Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
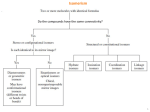
7 Visceral Situs, Heart Position, and Aortic Arch Position The second step in interpretation of a chest radiograph obtained in a new patient is to ascertain visceral situs, the heart position, and the position of the aortic arch relative to the trachea. For example, the radiographic report may start with this sentence: “The radiograph shows situs solitus, levocardia and a left aortic arch.” ■ Visceral Situs Visceral situs refers to the pattern of arrangement of the body organs relative to the midline. There are four types of visceral situs: situs solitus, situs inversus, heterotaxy with thoracic right isomerism, and heterotaxy with thoracic left isomerism (Fig. 7.1).1–4 Visceral heterotaxy has also been described as situs ambiguus, which means uncertain situs. This term should be abandoned because the situs is not uncertain but rather needs more words to describe it precisely. The structures that are helpful in determination of the situs include (1) the gastric air bubble, (2) the larger lobe of the liver, (3) the tip of the spleen, (4) the bronchi and pulmonary arteries, (5) the minor fissure, and (6) the azygos vein. The basic concepts regarding visceral situs is discussed in detail in Chapter 2. In situs solitus, the gastric air bubble is on the left side, and the larger lobe of the liver is on the right side (Fig. 7.2). The splenic tip can often be identified when the stomach and adjacent bowel loops are filled with air. When the bronchial air column can be traced, an asymmetric bronchial branching pattern with a short right and a long left main bronchus can be appreciated on the frontal radiograph. Normally the left main bronchus is 1.5 to 2 times longer than the right main bronchus. At the pulmonary hilum, the left pulmonary artery is seen slightly higher than the right pulmonary artery. The left pulmonary artery is seen above the left upper lobe bronchus, whereas the right pulmonary artery (in fact, its descending branch) is seen below the right upper lobe bronchus. An asymmetric branching pattern of the bronchi and pulmonary arteries is also evident on the lateral radiograph. As the upper lobe bronchi normally have horizontal courses, they are seen as two round lucencies arranged superoinferiorly in the middle mediastinum. The right upper lobe bronchus is located approximately one vertebral height above the left upper lobe bronchus. The right Fig. 7.1 Four types of visceral situs. GB, gallbladder; IVC, inferior vena cava; PA, pulmonary artery; SVC, superior vena cava. 68 7 Visceral Situs, Heart Position, and Aortic Arch Position Fig. 7.2 Situs solitus. Magnified views of the hilar anatomy (lower panels). Asterisks on the magnified frontal view mark the upper lobe bronchi. The left main bronchus is twice as long as the right main bronchus in this individual (solid lines). pulmonary artery lies anterior and slightly inferior to the right upper lobe bronchus. The left pulmonary artery lies posterior and superior to the left upper lobe bronchus. In short, the right upper lobe bronchus lies higher than the left, and the left pulmonary artery lies higher than and posterior to the right pulmonary artery. The minor fissure may cast a horizontal linear shadow over the midzone of a trilobed right lung. Situs inversus is characterized by a mirror-image arrangement of the visceral organs (Fig. 7.3). The gastric bubble is on the right and the larger lobe of the liver on the left. However, it is important to understand that the situs should not be called “situs inversus” solely because of the inverted positions of the gastric bubble and hepatic shadow. Plain film diagnosis of situs inversus can only be made when an inverted bronchial and pulmonary arterial branching pattern is clear. A lateral radiograph is helpful in differentiating the lateralized situs (i.e., situs solitus and inversus) from the symmetric situs (i.e., right isomerism or left isomerism). Normal hilar arrangement of the upper lobe bronchi and branch pulmonary arteries on the lateral view with a right-sided gastric bubble on the frontal view is highly suggestive of situs inversus even if the splenic shadow is not identified. In right isomerism, the hepatic shadow usually extends across the upper abdomen (Fig. 7.4). The gastric bubble can be seen on either side but tends to be closer to the midline. Interestingly, about 15% of patients with right isomerism have a hiatal hernia (Fig. 7.5).5 Hiatal hernia can be regarded as a manifestation of visceral heterotaxy. Bilaterally short bronchi can be appreciated in a welltaken frontal radiograph (Fig. 7.6). However, this feature is often unclear in infants. On the lateral radiograph, the end-on shadows of the upper lobe bronchi are seen at the same or similar horizontal level, and the pulmonary arterial shadow is seen mostly in front of the bronchi (Fig. 7.4). The presence of bilateral minor fissures indicates right isomerism (Fig. 7.7). In fact the diagnosis of right isomerism can be entertained when the minor fissure is present on the same side as the stomach even when a minor fissure is identified only on one side (Fig. 7.4, left panel). This is because the minor fissure and stomach cannot be 69 70 II Systematic Approach to Chest Radiographs Fig. 7.3 Situs inversus. The frontal view shows mirror-image arrangement of the bronchial and pulmonary arterial trees. Asterisks mark the upper lobe bronchi.The lateral view appears identical to that seen in on the same side in either situs solitus or situs inversus, and no minor fissure is present in either lung in left isomerism. However, a potential pitfall is the presence of an accessory fissure, which can simulate a horizontal fissure (Fig. 7.8).6,7 Right isomerism is associated with complex Fig. 7.4 Heterotaxy with thoracic right isomerism. The hepatic silhouette extends symmetrically across the upper abdomen. The stomach with a nasogastric tube in place is on the right side, lying somewhat close to the midline. A minor fissure is visible in the right lung. The presence of a minor fissure on the same side of the stomach is conclusive situs solitus (Fig. 7.2) but note the difference in labeling. This patient had Kartagener’s syndrome with subtle pulmonary infiltrates in the right lower lung. congenital heart disease in almost all cases. We have not seen any single case of right isomerism without complex congenital heart disease. As pulmonary atresia or stenosis is present in the majority of cases, the pulmonary vascularity is usually reduced (Figs. 7.4, 7.5, 7.6, and 7.7). evidence of right isomerism. On the lateral view, the similar length of the right and left main bronchi results in the upper lobe bronchi being projected at a similar horizontal level. The right and left pulmonary arteries are projected mostly in front of the upper lobe bronchi. 7 Visceral Situs, Heart Position, and Aortic Arch Position Fig. 7.5 Ectopic location of a part of the stomach in the thorax, which is often described as hiatal hernia, in a neonate with abdominal heterotaxy and thoracic right isomerism. Left isomerism is also characterized by a symmetric visceral arrangement. However, the hepatic shadow in left isomerism is usually less symmetric than in right isomerism, and it is not uncommon for the hepatic shadow to be indistinguishable from that seen in situs Fig. 7.6 Symmetrically short main bronchi are shown in this frontal radiograph in a child with right isomerism. This feature is not usually as apparent in neonates and small children. Asterisks indicate the origins of the upper lobar bronchi. solitus or inversus (Fig. 7.9). The gastric bubble can be on either side. The splenic shadow can be identified along the greater curvature of the stomach. On the frontal radiograph, bilaterally long bronchi can often be appreciated (Fig. 7.9, right panels). On the lateral radiograph, the upper lobe bronchi cast end-on shadows at the same or similar horizontal level, and the pulmonary arterial shadow is mostly seen behind the bronchi. The presence of a minor fissure in either lung excludes the Fig. 7.7 Bilateral minor fissures (arrows) in a neonate with right isomerism. 71 72 II Systematic Approach to Chest Radiographs Fig. 7.8 Accessory left anomalous fissure simulating the appearance of bilateral minor fissures in an infant with situs solitus and hypoplastic left heart syndrome. Right isomerism was suspected, but there was a situs solitus arrangement of the other organs. An accessory left minor fissure is not an uncommon normal variant.6,7 diagnosis of left isomerism. In approximately 80% of cases, left isomerism is associated with interruption of the inferior vena cava with azygos or hemiazygos venous continuation. 8 In this situation, the dilated azygos vein can be identified in the area of the tracheobronchial angle (Fig. 7.9, left panels). Absence of the inferior vena caval shadow on the lateral radiograph has also been described in patients with an interrupted inferior vena cava. We find this feature unreliable. As interruption involves the postrenal prehepatic segment of the inferior vena cava, the posthepatic segment of the inferior vena cava is present and collects the hepatic veins. Therefore, a web-like shadow, albeit somewhat smaller than normal, can be identified in the lateral radiograph. In addition, the inferior vena caval shadow can be hidden by the posteriorly enlarged heart. In contrast to right isomerism, left isomerism is not always associated with congenital heart disease. Left isomerism may be seen as an incidental finding in otherwise normal individuals or in patients with an arrhythmia or biliary atresia.9 It should be remembered that there are exceptions, although rare, to these rules, as discussed in Chapter 2. Fig. 7.9 Heterotaxy with left isomerism. Magnified views of the hilar anatomy (lower panels). The hepatic silhouette is not as asymmetric as it is in situs solitus or situs inversus, but is not as symmetric as it is in right isomerism. The splenic silhouette is barely visible lateral to the stomach (arrow). Symmetric bronchial branching can be appreciated on the frontal radiograph. The dilated azygos vein is seen above the right tracheobronchial angle. The trachea is mildly bent to the right by the left aortic arch. The lateral view shows the upper lobe bronchi at a similar horizontal level because of a similar length of the right and left main bronchi. The right and left pulmonary arteries cast a shadow mostly behind and above the upper lobe bronchi. The inferior vena caval shadow is not obvious on the lateral view. 7 Visceral Situs, Heart Position, and Aortic Arch Position Fig. 7.10 Three cardiac positions defined by the location of the main part of the heart relative to the midline. ■ Heart Position The cardiac position is described by using the terms levocardia, dextrocardia, and mesocardia (Fig. 7.10), which describe where the main part of the heart is located within the thorax. These terms are not used when the heart is displaced to one or the other side due to extracardiac pathology, such as hypoplasia of a lung or deformity of the thoracic cage (Fig. 7.11). When the heart is partially or completely outside the thorax, it is called ectopia cordis. Usually the cardiac apex points toward the side where the main part of the heart is positioned. However, there are exceptions where the cardiac position and the base-apex orientation are not matched. Fig. 7.11 (A) Rightward displacement of the heart due to right lung hypoplasia in a patient with absence of the right pulmonary artery in the mediastinum and (B) in another patient with scimitar syndrome. When defining the position of the heart on a chest radiograph, it is important to check whether there is any obliquity of radiographic projection. A subtle obliquity may bring the cardiac silhouette to the other side of the thorax (see Fig. 6.2). In general, the cardiac silhouette is brought to the right when the radiograph is obtained in a left anterior or right posterior oblique projection, whereas it is brought to the left when the radiograph is obtained in a right anterior or left posterior oblique projection. Although there are many exceptions, levocardia tends to have the right-sided right ventricle and the left-sided left ventricle (so-called D-loop ventricles), whereas dextrocardia tends to have the left ventricle on the right and the right ventricle on the left (so-called L-loop ventricles). This tendency explains why congenitally corrected transposition The displaced cardiac position in scimitar syndrome is often called dextroposition, which is a confusing term. 73 74 II Systematic Approach to Chest Radiographs Fig. 7.12 Discordant visceral situs and heart position. Situs solitus and dextrocardia (left panel). Situs inversus and levocardia (right panel). Both cases had congenitally corrected transposition of the great arteries. of the great arteries is the most common diagnosis when there is discordance between the heart position and visceral situs, such as dextrocardia with situs solitus (Fig. 7.12, left panel) and situs inversus with levocardia (Fig. 7.12, right panel). ■ Position of the Aortic Arch The reference structures used for the determination of the left- or right-sidedness of the aortic arch are the trachea and main bronchi.10 The left aortic arch courses backward on the left side of the trachea and above the left main bronchus, Fig. 7.13 Aortic arch positions relative to the trachea. The trachea normally shows indentation on the side of the aortic arch. The most proximal part of the descending aorta (arrows) can be traced on the same Ao, ascending aorta; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle. whereas the right aortic arch courses backward on the right side of the trachea and above the right main bronchus. Chest radiographic determination of the aortic arch position depends largely on the indentation of the tracheal air column. A left aortic arch indents and bends the trachea to the right side, whereas a right arch indents and bends the trachea to the left (Fig. 7.13). In almost all cases, the aortic arch continues with the proximal descending aorta on the same side, which is usually identifiable as a vertical stripe along the spine. The rare exceptions are the so-called circumflex retroesophageal aortic arches in which the distal segment of the aortic arch crosses the midline behind the esophagus to connect to the descending aorta on the opposite side10,11 (Fig. 7.14). When there side of the aortic arch. Bilateral indentation is typically seen in double aortic arch but other forms of vascular ring cannot be excluded. Fig. 7.14 Circumflex retroesophageal right aortic arch (right aortic arch with a left descending aorta). The proximal aortic arch is on the right side, whereas the distal arch has a retroesophageal course to con- nect to the descending aorta on the left side of the spine. The tracheal indentation is on the right side with the descending aorta seen on the left (arrows). A B Fig. 7.15 Cervical left aortic arch in a 14-year-old patient. (A) Chest radiograph and coronal magnetic resonance (MR) image show the aortic arch (arrows) reaching the upper thorax above the level of the clavicle (C). (B) Contrast-enhanced MR angiogram seen from the left side shows a tortuous aortic arch, aneurysmal dilatation (asterisks) in the distal aortic arch and left subclavian artery (LSA) and severe long segment narrowing of the proximal descending aorta. Dilated intercostal arteries are seen as collateral channels. As an incidental finding the left innominate vein (LIV) takes a retroaortic course. Ao, ascending aorta; LV, left ventricle. 76 II Systematic Approach to Chest Radiographs is double aortic arch, the trachea is bent to neither side or bent only slightly to the side of the smaller aortic arch. The trachea may show bilateral indentations with concentric narrowing of its lumen (Fig. 7.14). The descending aorta can be seen on either side, although a left-sided descending aorta is more frequent. The aortic arch can be unusually high, its apex reaching above the level of the clavicle (Fig. 7.15). This condition is called a cervical aortic arch.10,12 It occurs more commonly with a right aortic arch, often taking a retroesophageal course. It is commonly associated with tortuosity, aneurysmal dilatation, and narrowing. Pearls ■ The situs can be accurately defined when the bronchial branching pattern is clearly shown. ■ Cardiac position has nothing to do with the type of visceral and atrial situs. ■ A right-sided gastric air bubble is not a specific sign for situs inversus, as it can also be seen with right and left isomerism. A right-sided gastric air bubble simply means that the situs is not normal. ■ Levocardia tends to occur with D-loop ventricles (right ventricle on the right), and dextrocardia with L-loop ventricles (right ventricle on the left), but there are many exceptions. ■ The presence of a minor fissure in both lungs is a definitive sign for right isomerism. However, its absence means nothing. ■ A left aortic arch indents the left side of the trachea, and a right aortic arch indents the right side of the trachea. ■ The presence of a minor fissure on the same side of the stomach is a definitive sign of right isomerism. ■ The stripe of the descending aorta is seen on the same side as the aortic arch in most cases. ■ Symmetry of the right and left lobes of the liver is highly suggestive of right isomerism, especially when the heart is not enlarged and the pulmonary vascularity is diminished. ■ ■ A dilated azygos vein on either side is highly suggestive of left isomerism, but can be seen in other conditions such as superior or inferior vena caval obstruction. In double aortic arch, the trachea bends to neither side if the arches are symmetric in size. When the arches are asymmetric in size, the trachea may bend to the side of the smaller arch. The descending aorta can be seen on either side. References 1. Stanger P, Rudolph AM, Edwards JE. Cardiac malpositions. An overview based on study of sixty-five necropsy specimens. Circulation 1977; 56:159–172 2. Van Praagh R. Terminology of congenital heart disease. Glossary and commentary. Circulation 1977;56:139–143 3. Uemura H, Ho SY, Devine WA, Anderson RH. Analysis of visceral heterotaxy according to splenic status, appendage morphology, or both. Am J Cardiol 1995;76:846–849 4. Nagel BHP, Williams H, Stewart L, Paul J, Stümper O. Splenic state in surviving patients with visceral heterotaxy. Cardiol Young 2005;15: 469–473 5. Hsu JY, Chen SJ, Wang JK, Ni YH, Chang MH, Wu MH. Clinical implication of hiatal hernia in patients with right isomerism. Acta Paediatr 2005;94:1248–1252 6. Abiru H, Ashizawa K, Hashmi R, Hayashi K. Normal radiographic anatomy of thoracic structures: analysis of 1000 chest radiographs in Japanese population. Br J Radiol 2005;78:398–404 7. Gesase AP. The morphological features of major and accessory fissures observed in different lung specimens. Morphologie 2006;90:26–32 8. Applegate KE, Goske MJ, Pierce G, Murphy D. Situs revisited: imaging of the heterotaxy syndrome. Radiographics 1999;19:837–852, discussion 853–854 9. Gilljam T, McCrindle BW, Smallhorn JF, Williams WG, Freedom RM. Outcomes of left atrial isomerism over a 28-year period at a single institution. J Am Coll Cardiol 2000;36:908–916 10. Yoo SJ, Bradley TJ. Vascular rings, pulmonary artery sling and related conditions. In: Anderson RH, Edward JB, Penny D, Redington AN, Rigby ML, Wernovsky G, eds. Pediatric Cardiology, 3rd ed. Philadelphia: Elsevier, 2009, in press 11. Philip S, Chen SY, Wu MH, Wang JK, Lue HC. Retroesophageal aortic arch: diagnostic and therapeutic implications of a rare vascular ring. Int J Cardiol 2001;79:133–141 12. Baravelli M, Borghi A, Rogiani S, et al. Clinical, anatomopathological and genetic pattern of 10 patients with cervical aortic arch. Int J Cardiol 2007;114:236–240