemolytic on blood agar. The most important species is Moraxella catarrhalis. The other species associated are Moraxella nonliquefaciens- isolated from nose, throat, mouth and eye. Moraxella lacunate - isolated from mucous membrane of humans and animals Moraxella osloensis– common resident of human genital tract and other mucous membrane. 5 MINOR SPECIES – Moraxella atlantae, Moraxella lincolinii Animal associated Species Moraxella caviae–isolated from throat of guinea pig Moraxella bovis – bovine keratoconjuctivitis Moraxella ovis– from sheep Moraxella canis– from Dogs Apart from Moraxella catarrhalis other Moraxella’s have little pathogenic potential (2) Epidemiology and Transmission Moraxella catarrhalis is an exclusively human pathogen with an ecological niche in the human respiratory tract. The prevalenceof colonization of the upper respiratory tract is highly dependent on age. Whereas the rate of colonization among adults is low (1%-5%), nasopharyngeal colonization is quite common through infancy. A substantial variation in rates of colonization is observed in different geographic regions. (6) Higher colonization rate have also seen in preschool children with asthma than in healthy children. (7)A change in patterns of nasopharyngeal colonization is occurring in countries where pneumococcal conjugate vaccines are used widely. Colonization by vaccine serotypes of pneumococcus is decreasing, and colonization by the nonvaccine pneumococcal serotypes Hemophilus influenza andMoraxella catarrhalis is increasing, resulting in a shift in the pathogens that cause otitis media in children who had received the vaccine, compared with the prevalence among episodes that occurred before introduction of the pneumococcal conjugate vaccine. Pneumococcal vaccination does not affect the genetic diversity of nasopharyngeal isolates of Moraxella catarrhalis, suggesting that the increase in prevalence of colonization will translate to increased rates of otitis media. Similar shifts are being observed among children and adults with sinusitis (6). 6 Serological studies have indicated that the children with otitis media due toMoraxella catarrhalis produce antibodies against a variety of protein antigen of Moraxella catarrhalis.(7) Biofilms of Moraxella catarrhalis are present in the middle ears of children with otitis media and may account, in part, for recurrent and chronic otitis media. However, the role of biofilms in the pathogenesis of otitis media is not yet fully elucidated(6).Moraxella catarrhalis behave as a primary or as a secondary pathogen superimposed on an antecedent viral infection. (e.g. Respiratory syncytial virus).Lower respiratory tract infection due to Moraxella catarrhalis in adults occur predominantly in elder and immunocompromised patients particularly with COPD, bronchiectasis, congestive heart failure and predisposition of aspiration. Immunologic abnormalities because of underlying disease (e.g. diabetes,alcoholism, HIV,transplantation) are also important contributing factor. Nosocomially acquired pneumonia due toMoraxella catarrhalis occur in hospital respiratory units and paediatric intensive care unit. (7) Virulence Factors Hellio etal (1988) demonstrated the presence of a polysaccharide capsule. Antigenic characters has determined that the antigenic nature of outer membrane proteins is conserved among various strains.(7) Resistance to β-lactam antibiotics, mediated by either the BRO-1 or BRO-2 β-lactamase, is a characteristic acquired by the vast majority of strains within the past 20 years . The ability of Moraxella catarrhalis to resist complement – mediated lysis is considered to be an important virulence factor of this organism. (8) 7 Lipoologosaccharide – Studies using monoclonal antibodies demonstrate its structure Fimbriae – Functionas adhesins Hemagglutinins-Believed to contribute to adherence Outer membrane proteins UspA protein UspA 1 – Used as adhesins UspA 2 –Binds to complement system,mucosal adherence,resistance to non-immune sera C D Protein – Specifically binding tonasal and middle ear mucins LpbA and LpbB– lactoferrinbinding protein TbpA and TbpB– Transferrin binding protein CopB protein – Function in iron acquisition in growth. E- protein – It may assist in transport of fatty acid to cells.(7) Laboratory Diagnosis Specimens Clinical samples include sputum, blood, middle ear effusion, tracheal aspirate or BAL. Direct examination Grams stain Moraxella catarrhalis is a gram – negative diplococcus with flattened abutting sides. The sample should be evaluated by microscopy prior to culture to make sure that the Gram negative diplococcic are associated with inflammatory cells and there is adequate single morphotype bacteria present. 8 Culture methods Moraxella catarrhalis are non-fastidious organism produce 1-3 mm whitish grey colonies on blood agar and chocolate agar within 24 hour incubation. Optimum temperature for growth is 35 – 370C(7).Moraxella catarrhalis colonies can be solid along the agar surface without disruption this is termed the “hockey puck sign.” In addition, after 48 h of growth Moraxella catarrhalis colonies tend to be larger and take on a pink color.(6) A selective media containing acetazolamide and antibiotics has been described.(7) Biochemical Reactions Catalase positive Oxidase positive Asaccharolytic Indolenegative H2S negative Nitrate positive DNAse positive Identification based on Butyrate esterase (tributyrin test) The rapid identification of Moraxella catarrhalis is important. The tributyrin spot test will differentiate Moraxella catarrhalis from Neisseria species. The enzyme butyrate esterase produced by Moraxella catarrhalis hydrolyses the tributyrin substrate in buffered salt medium. The reaction yields butyric acid which lowers the pH of the medium resulting in a yellow colour change. This test can be tested using commercially available kits. 9 Complement resistance Moraxella catarrhalis strains can be tested for their sensitivity to serum complement – mediated lysis in a microtiter bactericidal assay,that used 50% pooled human serum. Strains were subdivided into 3 categories: resistant (R; >50% survival of the bacteria during a 3-h incubation in 50% pooled human serum), sensitive (S ;< 3% survival of the bacteria after incubation for 1 h in 50% pooled human serum), and intermediate. (8) Adherence of bacteria to HEp-2 cells An assay developed to measure adherence of group B streptococci to epithelial cells was adapted for use with Moraxella catarrhalis. This assay is based in the binding of fluorescein – labeled bacteria to monolayers of larynx (HEp-2) epithelial cells in vitro, as determined by a fluorescence-based micro titer plate reader(8). Molecular Techniques Methods for strain typing These methods include enzymatic bio typing, polyacrylamide gel electrophoresis of whole cell protein, immunoblotting, and pulsed – field gel electrophoresis and restriction fragment length polymorphism endonuclease analysis. Two DNA typing method probe generated restriction fragment length polymorphism analysis and single adapter modified fragment polymorphism analysis were recently used study the genetic relationships among 90 Moraxella catarrhalis strains. (7) 10 Treatment, Prevention and Control Animal models. Studies of the pathogenesis and host response to Moraxella catarrhalis infection have been limited by the absence of a good animal model of infection. Several studies suggest that Moraxella catarrhalis are generally susceptibleto amoxicillinclavulnate,2nd and 3rd generation cephalosporins, Macrolids, fluroquinolones etc. 11 6.3AIMS AND OBJECTIVES To identify Moraxella catarrhalis from clinical specimen (sputum, tracheal aspirates, BAL , blood, middle ear specimen). To determine the Antibiotic susceptibility pattern by disc diffusion method for the isolates. 7.MATERIALS AND METHODS 7.1 Source of data All the Moraxella catarrhalis isolated from clinical specimen like blood,middle ear effusions, sputum, tracheal aspirates, BAL in Microbiology department St Johns Medical college,Bangalore for a period of one year (approximately 30 samples)starting from December 2012. 7.2 Inclusion criteria 1. Moraxella catarrhalis grown from sputum samples where WBC’s is 10 times the number of Squamous epithelial cells and there are 3 to 4 + of Gram negative diplococcic seen will be included . 2. In all other samples ( middle ear effusion,tracheal aspirates,BAL ) if there is Gram negative diplococci associated with inflammatory cells is included. 3. In blood sample where there is pure growth of Moraxella catarrhalis will be included. 7.3 Exclusion criteria Nil 12 7.4 Methods a) Gram’s stain Gram negative diplococcus with flattened abutting sides. The sample should be evaluated by microscopy prior to culture to make sure that the Gram negative diplococci are present . In sputum samples if the number of WBC’s is 10 times the number of Squamous epithelial cells and there are 3 to 4 + of a single morphotype of bacteria, accept the specimen for culture. b)Culture These sample will be plated on the following media Blood agar Chocolate agar Mac Conkey agar 13 Colonies on Blood agar and Chocolate agar are round, opaque, convex and greyish white. The colonies remains intact when pushed across the surface of the agar and no growth will be obtained in MacConkey agar. Do Grams stain ,if gram negative diplococcous with flattened abutting sides present Do Catalase and Oxidase test, if positive Go to further identification of Moraxella catarrhalis by following method c)DNAse test This test detects the degradation of DNA by bacterial species that produce DNase. It can be tested by using DNAse agar. The agar should be inoculated with the organisms and incubated at 370C for 18 – 24 hours. The plate should be flooded with 1 M HCl that precipitates DNA and turns the medium cloudy. The presence of a zone of clearing around the area of growth indicates DNAse production. 14 d)Method of rapid identification of Moraxella catarrhalis Butyrate esterase (tributyrin test) The rapid identification of Moraxella catarrhalis is important. The tributyrin spot test will differentiate Moraxella catarrhalis from Neisseria species. The enzyme butyrate esterase produced by Moraxella catarrhalis hydrolyses the tributyrin substrate in buffered salt medium. The reaction yields butyric acid which lowers the pH of the medium resulting in a yellow colour change. Antibiotic Susceptibility Disc Diffusion Method Media – Muller Hinton Agar with (5%) sheep blood Method Inoculum is prepared visually to match the turbidity of 0.5 McFarland standard. Do a lawn culture on MHA with sheep blood.Place the disc on media. Incubate at 350 C for 16 – 18 hours in 5 %co2. Antimicrobial agents used Selected according to CLSI guidelines 2011 Amoxicillin/clavulanate Cefuroxime Cefpodoxime Cefixime Azithromycin Clarithromycin 15 Ciprofloxacin Levofloxacin Beta lactamase testing Nitrocefin has very high affinity for bacterial beta lactamase. A nitrocefin disc is removed from the container and placed on a slide or on a empty petri dish lid. The disc is moistened with a loopfull of distilled water. A small amount of organism is applied on the moistened nitrocefin disc and incubated for 5 minutes in room temperature. Development of pink red colour if the isolate is beta lactamase positive 7.3 Does the study require any investigation or interventions to be conducted on patients or other human beings? No, study will be done on isolates obtained from clinical sample only. 7.4 Has ethical clearance been obtained from your institution in case of 7.3 Not applicable 16 8.LIST OF REFERENCES 1)Subhash Chandra parija 2009,page 334, Parijas text book of Microbiology and Immunology,Elsevier.A division of Reed Elsevier 2)S. Peter Borriello,Pattrick . R . Murray and Guido funke, 2005 Chapter 49 page 1305-1308Acinetobacter and Moraxella,Topley and Wilsons Microbiology and Microbial Infections,Bacteriology Volume 2,10th edition.Edward Arnold (Publishers) Ltd. 3) . Timothy F Murphy, Aimee L. Brauer, Brydon J. B. Grant and Sanjay Sethi Moraxella catarrhalis in Chronic Obstructive Pulmonary Disease Burden of Disease and Immune Response. Journal of Respiratory Critical.Care Med.2005.vol 172.pp 195-199 DOI: 10.1164/rccm.200412-1747oc on April 1,2005 4)FarisBakri,Aimee L. Brauer, Sanjay Sethi and and Timothy F. Murphy Systemic and Mucosal Antibody Response to Moraxella catarrhalis after Exacerbations of Chronic Obstructive Pulmonary Disease.Journal of Infectious Diseases.2002 ;185:632-40 5) H. V.Prashanth , R. M. Dominic Saldanha ,ShaliniShenoy Moraxella catarrhalis A Rediscovered Pathogen. International Journal of Biological& Medical Research2011; 2 (4):979-981 6) Timothy F. Murphy G.IyerParameswaran ,Ellie J.C. Goldstein Moraxella catarrhalis, a Human Respiratory Tract Pathogen . Clinical Infectious Diseases. 2009; 49:124-31 7)Washingtonc.Winnetalchapter 11.Konemans color Atlas and Textbook of Diagnostic Microbiology,Edition 6 .Lippincot Williams and Wilkins. 8) Hester J. Bootsma1, Han G. J. van der Heide, Simone van de Pas, Leo M. Schoulsand Frits R. Mooi Analysis of Moraxella catarrhalis by DNA Typing: Evidence for a Distinct Subpopulation Associated with Virulence Traits Journal of Infectious Diseases. 2000;181:1376-87 17 9. SIGNATURE OF CANDIDATE DR. MARY DIAS 10. NAME AND DESIGNATION OF ASSISTANT PROFESSOR THE GUIDE DEPARTMENT OF MICROBIOLOGY, ST.JOHN’S MEDICAL COLLEGE, BANGALORE – 34 11. REMARKS OF THE GUIDE SIGNATURE OF THE GUIDE HEAD OF THE DEPARTMENT DR. S. MURALIDHARAN PROFESSOR AND HEAD DEPT. OF MICROBILOGY ST.JOHN’S MEDICAL COLLEGE BANGALORE – 560034 12. SIGNATURE OF THE HEAD OF THE DEPARTMENT REMARKS OF THE DEAN OF THE INSTITUTION SIGNATURE OF THE DEAN 18 19