Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
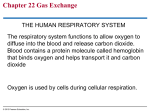
ODESSA NATIONAL MEDICAL UNIVERSITY Department of Surgery № 1 METHODOLOGICAL INSTRUCTIVE ELABORATION of the practical lesson from the discipline "Surgical diseases with child's surgery and oncology" for students Module № 4. "Symptoms and syndromes in surgery" Semantic module № 8. "Clinical displays of surgical diseases". Theme № 20. «Modern methods of diagnostics and medical treatment of diseases of the cardiovascular and respiratory systems». Discussed and ratified onto the methodical conference of the Department "29" auguct 2014 р. Protocol № 1. Head of the Department Professor __________Grubnik V.V. ODESSA - 2014 2 1. Theme of the lesson: «Modern methods of diagnostics and medical treatment of diseases of the cardiovascular and respiratory systems» - 6 hours. 2. Actuality of theme. Cardiovascular diseases are main reason of disability and ahead of early death of people economic the developed states. Today the fate of these diseases in the structure of death rate makes 40-60%, getting up of morbidity and defeat of habitants of our planet of young age is here marked, that does cardiovascular diseases by the most important medical-social problem of health protection. On economic prognoses in the third millennium expense the health protection related to medical treatment of lungs diseases will exceed charges on the fight against the diseases of the cardiovascular system and oncologic diseases. Contamination of atmospheric air, prevalence of smoking, including passive smoking, abuse by an alcohol, supercooling of organism, considerable frequency of acute bronchitis and pneumonias in a period of epidemics of flu, change of reactivity of organism of person, and also failings in organization of medical treatment is instrumental in growth of prevalence of lung diseases. Growth of morbidity of population by the diseases of lungs points to the increase of sizes of losses of society from disabled. With age there is growth of number of chronic diseases of lungs. It gives to the problem of diseases of lungs not only medical-biologic and social-hygienic but also economic value. 3. Purpose of lesson. 3.1. General purpose. - to acquaint students, to make the picture of pathology of cardiovascular and respiratory systems organs, methods of diagnostics and medical treatment. - to master terminology which is used in clinical medicine; - to master methodology which is used at raising of diagnosis of diseases of the cardiovascular and respiratory systems; - to master information about the methods of laboratory-instrumental diagnostics in internal medicine. 3.2. Educate purpose. - to form deontological principles of examination and treatment of patients with the diseases of the cardiovascular and respiratory systems; - taking into account the psychosomatic aspects of pathogenesis of these diseases; - to develop sense of legal responsibility for a timeliness and rightness of choice of optimum method of the cardiovascular and respiratory systems diseases medical treatment. 3.3. Concrete purpose. - to know: 3 - Knowledge of basic moments of clinical picture of the most widespread diseases of the cardiovascular and respiratory systems. - Knowledge of testimonies and contra-indications to conducting of major instrumental researches at diagnostics of the cardiovascular and respiratory systems diseases. - Knowledge of diagnostic possibilities and limitations of major methods of instrumental diagnostics. - Understanding of principles of modern therapy of the most widespread diseases of the cardiovascular and respiratory systems. 3.4. On the basis of theoretical knowledges from a theme: - to capture methods(to be able): - To give possibility to capture skills and technique of execution of methods of investigations of the cardiovascular and respiratory systems to the students; - To give to the students of ability to conduct the clinical investigation of the cardiovascular and respiratory systems; - to analyze the results of researches; - to differentiate the disease of the cardiovascular and respiratory systems; - to appoint medical treatment depending on the exposed pathology; - to define the indications and contraindications to surgical interference, to choose optimum access and volume of operative medical treatment; - correctly to estimate possible complications during operation and in a postoperative period; - to define the rehabilitation of patients and a little rather clinical supervision; - to design a medical document. № Discipline 4. Interdisciplinary integration To know Previous disciplines 1 Anatomy 2 Physiology Anatomy of the pectoral cavity organs Lungs and heart physiology 3 Propaedeutics of internal diseases Methods of cardiovascular and respiratory systems examination To be able To define the function of the external breathing and parameters of blood circulation To be able to expose the scopes of heart, to conduct lungs and heart percussion and auscultation Next disciplines 1 Cardiology 2 Pulmonology Clinical signs and changes on ECG at the acute infarction of myocardium Clinical signs of lungs diseases and displays of them on the roentgenogram of pectoral cavity organs To read ECG To expose the changes of pectoral cavity organs on the roentgenogram Inter-subject integration 4 1 Thoracic Surgery 2 Cardiosurgery Exigent states of pectoral cavity organs diseases Signs of acute coronary syndrome To give exigent help To be determined with the algorithm of modern diagnostics and medical treatment 5. Table of contents of theme Methods of respiratory organs investigation. 1. Question: complaints of patient and their semiological estimation. Examination and palpation of thorax 2. Roentgenologic investigation For investigation of respiratory organs apply roentgenoscopy, roentgenography, bronchography and tomography of lungs. Roentgenoscopy is the most widespread method of investigation, which allows by sight to define the change of transparency of pulmonary fabric, to expose the hearths of compression or cavity in it, to expose the presence of liquid or air in a pleura cavity, and also other pathological changes. Roentgenography is used with the purpose of registration and document of exposed at roentgenoscopy of changes in the respiratory organs on x-ray photography tape. At pathological processes in lungs, that point to the loss of lungs compression of pulmonary tissue (pneumonia, lungs infarction, tuberculosis and etc.), the proper areas of lungs on negative tape have more pale image as compared to normal pulmonary tissue. A cavity of lungs that contains air and is surrounded by inflammatory roller, on negative x-ray photography tape has the appearance of dark patch of the oval form surrounded by more pale shade, than shade of pulmonary tissue. A liquid in a pleura cavity, which is less penetrable for x-rays as compared to pulmonary tissue, on negative x-ray photography tape gives shade, paler as compared to shade of pulmonary tissue. A roentgenologic method allows to define not only the amount of liquid in a pleura cavity but also its character. At presence of pleura of inflammatory liquid or exudate in a cavity the level of collision of it with lungs has a slanting line, that gradually follows upwards and lateral from a midclavicular line; at accumulation in the pleura cavity of noninflammatory liquid or transudate the level of it is disposed more horizontally. Tomography is the special method of roentgenography that allows producing layer roentgenologic investigation of lungs. It is used for diagnostics of tumours of bronchial tubes and lungs, and also small infiltrates, cavities and cavities which are bed on a different depth of lungs. Bronchography is used for investigation of bronchial tubes. To the patient after previous anaesthesia of respiratory tracts the contrasting substance is entered in the road clearance of bronchial tubes, that detains x-rays (for example, jodolipole), then execute roentgenoscopy of lungs and get the expressive image of bronchial tree on a roentgenogram. This method allows diagnosing expansion of bronchial tubes (bronchiectasis), abscesses and cavities of lungs, narrowing of road clearance of large bronchial tubes by a tumour or strange body. Fluorography also is the variety of roengenography research of lungs. It is conducted by the special vehicle - fluorographe, that allows doing a radiograph on 5 a mini-informative film, and is used for the mass prophylactic survey of population. Computer tomography (КТ) is the investigation, that allows to get the xray photography image of transversal cuts of thorax and its organs with the very large clearness of image and large deciding ability. On transversal cuts it is possible expressly to distinguish the changes conditioned by a pathological process in pulmonary tissue, tracheas, bronchial tubes, lymphatic knots of mediastinum, more precisely to define prevalence of pathological process, its mutual relations with other organs, presence of sweat selection in a pleura cavity and changes of pleura at tumours. Magnetic-resonance tomography. A method allows to differentiate tumours from cysts and vascular new formations, as changes in vessels it is good noticeable on the got images without introduction of contrasting substance. Endoscopic investigation To the endoscopic methods of investigations bronchoscopy and thoracoscopy are takes. Bronchoscopy is used for the review of mucus shell of trachea and bronchial tubes of the first, second and third order. It is executed by the special device - bronchoscopy which the special tongs for a biopsy are added to, drawing out of foreign bodies, deleting of polypuses, photo-prefix et cetera. Before introduction of bronchoscopy anaesthesia by a 1-3% solution of dicaine mucus shell of overhead respiratory tracts is conducted. Then bronchoscopy is entered through a mouth and glottis in a trachea. A doctor that explores, examines the mucus shell of trachea and bronchial tubes; by the special tongs on a long handle it is possible to take the piece of tissue from a suspicious area (biopsy) for histological and cytological investigation, and also to take picture of it. Bronchoscopy is applied for diagnostics of erosions, ulcers of mucus shell of bronchial tubes and tumour of bronchial wall, drawing out of foreign bodies, deleting of polypuses of bronchial tubes, medical treatments of bronchiectatic disease and centrally located abscesses are lungs. In these case through bronchoscopy festering the sputum is sucking-off at first, and then antibiotics are entered in the road clearance of bronchial tubes or cavity. Thoracoscopy is executed by the special device - rhoracoscope, which consists of hollow metallic tube and special scope with an electric light bulb. It is used for the review of visceral and parietal sheets of pleura, taking of biopsy, disconnection of pleura joints and conducting of row of other manipulation treatments. Methods of functional diagnostics The methods of functional diagnostics of the external respiratory system matter very much in the complex examination of patients suffering by the diseases of lungs and bronchial tubes. They enable to expose the presence of respiratory insufficiency quite often long before appearance of the first clinical symptoms, to set its type, character and measure of expressed, to trace the dynamics of change of functions of vehicle of the external respiration in the process of development of disease and under act of medical treatment. 6 Pulmonary ventilation. The indexes of pulmonary ventilation do not have severe constants: in most they not only are determined by pathology of lungs and bronchial tubes, but depend also to a great extent from constitution and physical training, growth, mass of body, sex and age of person. Therefore findings are estimated as compared to the so called proper sizes, that take into account all these information and that are a norm for the explored person. The proper sizes are calculated on nomogrammes and formulas determination of the proper basic exchange lies in basis of which. Pleural puncture Pleural puncture is used for determination of character of pleura liquid with the purpose of clarification of diagnosis and for deleting of liquid from a pleura cavity and subsequent introduction at it of medicinal matters with a medical purpose. Before puncture conduct treatment of the manipulation field by an iodine with an alcohol and local anaesthesia in the place of puncture. Puncture usually conduct on a back axillary line between seventh and eighth ribs on the overhead edge of rib (see image 1). Figure 1. 1 - Line of Damoiseau; 2 – Garlend’s triangle; 3 - the RauhfussGrokko’s triangle; 4 - low bound of lungs. With a diagnostic purpose take 50-150 ml liquids and send it on cytological and bacteriological investigation. With a medical purpose at accumulation of a plenty of liquid in a pleura cavity 800-1200 ml liquids are taken at first. Deleting from the pleura cavity of greater amount of liquid results in the rapid change of organs of mediastinum in a sick side and can be accompanied by a collapse. For drawing out of liquid use special syringe by volume of 50 ml or the Poten’s vehicle. The liquid got from a pleura cavity can have the inflammatory (exudate) or non-inflammatory (transudate) origin. With the purpose of differential diagnostics of liquids character determine its specific weight, amount of albumen, which is contained in it, red corpuscles, leucocytes, mesotelial and atypical cages. Specific gravity of inflammatory liquid 1,015 and higher, maintenance of albumen more than 2-3%, and the Rivalt’s test is positive. Specific gravity of transudate less than 1,015, amount of albumen less than 2%, the Rivalt’s test is negative. For conducting of the Rivalt’s test take a cylinder by volume of 200 ml, fill it with plumbing water, 5-6 drops of strong vinegar acid are added at it, and then 7 by a pipette a few drops of pleura liquid are dropped at it. Appearance of turbid cloud in the place of dissolution of drops testifies to inflammatory character of pleura liquid, that contains the promoted amount of serosomucine (positive reaction, or the Rivalt’s test). The non-inflammatory liquid of turbid cloud does not give (negative Rivalt’s test). Sputum investigation Microscopic sputum investigation is produced both in native and in the painted preparations. The cages of malignant tumours quite often get in sputum especially if a tumour grows endobronchially or disintegrates. In native preparation these cages are selected by its non-typicalness: by largenesses, different, often by an ugly form, by a large kernel, sometimes by multinucleosis. Diagnostics of cardiovascular diseases Electrocardiogram (ECG) is one of the most widespread and more effective methods of diagnostics of cardiovascular diseases, based on the analysis of curve - result of fixing of electric tension in the muscle of working heart. For registration of electrocardiogram the special devices the electrocardiographs of different prospects are used. Usually this vehicle is a standard block which the reception of signals of ECG through the cable of taking (electrodes are imposed on a thorax, extremities of patient) is produced by, these signals are kept in memory, and also is represented on an indicator, is fixed on a paper - a curve is represented, that represents the changes in time of difference of potentials of the electric field (bio-potentials) of heart at his reductions. ECG is a valuable diagnostic instrument. It is possible to estimate the source (so called driver) of rhythm, regularity of cardiac reductions, and their frequency by it. All of it matters very much for diagnostics of different arrhythmias. On duration of different intervals and indents of ECG it is possible to judge about the changes of cardiac conductivity. The changes to eventual part of gastric complex allow a doctor to define a presence or absence of ischemic changes in a heart. Amplitude of indents is the important index of ECG. The increase speaks its about hypertrophy of appropriate departments of heart, which is observed at some diseases of heart and at hypertensive illness. Indicates to conducting of ECG: 1. The risks at the diseases of heart are basic factors: - Hypertensive disease - For men - age after 40 years - Smoking - Hypercholesterinemia - Carried infections - Pregnancy 2. Worsening of the state of patients with the diseases of heart, appearance of pains in the region of heart, development or strengthening of shortness of breath, origin of arrhythmia. 3. Before any operative interferences. 8 4. Disease of internal organs, endocrine glands, nervous system, illnesses of ear, throats, nose, skin diseases et cetera, at suspicion on bringing in of heart in a pathological process. The electrocardiograms monitoring (daily (Holter’s) monitoring) is investigation of electric activity of heart, that represents the rightness of its work during ordinary for the patient of the physical and emotional loadings, that is producible by the special device, that writes down an electrocardiogram during 24 hours. This procedure has some features. Five or seven electrodes will be glued on the thorax of patient. These electrodes join the writing down device which on a size and weight reminds a small transistor radio receiver or tape recorder. A patient will need to carry on itself this writing down the device provided with a humeral small strap, for a long day. A patient must mark in the special diary that he did during these days. If some symptoms, such as dizziness, pains in breasts, difficulty of respiration or feeling of trembling in breasts, unrhythmic work of heart and others like that, will appear, it costs to mark them in a diary. A doctor at the analysis of record will compare activity of heart with the symptoms marked in a diary. For diagnostics of defeats of vessels angiographic investigation of coronary vessels is actively used in a cardiologic clinic, coronary angiography is here, as a rule, logical completing by a link in the complex inspection of patient by ischemic heart disease (IHD), as is the most informing method for the decision of such important questions, as: - verification of the IHD diagnosis; - clarification of localization of defeat of vascular river-bed; - determination of tactic of medical treatment. Coronarography is roentgen-contrast method of investigation, which is the most exact and reliable method of the IHD diagnostics, allowing exactly to define character, place and measure of narrowing of coronary artery. Order of procedure of coronarography: - A patient is delivered in the cabinet of roentgen-vascular surgery. Procedure is mini-traumatic - during all procedure a patient is in consciousness. - After conducting of local anaesthesia proceed to investigation - the special catheter is conducted through a femoral artery and overhead part of aorta in the road clearance of coronary arteries. - In a number of cases a catheter is entered through the artery of forearm that diminishes the term of supervision after executed coronarography. - Through a catheter the roentgen-contrast substance which by the current of blood is carried on coronary vessels is entered. A process is fixed by the special setting - angiograph. - A result hatches on a monitor; except for it is placed in a digital archive. During coronarography a measure and size of defeat of coronary vessels is set, that determines subsequent tactic of medical treatment. Indications to coronarography conducting: 9 - high risk of complications from data of clinical and non-invasive examination, including at the without-symptom flow of ischemic heart disease; - uneffective of medicinal medical treatment of angina pectoris; - unstable angina pectoris, that does not respond to medicinal treatment, arose up at a patient with the heart attack of myocardium in anamnesis, is accompanied by dysfunction of left ventricle, arterial low blood pressure or edema of lungs; - postinfarction angina pectoris; - impossibility to define the risk of complications by non-invasive methods; - future operation on the opened heart (for example, prosthetics of valves, correction of innate vices of heart etc.) at a patient more senior 35 years. In a modern cardiology the possibility of exposure of initial stages of ischemic heart disease and atherosclerosis of coronary vessels at the patients of group of the promoted risk appeared by a non-invasive method. New method - virtual coronarography, allows exploring the state of vessels of heart, permeability of stents after shunting, to measure the level of calcification of vessels, to get the indexes of functions of heart. Research is conducted by modern computer tomograph apt at the transmission of 64 pictures after 0,4 sec. with subsequent treatment on a computer and creation of three-dimensional models of heart and vessels. Research duration makes 40-50 sec., does not require hospitalization and anesthesia. It is brought the contrasting substantion into an elbow vein, and the receipt of images is synchronized with the certain phase of cardiac cycle. Coronarography allows obtaining state information the vessels of heart and preventing development of heart attack of myocardium, and also reducing the risk of sudden death. USD of heart and vessels in medical practice, foremost, is used for recognition of heart diseases. It is used for diagnostics of ischemic heart disease angina pectoris, infarct of myocardium, states after the carried infarct of myocardium; diseases of muscular and external shells of heart (cardiomyopathies, pericarditises); at the diseases of peripheral arteries - cerebrum, lower extremities, organs of abdominal region, buds. All wider is used USD of heart and vessels for conducting of prophylactic examinations, as a method allows to expose disorders of operation of heart earlier in all. USD of heart and vessels is conducted by vehicles which allow getting the image and pictures during procedure. At research of heart a patient undresses to the belt, the forehand of thorax oils by the special gel, a doctor sets an ultrasonic sensor in different positions, that allows seeing different departments of heart and executing the necessary measuring. In a cardiology the ultrasonic methods of investigation are priority and own the row of advantages: - by non-invasion; - by safety; 10 - by availability; - by possibility of the repeated conducting of investigation. Echocardiography has high diagnostic meaningfulness. Dopplerography is inalienable part of ultrasonic investigation of heart and allows estimating blood flow in a heart and vessels in the real-time mode. Ultrasonic investigation (USD) of heart (echocardiography) and vessels allows getting the image of heart, its four chambers, valves; all of them are visible afoot in the real time. Use of the special principle of analysis of image - Doppler allows to document motion of blood into a heart and in vessels. Due to such approaches, USD of heart allows to estimate not only the structure of heart but also its functions. Echocardiography on the modern vehicles provided with computers allows getting the row of quantitative indexes which characterize the basic function of heart - retractive. Already on the early stages of decline of this function it is possible to recognize these violations and conduct the proper medical treatment. The repeated researches allow a doctor to estimate efficiency of medical measures. Echocardiography allows with large exactness to recognize the disease of external shell of heart - pericardium, bulge of sheets of pericardium, joints between them, presence of liquid in the cavity of pericardium. The tumours of heart appear expressly. Investigation of peripheral vessels exposes, mainly, narrowing of their road clearance. The loading test is a method at which a doctor does the record of electrocardiogram of patient at the physical loading. During investigation to the patient suggest to move on a path (treadmill), that hurries, or to twist the pedals of bicycle (veloergometre). The got results help to estimate the state of the cardiovascular system. More frequent a method is used for diagnostics of ischemic heart disease. Invasive electro-physiology investigation (EPI) First potential of the His’ bundle was written down by Scherlag et al. in 1969. Since then on electro-physiology research is widely drawn for diagnostics of violations of rhythm of heart. Due to development of new technologies at the last 10 years on the change analog 8 and 16 - the digital systems on the basis of the personal computer came to the channel devices, that allow not only to write down to 128 channels from one electrode, but yet the measured images build 3 th and 4th. Invasive ЕPІ is widely used presently, as a mean of diagnostics, medical treatment and prognosis in many clinical situations. For conducting of intra-cardiac ЕPI under local anaesthesia punctured the large veins (femoral or subclavicular) and through them under x-ray photography and ECG-control in the cavity of heart set one or a few multipolar electrodes for registration of electric activity of different departments of auricle, ventricles and the His’ bundle intra-cardiac electro-gramme and endocardial stimulations. The ЕPI essence consists in conducting of programmable stimulation of auricle or ventricles in combination with simultaneous registration the electro-grammes of different departments of heart and a few taking of ECG. 11 This research owns an indisputable diagnostic (receipt of information about character of violation of rhythm, its electro-physiology mechanism), therapeutic (estimation of therapy, that is conducted, and ablation of arrhythmogenic areas or additional ways of conducting) and prognostic value. In spite of this certificate to its clinical use formulated not enough expressly. This question requires the decision as the technician ЕPI, that earlier was the mean of difficult scientific researches only, accessible now into many regional medical centers. At the clinical use ЕPI it is necessary to take into account not only the relation risk-benefit but also efficiency of charges. Basic indexes to the ЕPI conducting: - there is a necessity in determination of electro-physiology mechanism of violations of rhythm; it is topical diagnostics of arrhythmogenic hearth and additional ways of conducting; - clarification the degree of malignant of gastric arrhythmias; - control after efficiency of medicinal anti-unrhythmical therapy at ventricle’s arrhythmias; - refractory to medicinal therapy paroxysmal tachycardia, that require ablation or surgical medical treatment; - diagnostics of the not clear syncopal states; Complications during conducting of intra-cardiac EPI: - bleeding from a puncture; - perforations of myocardium or vessels; - thrombophlebitis in the puncture place; - death from fibrillation of ventricles, by cardio-versus, that is not removed. One of basic methods of non-invasive diagnostics of violations of cardial rhythm is intra-esophageal electro-physiology investigation (IEEPI). Availability, safety and relatively low cost allow substantially extending its use. It appears that the IEEPI results in many cases coincide with invasive. Under IEEPI the aggregate of methods of electric stimulation of heart through a gullet, which together with registration of intra-esophageal electro-grammes during violations of rhythm of heart allow to estimate the functional state of different departments of the leading system of heart and obtain certain information about the possible mechanisms of arrhythmias origin, is understood. The IEEPI advantages: - allows to estimate the electro-physiology mechanism of supra-ventricle paroxysmal tachycardia, character of the antegrade conducting, and also most antegrade refractory periods of different departments of the leading system of heart; - the basic electro-physiology criteria of the supraventricular tachycardia diagnostics do not differ from the criteria of intra-cardiac ЕPІ; - non-invasive method, that does not require a dear apparatus and special laboratory. Lacks of method: - discomfort; 12 - does not allow to carry out topical diagnostics of additional ways, size of retrograde refractory periods of different departments of the leading system of heart. The IEEPI conducting contra-indicated at presence at patient of the following pathological states: - tumours, diverticules, scars, varicose expansion of veins of gullet, esophagitis; - stable motion of angina pectoris IV functional class; - electric instability of myocardium, conditioned by acute coronary syndrome (acute to THEM, first by arising up and making progress angina pectoris of tension); - by insufficiency of the III-IV functional class blood circulation; - aneurism of left ventricle, intra-cardiac blood clots, prosthetic appliances of valves; - acute infectious diseases. Indications to conducting of investigation: - diagnostics of weakness of sinoatrial node; - attacks of proof palpitation; - fainting fit of not clear etiology; - estimation of risk origin of blinking arrhythmia with high frequency of cardiac reductions at patients with premature excitation of ventricles; - selection of antiunrhythmical therapy by a patient with paroxysmal supraventricle tachycardia. IEEPI at patients with paroxysmal supra-ventricle tachycardia pursues aims: - to learn character of the antegrade atrioventricular conducting; - to expose and localize additional atrioventricular connections (the Kent’s bundle) which function in antegrade direction; - to learn the functional state of different departments of the antegrade leading system of heart; - to set the electro-physiology mechanism of paroxysmal supra-ventricle tachycardia; - to define the mode of electric stimulation, that allows to provoke and to cup off the attack of supra-ventricle tachycardia; - subsequent testing of efficiency of antiunrhythmical preparations in the conditions of IEEPI. The diagnosis of blinking arrhythmia usually does not represent substantial difficulties, if on ECG one paroxysm is registered even. The IEEPI role for diagnostics of fibrillation of auricle, similarly as well as at their trembling, is taken to the decision of the following tasks: - verification of origin of paroxysm of auricle trembling by its induction at patients with the undocumented attacks of palpitation; - differential diagnostics of trembling, twinkling of auricle with other variants of paroxysmal tachycardia with the wide complexes QRS. At development of paroxysmal tachycardia with the wide complexes QRS, that flows without the expressed haemodynamic disorders, expedient registration 13 the gullet the electro-grammes, allowing to conduct differential diagnostics between gastric tachycardia and antidromic tachycardia at the WPW syndrome, supra-ventricular tachycardia with the functional blockade of leg of the His’ bundle, and also to estimate possibility of tachycardia stopping by trans-esophageal electro-stimulation auricle. Speaking about diagnostics of rhythm violations, it is impossible not to reminisce a tilt-test, common in diagnostics of the syncopal states. In vertical position of body a blood is saved in feet, diminishing the vein returning. In a norm it points to reflex tachycardia and vasoconstriction. However at some people the increased reductions of ventricles on a background reduction of pre-loading activate mechanic-receptors, pointing to the acute activating of the parasympatic system, appearance in this connection of reflex hypotension and bradicardia and syncopal state. For the correct conducting there is the tilt-test (together with the proper equipment) necessary whole row of terms: weakly lighting, barely cool room without noises from outside. Tilt-test is used for the inspection of persons with the syncopal states. Place a patient on the special table and after the arterial pressure and pulse measuring quickly levitate overhead part of body with the angle of slope from 60% to 80% on 20 - 45 minutes. The use of isoproterinol allows to multiply the sensitiveness of this method, and also shorten research time. The initial dose of isoproterinol makes 2 milligrams with the subsequent increase of a to 8 milligram maximal. Isoproterionol strengthens the vasodilatation influencing, that points to the frequency of cardiac reductions reduction to the decline of arterial pressure up to development of the syncopal state at some patients. Medical treatment of thoracic organs 1. Medical bronchoscopy - Deleting of aspirating strange bodies. Medical possibilities of бронхоскопии long time were taken to deleting of аспірованих strange bodies, and now it is the unique bloodless method of their deleting from bronchial tubes. Development of flexible extractors and considerable experience accumulated to the present tense allows to consider that most aspirating strange bodies at adults can be remote by bronchoscope under local anaesthesia and even in ambulatory terms. However much the foreign bodies of respiratory tracts sometimes bring to the thoracoscopist unpleasant surprises, which force to apply the common anaesthetizing and hard instruments which require maximal concentration of forces and ability from him, and at times - inspiration. - Drainage of intrapulmonary festering hearths. Indisputable medical action of bronchoscopy, as a method of drainage of intrapulmonary festering hearths, is that bronchiectasis or lungs abscesses. Medical catheterization of bronchial tubes during bronchoscopy allows to deblock considerable part of intrapulmonary abscess formation cavities, and protracted transnasal drainage provides permanent introduction of antibacterial preparations to the cavity and releases patients from conducting of repeated bronchoscopies and 14 catheterizations. Method of immune-replacing therapy as intracavital introduction of autologic macrophages’ suspension, which does bronchoscopic medical treatment yet more effective was developed. The medical role of bronchoscopy at a chronic obstructive bronchitis (COB) was traditionally taken to renewal of respiratory tracts permeability with stimulation or imitation of the broken drainage function of bronchial tubes and local use of antibacterial and secretolytic facilities. After the first publications of A. Soulas and P. Mounier-Kuhn, that described the method of medical treatment of patients by the chronic unspecific diseases of lungs by bronchoscopy, the great number of different methods of the bronchoscopic medical treatment of COB was offered. Some of them were left, as those, which verifications by practice did not pass; other took the seat in the arsenal of remedies at patients with the diseases of the bronchopulmonary system. Bronchofibroscopy well recommended itself as effective manipulation treatment at violation of bronchial permeability at patients in an early postoperation period and, especially, at patients which need the protracted artificial ventilation of lungs (AVL). Flexible bronchofibroscope can be easily conducted in the respiratory tracts of patient through the intubation or tracheostomic tube, that allows to execute cleansing bronchoscopy at patients on AVL daily, and if necessary and on a few one times per a day. Except for the transferred enough ordinary situations which require the use of bronchoscopy, there is a row rarely the nascent pathological states at which bronchoscopy also can have the medical value. The special cases of destructive pneumonia belong to them, complicated pyopneumothrax. At some patients with this disease wide or plural bronchopleural fistulas does not only allow to straighten a lung after drainage of pleura cavity but also does not give successfully cleansing the cavity of pleura from penetration of lavage liquid in respiratory tracts. In a similar situation there is possibility to enter the obturator from foam or collagen sponge through bronchoscopy in proper segmental or lobar bronchus and temporally block it. It pressurizes a lung and halts the upcast of air through drainage. Terms for effective are thus created lavage pleura cavity and violence lungs. A similar blockade of bronchial tubes is possible on a term from a few days of to 2 weeks. For this time pleural enlargement have time to fix a lung in the straightened state, and shallow fistulas can be closed. Temporal occlusion of bronchial tubes with success is used and at large solitary abscesses the lungs, instrumental in reduction and obliteration of their cavity. 2. Endotracheal and endobronchial surgical interferences. Description of medical possibilities of bronchoscopy will be incomplete without mention about endotrachial and endobronchial surgical interferences. On the first pores they were executed by the current of high-frequency, and lately began mainly to use high-power YAG-lasers - neodymium and holmium. Using this technique, during bronchoscopy with success the of high quality tumours of trachea and large bronchial tubes are deleted, execute recanalization tracheas at it’s tumours, granulation and cicatricial stenosises. The last meet enough often, complicating continued intubation of trachea or tracheostomy at patients in the 15 departments of reanimation and intensive therapy. For the prophylaxis of repeated to the stenosing trachea after its recanalization by a laser, at peri-bronchial tumours which squeeze the road clearance of trachea or main bronchial tubes, and also at collapse of tracheas walls as a result of tracheomalacia use stetnts from silicon of a different construction - that fixed itself by appearances, Т- similar or Y- similar, bifurcation. Such stents-cross-bar can remain in education of trachea and main bronchial tubes during great while and provide free permeability of large respiratory tracts, in a number of cases allowing to do without tracheostomy. Contra-indication to bronchoscopy. Contra-indication to bronchoscopy, as a rule, is relative. To them belong the expressed respiratory insufficiency, cardiac arrhythmias, propensity to bronchial spasm, violation of ability to convolve to the blood, heavy intoxications. Is the question in these case there, mainly, about diagnostic researches. Wherein bronchoscopy is executed with a medical purpose, these contra-indications quite often depart on the second plan and after the congratulatory shows bronchoscopy can be justified at the heaviest patients. Complication of bronchoscopy With the increase of number and invasion of bronchoscopic methods and expansion of shows to them was multiplied the risk of procedure which in spite of megascopic level of the anaesthetic providing, as well as before from time to time is accompanied by enough serious complications. Their prophylaxis and medical treatment makes a separate and very vast problem which it is impossible to light up in the limited scopes of this review. The analysis of complications of bronchofibroscopy and so called hard or rigid bronchoscopy is conducted by us in the homogeneous groups of patients showed that "flexible" bronchoscopy, that is executed with a diagnostic purpose, on the whole was accompanied for certain by the less number of heavy complications, in particular, caused by diagnostic manipulations, because related to the less trauma of bronchial tubes and objects of biopsy. It allows to speak about greater safety of diagnostic bronchofibroscopy is comparative under local anaesthesia, that is especially important in ambulatory practice. To compare safety of medical bronchoscopic manipulations which are conducted by hard and flexible endoscopes, it is impossible, as indicators to their application, and consequently and weight of the state of patients, differentiate substantially. It follows only to underline that bronchofibroscopy, similarly as well as "hard" bronchoscopy, it is impossible to consider the absolutely safe method of research and medical treatment. This procedure requires from endoscopist ability not only to execute her in number of different ways and know endobronchial and pulmonary pathology but also be ready to development of different, sometimes heavy complications, requires certain knowledges and skills of reanimation, therapeutic and surgical character. Apartment, bronchoscopy, be that the special cabinet, or chamber of intensive therapy is executed in which, is to be accordingly equipped and equipped by all adaptations for conducting of successful reanimation or immediate medical treatment of any complication potentially possible at introduction of bronchoscopy and endobronchial manipulations with its help. 16 3. Videothoracoscopy. Presently there are two varieties of mini-invasive intra-thoracicf thoracoscope instruments enter in a pleura cavity through thoracic ports, and operations with video-accompaniment, when so called utilitarian mini-thoracotomy (5-6 sn), which is executed for deleting of fragment, that resected, at the end of thoracoscopic operation, execute at the beginning of interference, that allows to have the double review of the operated area and use traditional instruments. For denotation of such operations the term of «Video assisted» is used in English-language literature, and a new direction in thoracic surgery is named, accordingly, «video assisted thoracic surgery» (VATS). In Russian-language literature most widespread there is a term «intra-thoracic surgery with videoaccompaniment». Thoracoscopic operations and intra-thoracic interferences with video-accompaniment at the last 5-6 years more acquire everything to character of conservative, especially after such shows, as interstitial (disseminated) diseases of lungs and pleurisies not of clearing genesis, at which thoracoscopic biopsy allows to obtain verification of diagnosis in 100% of cases with the minimum number of complications. Торакоскопія at spontaneous pneumothorax allows to execute manipulations which will be realized during thoracotomy: resection, pleura abrasion or pleurectomy. Purpose of the use of videotechnologies at spontaneous pneumothorax foremost minimization of operating trauma, that conduces to reduction of postoperation pain, amounts of complications, terms of patients staying in hospital and more early returning of them to professional activity. At empyema of pleura with thoracoscopy, it is possible to remove a pus from encysted cavities, fibrin from parietal and visceral pleura under the visual control, to execute partial lungs decortication and pleurectomy. Last years thoracoscopy is used for empyema of hemithorax after pneumonectomy. Essence of method consists in sanation of cavity, deleting of fibrinous deposits, attempts of transthoracic occlusion of main bronchus stump fistula with the use of hernio-stapler. Thoracoscopy often appears by the optimum method of medical treatment at pathology of mediastinum, although manipulations in this area very difficult and tense through anatomic correlations and narrow field of examination. However, of high quality neo-formations of mediastinum, for example cysts, quite often are the shows to thoracoscopy. Thoracoscopic manipulations in the back departments of mediastinum include drainage of paravertebral abscessespuncture and deleting of bronchogenic cysts, ligation damaged pectoral lymphatic channel and deleting of neurogenic tumours. Most debatable and discutable role of thoracoscopy in diagnostics and medical treatment of cancer lungs. To execute lobectomy or pneumonectomy with video-accompaniment it follows only at patients which have sufficient functional backlogs, able to carry traditional operation, as it can necessary at any point. Successful executing of thoracoscopy in diagnostics and medical treatment of many diseases of organs of pectoral cavity resulted in more active use of this 17 method at the opened and closed trauma of breasts, and also at the consequences of operating trauma. Bandaging of pectoral lymphatic channel at postoperative chylothorax, medical treatment of postoperative bronchial fistulas, deleting from the pleura cavity of strange bodies and drainages which were torn off were described. A purview thoracoscopy is unreserved only by the transferred indications, and includes also interference concerning bronchiectasis, aneurism of internal pectoral artery, opened arterial channel, chyatal hernia, ventricular arrhythmias, relaxation of diaphragm. Indications: · Diseases of pleura: unspecific empyema of pleura. · Diseases of lungs: diseases of bulls, spontaneous pneumothorax, tuberculoma, of high quality tumours are lungs, solitary metastases, peripheral and central cancer the lungs in the stage of Т1М0 and Т2М0, bronchiectasises. · Diseases of pericardium: pericarditises, cysts of pericardium. · Diseases of mediastinum: thymoma, mediatinal cysts, tumours of mediastinum, chylothorax. · Diseases of gullet: achalasia of gullet, gastroesophageal reflux disease, leyomioma of gullet, shrines of gullet. · Diseases of diaphragm: relaxation of diaphragm cupola, diaphragmal hernia. · Trauma of thorax: haemothorax, strange bodies of pleural cavity. · Other indications: peptic ulcer, bronchial asthma, idiopathic hyperhidrosis of hands, axillary cavity and face, the Reyno’s disease, the Sudek’s dystrophy, disease of arterial occlusions, numero-antebrachial syndrome, migraine. Absolute contra-indications. Presence of rough pleura accretions, that appeared as a result of defeat or there were lungs in connection with impossibility of collapse as a result of previous surgical interference. Relative contra-indications. General somatic contra-indication (presence of concomitant pathology, that stipulates the high risk of conducting of anesthesia and surgical interference); prevalence of process, that causes doubting in possibility of implementation of necessary volume of operation by facilities of endoscopic surgery (endoscopic operation can be applied, but only on condition of providing of possibility of its conversion in the opened interference). Possible complications. General pulmonary-surgical intraoperation (traumatic, anaesthetic) and postoperation complications (festering-inflammatory, pleuro-pulmonary, discoagulation, cardiovascular and respiratory insufficiency, violation of bronchial permeability and atelectasises). General description. In the modern terms of thoracoscopic operation, as a rule, execute under intubal anesthesia with myorelaxants and artificial ventilation of lungs. Advantage gives oneself up to separate intubation in main bronchial tubes, although endotracheal intubation is used. However at implementation of diagnostic thoracoscopy with the small volume of surgical manipulations the intravenous can be used, anesthesia with mask in combination with local anaesthesia. In a number of cases the possible use especially of local anaesthesia. 18 Thoracocentesis is executed, depending on localization of pathology, in a point, that provides the optimum examination of pleural cavity (standard - in fifthsixth intercostal cavity on a middle, front or back axillary line). Thoracoscope is entered in pleura cavity, an examination is executed, the location for introduction of instrumental thoracoports is determined. Depending on the task of interference the common number of thoracoports can be from one to four-five. More frequent all three is used, which place, forming an isosceles triangle; subsequent ports are placed, coming a concrete topographical and technical situation from. If necessary survey and manipulation ports can be changed by places. At presence of pleura accretions they are destroyed, pleura perspiration (at presence of) is deleted, the examination of parietal pleura is farther conducted, structures of mediastinum, visceral pleura and lungs. The presence of pathological process is estimated, its character, prevalence, a biopsy is executed in the places of pathological changes. Minithoracotomy is additionally executed if necessary. Farther is surgical interference (regional resection the lungs at a disseminated process, coagulation, sewing or deleting of bullous fragments lungs at bullous emphysema, resection the lungs with a solitary new formation et cetera). Operation is closed, as well as thoracotomy is opened, by drainage of pleura cavity. Thus, now thoracoscopic interference is justly examined how alternative traditional thoracotomy. Advantages of these minimum injuring operative methods consist in the best review of the operated area, noticeable reduction of number of postoperative complications, less sickliness, early postoperative activity and brief stay of patients in hospital. Laser destruction Indicationsy to conducting of endoscopic laser destruction: 1. Presence of complete or partial tumour obturation of tracheobronchial tree with hypoventilation, by obtural pneumonia, by atelectasis of appropriate departments of lungs. 2. Presence of endobronchial component of tumour at patients which are subject to the special methods of medical treatment. 3. Endobronchial relapse of crawfish after surgical medical treatment or radial therapy. 4. Presence of high quality tumour in a tracheobronchial trunk. Endoscopic laser destruction is the effective and safe method of medical treatment of new formations of tracheobronchial tree. Efficiency of endoscopic laser recanalization malignant neoplasms depends on localization, character of growth and expressed of tumour stenosis: most - at the endobronchial tumours of trachea and main bronchial tubes, that partly stenosing, substantially below - at tumours of bronchial tubes of less caliber, and also in case of complete stenosis regardless of localization of tumour in a bronchial tree. The use of tumour’s endoscopic laser destruction as component of medical treatment of malignant neoplasms of trachea and bronchial tubes is the effective mean of optimization of terms of conducting of surgical interference, as a result of reduction of tumour’s mass, removal of bronchial obstruction, related to its respiratory insufficiency and concomitant inflammatory phenomena. 19 The endoscopic laser destruction executed with the purpose of removal of stenosis of tracheobronchial tree can be the method of choice in palliative medical treatment of інкурабельних patients with the malignant tumours of trachea and bronchial tubes, that stenosing, and is the instrumental method in the improvement of quality of life of patients. Endoscopic laser destruction is the effective method of medical treatment of high quality neoplasms of tracheobronchial tree. In default of intramural and allowed the exobronchial component of tumours of the use of method to obtain the radical deleting of tumour in 100% of patients. Medical treatment of cardiovascular diseases Intervention methods Indications to the intervention methods of medical treatment of chronic IHD: - Angina pectoris of the ФК III-IV tension. - Carried to them in anamnesis even without the clinic of angina pectoris. - Stenosis of the left coronary artery trunk more than 50% even without the clinic of angina pectoris (very often at once begins from vast by HIM - The right coronary artery stenosises more than 30% at patients with the clinic of angina pectoris of any functional class. Coronary bulb angioplasty • Gruentzig A. firstly executed it in 1977. • Principle: a bulb dilatation catheter is entered in a coronary artery, under the control a screen a bulb is brought into the place of stenosis, whereupon pressure in a bulb is to 6-8-10 atmospheres during 3 minutes, a name-plate is squashed as a result. Upon termination of procedure obligatory to measuring of pressure in an artery below than stenosis and control coronarography. The angiographic criterion of success is reduction of measure of stenosis more than on 20%. Often bulb dilatation is concluded by vessels stenting (stents 2-4,5 mm). 24 hours prior to manipulation a patient begins to adopt antiagregants, in the moment of angioplasty conducting intracoronary enter heparin and nitroglycerine. • Angioplasty is conducted at the unfolded cardiovascular operating-room and at permanent ECG monitoring (complication is acute occlusion of artery, stratification of intima, acute myocardial ischemia). • New technologies of angioplasty: laser recanalization - by the «cold» laser radiation (on the end of light-wire) a channel is done in education of occlusing artery, bulb angioplasty is farther produced. • Indications to angioplasty: single stenosises of any of coronary arteries (except for the basic trunk of left coronary artery), single stenosises no more than 2 coronary arteries, plural stenosises in one coronary artery, chronic occlusion by a remoteness less than 3 months and slowness no more than 2 sm. • Lethality - 1,2%, nearest positive result - in 90%, during 1st in 40% arise up re-stenosises. Frequency of complications which require urgent operation - not higher 6%. Surgical medical treatment (aortocoronary shunting and mammarocoronary shunting) 20 • Aortocoronary shunting first executed Michael Ellis DeBakey in 1964, and mammarocoronary shunting – V.I. Kolesov also in 1964. • Indications: stenosis of the basic trunk of left coronary artery (even at ejection fraction < 40%), stenosises or occlusions more than 2 coronary arteries, plural stenosises of coronary arteries. • Basic principles: operation is conducted only in the glucose-insulinpotassium mixture terms on a «dry heart», it is better with the use of optics (increase in 2-4 times); all arteries which have haemodinamically meaningful stenosis (one-momently it is possible to shunt no more than 7 arteries by a diameter more 1mm) are shunted, however with an aorta no more than 4 anastomosises are imposed, at first shunt anterior interventricular artery, then rounding artery and right coronary artery; coronary anastomosises are usually imposed at first, then are aortic (Yu.V. Belov - in a reverse sequence); during operation execute the control of function of shunt by fluometer (blood stream on a shunt - not below 50 ml/min). Imposition is presently considered optimum no more than 4 shunts. • The heavy defeat of distal river-bed and ejection fraction of left ventricle is contra-indications to aortocoronary shunting < 40%. • After aortocoronary shunting because of high risk of development of acute cardiac insufficiency (especially at patients with ejection fraction < 50%) are to be foreseen trans-aortal bulb contra-pulsation, or artificial left ventricle. Results and prognosis after aortocoronary shunting (mammarocoronary shunting) • Lethality after aortocoronary shunting - 5,7%; at persons junior 75 years 1,4%, at patients with angina pectoris without silent myocardial infarction in anamnesis - 0,5%. • Five-year survivability after aortocoronary shunting - 96%, at conservative medical treatment of that category of patients - 60%. Frequency of silent myocardial infarction after aortocoronary shunting - 1% in a year, without aortocoronary shunting > 3%. • During 1st permeability of aortocoronary shunting is kept in 80% of patients, then frequency of occlusion of shunts - 2% in a year, and in 5 years - 5% in a year. Results it is better after mammarocoronary shunting (therefore aortocoronary shunting and mammarocoronary shunting combines presently). At women the results it is worse in 2,5 times. • At the defeat of 1 coronary artery (eliminating the left coronary artery trunk) the aortocoronary shunting results comparable with the results of conservative therapy. At the defeat 2 and more coronary artery at angina pectoris of functional class I-II surgical medical treatment improves quality of life, deprives a patient from the attacks of angina pectoris and permanent reception of antianginal preparations, substantially not influencing on remote survivability. At functional class III-IV aortocoronary shunting as surgical medical treatment increases and remotes survivability. 21 Transmiocardial and endomiocardial laser revascularization. • Principle: by a «cold» laser of 30-60 small channels is created in myocardium either transmiocardially (on a working heart) or endomiocardially (by a catheter). • It is the aortocoronary shunting alternative at patients with the heavy defeat of distal river-bed and low faction of the troop landing. Medical tactic. • Conservative medical treatment such as well as at unstable angina pectoris. Obligatory – adrenoblockers and antagonists of calcium (the area of ischemia is abbreviated), adequate anaesthetizing by narcotic analgetics. At development of cardiogenic shock - ТАБК. Period of finding in the separation of intensive therapy - 10 days (danger of development of heavy complications). • Urgent intra-coronary fibrinolytic and anti-thrombotic therapy with subsequent bulb angioplasty effective if no more than 6 hours passed from the moment of myocardial infarction. 6. Materials of the methodological providing of lesson. 6.1 Task for self-control. А. Questions for self-control 1. Describe the basic methods of research of organs of pectoral cavity. 2. Name the basic methods of research of the cardiac system. 3. Name the basic methods of medical treatment of lungs. 4. Transfer the intervention methods of medical treatment of heart. 5. Methods of surgical medical treatment of diseases of the cardiovascular system. B. Tests for self-control Which from the transferred methods of research of patient with suspicion on myocardial infarction it is necessary to execute above all things: А. ECG B. Roentgenogram of pectoral cavity organs C. Echocardioscopy D. Coronarography E. КТ of pectoral cavity organs Right answer - A. В. Tasks for self-control Patient К., 27 years entered with complaints about acute pain in a left half pectoral cavity, complicated breathing, palpitation. Pulse of 96 blows/min, arterial pressure 110/70 mm of m.p, breathing frequency 24/min. Auscultative: to the right breathing is hearkened on all draught, on the left is acutely weakened. Roentgenogram: - collapsed left lung, shade of mediastinum is on right side displaced. Diagnosis: left-side pneumothorax. What your medical tactic? А. Drainage of left pleura cavity. B. Thoracotomy. C. Pleural puncture. 22 D. Conservative medical treatment. E. Bronchoscopy. 6.2. Literature Basic: 1. Факультетська хірургія / За ред. В.О. Шідловського, М.П. Захараша. – Тернопіль : Укрмедкніга, 2002. - С. 349-356, 363-371. 2. Хірургічні хвороби / Под ред. М.І. Кузіна. - М. : Медицина, 1995. - С. 38-60. 3. Хірургічні маніпуляції / Під ред. Б.О. Мількова, В.Н. Круцяка. - К. : Вища школа, 1985. - 208 с. 4. Сулимов В. А., Маколкин В. И. Чреспищеводная электрическая стимуляция сердца. – M. : Медицина, 2001. 5. Рычков А. Ю. Показания к проведению чреспищеводного электрофизиологического исследования // Вестник аритмологии. – 2001. - № 20. 6. Шпитальна хірургія : Руководство / Ковальчук Л. Я. и др. – Тернопіль : Укрмедкнига, 1999. – 590 с. 7. Сердечно-сосудистая хирургия : Руководство / Бураковский В. И., Бокерия Л. А. - М. : Медицина, 1989. – 752 с. Additional: 1. Белоконь Н. А. Врожденные пороки сердца. - М., 1990. – 352 с. 2. Амосов Н. М., Бендет Я. А. Терапевтические аспекты кардиохирургии. - К. : Здоров’я, 1990. – 296 с. 3. Сулимов В. А., Маколкин В. И. Чреспищеводная электрическая стимуляция сердца. – М. : Медицина, 2001. 4. Рычков А. Ю. Показания к проведению чреспищеводного электрофизиологического исследования // Вестник аритмологии. – 2000. - № 20. 7. List of educational practical tasks which it is necessary to execute during practical lesson 1. Correct reading of roentgenogram of thorax. 2. Faithful interpretation of ECG in relation to recognition of acute myocardial infarction 3. Method of pleural puncture and drainage of pleural cavity. 23 Tests for self-control Which from the transferred methods of research of patient with suspicion on myocardial infarction it is necessary to execute above all things: А. ECG B. Roentgenogram of pectoral cavity organs C. Echocardioscopy D. Coronarography E. КТ of pectoral cavity organs Right answer - A. The methodological instructive elaboration is made by associated professor Martynuyk V.A.