Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Online Appendix for the following February 20 JACC article
TITLE: Endothelial Progenitor Cells in Cardiovascular Disorders
AUTHORS: Eduard Shantsila, MD, Haemostasis, Thrombosis & Vascular Biology Unit,
University Department of Medicine, City Hospital, Birmingham, United Kingdom, Timothy
Watson, MRCP, Haemostasis, Thrombosis & Vascular Biology Unit, University Department
of Medicine, City Hospital, Birmingham, United Kingdom, Gregory Y.H. Lip, MD, FRCP,
Haemostasis, Thrombosis & Vascular Biology Unit, University Department of Medicine, City
Hospital, Birmingham, United Kingdom
APPENDIX
SEARCH STRATEGY
We performed a comprehensive literature search using electronic bibliographic databases (i.e.,
MEDLINE, EMBASE, DARE, COCHRANE DATABASE), scanning reference lists from
included articles and hand searching abstracts from national and international cardiovascular
meetings. For the search, we used the term “endothelial progenitor cell(s).” Bibliographies of
all selected articles and review articles were reviewed for other relevant articles. Finally, the
supplements of major journals were hand searched to identify relevant abstracts that had not
been published as peer-reviewed articles. Where necessary, study authors were contacted to
obtain further data.
ENDOTHELIAL PROGENITOR CELLS: PATHOPHYSIOLOGICAL
CONSIDERATIONS—DEFINITION AND LINKS TO ANGIOGENESIS
Endothelial Markers
In 1997, Asahara et al. (1) first reported the isolation of endothelial precursor cells (EPCs)
from peripheral blood because they had found that CD34+ hematopoietic progenitor cells can
differentiate to cells with endothelial characteristics. The EPCs were defined as cells positive
for both hematopoietic stem cell and endothelial cell markers, such as CD34 and vascular
endothelial growth factor (VEGF) receptor-2, respectively. The latter VEGF receptor-2 is
often referred to as kinase insert domain receptor (KDR).
The putative CD34+ EPC is able to proliferate and differentiate to mature endothelial cells
with expression of different endothelial markers (Figure) such as KDR (2,3), plateletendothelial cell adhesion molecule (CD31) (2,4), von Willebrand factor (2,3,5), VE-cadherin
(2,3), caveolin-1 (4,6), and endothelial nitric oxide synthase (4,6). While in vitro, EPCs can
form vascular-like structures (3,6), and in vivo, incorporate into neovessels at sites of tissue
ischemia (3,5,7). Of note, CD34 antigen density is highest on early progenitors and decreases
progressively as cells mature (8); however, CD34 is expressed not only on EPCs but on
mature endothelial cells, albeit at a lower density (9). Therefore, an early hematopoietic stem
cells marker, CD133, was adopted as an alternative additional marker to indicate a “true” EPC
(10,12).
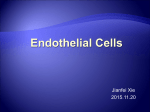
FIGURE
Potential Origin and Differentiation of Endothelial Progenitor Cells
BONE MARROW
Hematopoietic stem cells
CD34+ CD133++ CD45+
Mesenchymal stem
cells CD34- c-kit-
Side population
cells
Myeloid Precursors
CD14+ CD45+
Tissue-resident
stem cells
c-kit+
“Early” EPCs
CD34++ CD133++
KDR+
Macrophages
Monocytes
“More mature” EPCs
+
+
++
CD14
+
CD14+++ CD45+
CD45
+
CD34 CD133 KDR
BLOOD VESSEL
Mature EPCs
CD133- CD34low
KDR+ CD31+
VE-Cadherin+
vWF+
Are these cells the same?
The marker CD133 (also known as prominin or AC133) is a 120-kDa transmembrane
polypeptide with an (as yet) unknown biological function. It is expressed on hematopoietic
stem and progenitor cells from human bone marrow, fetal liver, and peripheral blood (11). As
progenitors develop to more mature endothelium-like cells, CD133 is rapidly downregulated
(10). The CD133+ cells are able to form both early and late outgrowing colonies in vitro (10).
Thus, CD133 might provide a more reliable means of defining and tracking human
angioblast-like EPCs and distinguishing these from mature endothelial or monocytic cells.
The combination of CD34, CD133, and KDR is commonly used for this purpose, and this
represents a rare subset of peripheral blood cells. Interestingly, the CD34−/133+
subpopulation of endothelial progenitors was recently found to be a possible precursor of
classic CD34+/133+ EPCs, but to possess even more potent angioregenerative properties in
vivo than on the latter (13).
Hematopoietic Markers
Hematopoietic
cell
markers
such
as
CD34,
CD133,
and
CD117
(c-kit)
and
monocytic/macrophagic cell markers such as CD11 and CD14 are expressed by early
immature EPCs, and are subsequently lost in the more differentiated state (10,11).
Paradoxically, expression of endothelial markers progressively increases with EPC maturation
(3). Subtypes of these cells that do not express VE-cadherin and von Willebrand factor seem
to be an early subpopulation of EPCs localized predominantly in the bone marrow or detected
immediately after their migration into the systemic circulation (14). More mature circulating
CD34-positive EPCs also present CD31, CD146, VE-cadherin, and endothelial nitric oxide
synthase, as well as begin to express von Willebrand factor (10,11). Thus, the surface marker
profile of EPCs seems to depend predominantly on their stage of differentiation (15). The
current most detailed phenotypic description of circulating EPCs proposes the co-expression
of several common hematopoietic and endothelial antigens: CD34, CD133, CD31, CD38,
CD45, KDR, VE-cadherin, c-kit, and Flt-1 (16).
Cultivation of peripheral blood mononuclear cells (MNCs) in medium favoring endothelial
growth is another approach widely used for definition and quantitative analysis of EPCs.
Adherent cells grow colonies and have been shown to possess endothelial characteristics, such
as expression of von Willebrand factor and staining for Dil-acetylated low-density lipoprotein
and Fluorescein isothiocyanate (FITC)-conjugated BS-lectin (17–20). Despite the relatively
low numbers of CD34+ of circulating endothelial precursors in peripheral blood (100 to
500/ml), relatively large numbers of adherent cells are found during culture (approximately
100,000 from 1 mL blood). This raises some controversy with respect to the identification and
the origin of isolated EPCs, as these cells seem to reflect a functional subpopulation within
the blood MNCs that have the potential to differentiate into an endothelial phenotype in vivo
(18,21–23,24).
There are at least 2 morphologically and functionally distinct endothelial cell populations can
be grown from circulating MNCs (2). The early spindle-like outgrowth cells possess a
relatively low proliferative capacity and low ability to express mature endothelial proteins (3).
These cells presumably represent cells of different lineage, which include a subset of
CD14+/CD34− monocytic cells, which have the potential to differentiate (transdifferentiate)
into endothelial-like cells under certain environmental condition in the presence of special
growth factors (e.g., VEGF, fibroblast growth factor, and so on) (22). Late “outgrowth cells”
show a high proliferative potential and originate predominantly from bone marrow donors and
are considered as circulating angioblasts (2).
It is important to appreciate that although monocyte-derived EPCs have a lower in vitro
proliferation potential than hematopoietic stem cells or cord-blood-derived EPCs (25), the
different progenitor types seem to have a similar ability to enhance neovascularization in
experimental models (3,26,27). One may speculate that proliferation capacity is not the
decisive factor and that the reduced proliferation of the monocyte-derived EPCs is likely to be
attributable to increased release of growth factors, which may act in a paracrine manner to
support angiogenesis and arteriogenesis (28).
The expression of common markers by hematopoietic and endothelial progenitor cells in
embryonic development and transdifferentiation potential of monocytes into cells with
endothelial characteristics would suggest a possible common origin from a bone marrow
precursor, perhaps a putative hemangioblast (29). Bone marrow also contains mesenchymal
cells, which have been shown to differentiate into endothelial cells (30), improve
vascularization in vivo (31,32), and contribute to tissue repair (33). Likewise, other bonemarrow-derived EPCs mesenchymal stem cells release a variety of angiogenic growth factors
(34). In addition to bone-marrow-derived cells, other cell populations, such as fat tissue
(35,36), cardiac tissue (37), neural stem cells (38), and fetal liver cells (39), can give rise to
endothelial cells, suggesting that tissue-resident stem/progenitor cells can contribute to
vascular growth in the adult.
In summary, a universal single or complex EPC marker still remains to be identified, showing
the heterogeneous nature of endothelial precursors. As a result, both different surface markers
and culture properties have been used by research workers to define EPCs.
ANGIOGENIC CYTOKINES AND CHEMOKINES: THE LINK TO EPCs
EPCs have been linked to angiogenic cytokines and chemokines. For example, VEGF is one
of the key angiogenic factors involved in the earliest stages of vasculogenesis and
angiogenesis (40–42), and is the primary determinant of hemangioblast differentiation into
angioblasts (EPCs) and hematopoietic stem cells (43). Asahara et al. first showed the effects
of VEGF on adult endothelial progenitors, which included enhanced EPC mobilization from
bone marrow, proliferation, differentiation, and incorporation of bone-marrow-derived EPCs
into the neovasculature (44). This physiological pathway may be another target of
cardiovascular risk factors, such as oxidized low-density lipoprotein; the latter inhibits VEGFinduced EPC differentiation (45). For patients with inoperable CAD (46) or critical limb
ischemia (47), VEGF gene transfer results in mobilization of EPCs, which could potentially
be involved in the success of such therapy (46). Interestingly, the dose of EPCs required to
obtain clinical improvement in murine hind limb ischemia reduced by as much as 30-fold
when VEGF gene transfer was simultaneously used (48). Furthermore, combination of VEGF
gene therapy with cytokine (granulocyte colony-stimulating factor [G-CSF] and stem cell
factor) administration led to enhanced neovascularization, bone marrow cell mobilization, and
incorporation into the neovasculature, as well as improvements in cardiac performance, at
least in animal models of cardiac ischemia (49).
However, intramyocardial injection of VEGF-A plasmid followed by G-CSF in patients with
severe chronic ischemic heart disease failed to induce angiogenesis, as well as to show any
improvement in cardiac perfusion or function (50). This might be explained partly by the low
VEGF-A165 plasmid dose chosen (probably for safety reasons) because no significant
increase in CD34+ cells was observed. In another rodent study, VEGF gene transfer was
associated with enhanced angiogenesis and mobilization of bone marrow cells and the
recruitment of cultured MNCs to the sites of neovascularization (51).
Both G-CSF and granulocyte-macrophage colony-stimulating factor, which are already
widely used clinically in oncology and in transplant donors, were considered attractive
candidates for stimulating arteriogenesis. Pre-clinical studies uniformly report positive results
of their infusion alone (52) or in combination with bone marrow MNC transplantation (53) or
cytokines to mobilize EPCs in different models of ischemia (54–56). However, 3 clinical
trials of G-CSF and granulocyte-macrophage colony-stimulating factor treatment to stimulate
neovasculogenesis were stopped early because of serious safety concerns (57–59). For
example, the MAGIC cell-randomized clinical trial of intracoronary administration of
peripheral blood leucocytes with subcutaneous infusion of G-CSF in patients after myocardial
infarction was stopped because of a high rate of in-stent restenosis despite good
periprocedural results and short-term safety (59). In the study by Zbinden et al. (57), an acute
occlusion of a coronary artery developed in 2 of 7 patients with stable angina undergoing
percutaneous coronary intervention within 12 days of treatment with granulocyte-macrophage
colony-stimulating factor. In the study by Hill et al. (58), G-CSF increased the number of
circulating CD34+/CD133+ progenitors in patients with severe CAD, but also increased Creactive protein levels and white cell counts. At 1 month after treatment, there was no
improvement in either cardiac contractility or exercise duration, and a trend toward a greater
number of ischemic segments was seen. Worryingly, 2 of 16 patients included in the study
experienced myocardial infarction, which was fatal in 1 patient.
Although in 1 study, treatment with G-CSF in patients with myocardial infarction subjected to
primary PCI stenting with abciximab not only mediated mobilization of CD34+ progenitors,
but significantly improved left ventricular function and geometry without signs of accelerated
restenosis or other serious complications (60), it was proposed to restrict ongoing trials using
G-CSF or granulocyte-macrophage colony-stimulating factor to patients with no other
therapeutic options, such as those with refractory angina or critical limb ischemia (61). The
mechanisms of the reported complications are unclear, but may relate to the proinflammatory
and procoagulant effects of G-CSF (62), possibly leading to vascular smooth muscle cell
proliferation. Indeed, recently G-CSF was shown to induce neointimal overgrowth in a rabbit
iliac artery balloon injury model after bare-metal stenting, possibly as a result of concomitant
mobilization of smooth muscle progenitors. Implantation of paclitaxel-eluting stents
substantially reduced neointimal overgrowth, probably by preferential inhibition of
proliferation of smooth muscle lineage cells rather than EPCs, and G-CSF treatment in this
group significantly accelerated endothelial recovery (63). A further clinical trial by
Zohlnhufer et al. (64) has failed to reignite interest in the potential of G-CSF to induce
neoangiogenesis. In this study, a cohort of patients with acute myocardial infarction
undergoing percutaneous coronary intervention within 12 h of symptom onset were
randomized to a 5-day course of G-CSF or placebo. The CD34 cell counts were quantified by
flow cytometry up to 1 week after randomization. Although CD34+ cells did increase in the
G-CSF group, there was notably no difference in infarct size as assessed by technetium
Tc99m sestamibi scintigraphy 4 to 6 months compared with baseline. Importantly though, the
previously noted excess of restenosis did not feature strongly in this study.
A positive impact on the EPC characteristics and potential proangiogenic properties has been
shown in the experimental studies for a number of cytokines/chemokines such as stromal cellderived factor-1-alpha (65), stem cell factor (55), hepatocyte grow factor (66), transforming
growth factor-beta1 (67), hemangiopoietin (68), and secretoneurin (69). For example, stromal
cell-derived factor-1alpha was shown to play an important role in the mobilization of
CD34+CXCR4+ progenitor cells during cardioplegia and cardiopulmonary bypass (70).
Members of the platelet-derived growth factor (PDGF) family are involved in vascular
physiology, and may be possible promoters of angiogenesis. Secreted by ECs, PDGF-BB
plays an important role in the maturation of blood vessels via recruiting mural cells (71), as
well as in the promotion of angiogenesis indirectly by producing VEGF (72). Also, PDGF-BB
was shown to induce differentiation of bone marrow EPCs into smooth muscle cells (73).
When administered alone, PDGF-BB reduces EC survival and causes destabilization of
vessels as a result of impaired mural cell coverage. Both PDGF-BB and PDGF-AB show
positive vascular effects only when coadministered with other cytokines or bone marrow cells
(73–75). Recently, Li et al. (76) showed multiple proangiogenic properties of PDGF-CC, a
novel member of PDGF family: mobilization, differentiation of EPCs and their homing to the
sites of ischemia, migration of mature endothelial cells and microvessel sprouting, and release
of VEGF. Moreover, PDGF-CC can induce differentiation of progenitors into endothelial
cells and smooth-muscle cells, which represent another essential component of blood vessels
(76). Given its multiple angiogenic actions, PDGF-CC is considered to be an attractive
candidate for combination therapy with other growth factors (77).
REFERENCES
1. Asahara T, Murohara T, Sullivan A, et al. Isolation of putative progenitor endothelial cells
for angiogenesis. Science 1997;275:964–7.
2. Lin Y, Weisdorf DJ, Solovey A, Hebbel RP. Origins of circulating endothelial cells and
endothelial outgrowth from blood. J Clin Invest 2000;105:71–7.
3. Hur J, Yoon CH, Kim HS, et al. Characterization of two types of endothelial progenitor
cells and their different contributions to neovasculogenesis. Arterioscler Thromb Vasc Biol
2004;24:288–93.
4. Gulati R, Jevremovic D, Peterson TE, et al. Autologous culture-modified mononuclear cells
confer vascular protection after arterial injury. Circulation 2003;108:1520–6.
5. Shi Q, Rafii S, Wu MH, et al. Evidence for circulating bone marrow-derived endothelial
cells. Blood 1998;92:362–7.
6. Gulati R, Jevremovic D, Peterson TE, et al. Diverse origin and function of cells with
endothelial phenotype obtained from adult human blood. Circ Res 2003;93:1023–5.
7. Zhang ZG, Zhang L, Jiang Q, Chopp M. Bone marrow–derived endothelial progenitor cells
participate in cerebral neovascularization after focal cerebral ischemia in the adult mouse.
Circ Res 2002;90:284–8.
8. Civin CI, Banquerigo ML, Strauss LC, Loken MR. Antigenic analysis of hematopoiesis.
VI. Flow cytometric characterization of My-10 positive progenitor cells in normal human
bone marrow. Exp Hematol 1987;15:10–7.
9. Fina L, Molgaard HV, Robertson D, et al. Expression of the CD34 gene in vascular
endothelial cells. Blood 1990;75:2417–26.
10. Peichev M, Naiyer AJ, Pereira D, et al. Expression of VEGFR-2 and AC133 by
circulating human CD34 (+) cells identifies a population of functional endothelial precursors.
Blood 2000;95:952–8.
11. Yin AH, Miraglia S, Zanjani ED, et al. AC133, a novel marker for human hematopoietic
stem and progenitor cells. Blood 1997;90:5002–12.
12. Miraglia S, Godfrey W, Yin AH, et al. A novel five-transmembrane hematopoietic stem
cell antigen: isolation, characterization, and molecular cloning. Blood 1997;90:5013–21.
13. Friedrich EB, Walenta K, Scharlau J, Nickenig G, Werner N. CD34−/CD133+/VEGFR2+ endothelial progenitor cell subpopulation with potent vasoregenerative capacities. Circ Res
2006;98:e20–5.
14. Quirici N, Soligo D, Caneva L, Servida F, Bossolasco P, Deliliers GL. Differentiation and
expansion of endothelial cells from human bone marrow CD133+ cells. Br J Haematol
2001;115:186–94.
15. Murohara T, Ikeda H, Duan J, et al. Transplanted cord blood-derived endothelial
precursor cells augment postnatal neovascularization. J Clin Invest 2000;105:1527–36.
16. Burger PE, Coetzee S, McKeehan WL, et al. Fibroblast growth factor receptor-1 is
expressed by endothelial progenitor cells. Blood 2002;100:3527–35.
17. Shintani S, Murohara T, Ikeda H, et al. Mobilization of endothelial progenitor cells in
patients with acute myocardial infarction. Circulation 2001;103:2776–9.
18. Hill JM, Zalos G, Halcox JP, et al. Circulating endothelial progenitor cells, vascular
function, and cardiovascular risk. N Engl J Med 2003;348:593–600.
19. Vasa M, Fichtlscherer S, Adler K, et al. Increase in circulating endothelial progenitor cells
by statin therapy in patients with stable coronary artery disease. Circulation 2001;103:2885–
90.
20. Vasa M, Fichtlscherer S, Aicher A, et al. Number and migratory activity of circulating
endothelial progenitor cells inversely correlate with risk factors for coronary artery disease.
Circ Res 2001;89:E1–7.
21. Fernandez Pujol B, Lucibello FC, Gehling UM, et al. Endothelial-like cells derived from
human CD14 positive monocytes. Differentiation 2000;65:287–300.
22. Harraz M, Jiao C, Hanlon HD, Hartley RS, Schatteman GC. CD34(-) blood-derived
human endothelial cell progenitors. Stem Cells 2001;19:304–12.
23. Schmeisser A, Garlichs CD, Zhang H, et al. Monocytes coexpress endothelial and
macrophagocytic lineage markers and form cord-like structures in Matrigel under angiogenic
conditions. Cardiovasc Res 2001;49:671–80.
24. Rookmaaker MB, Vergeer M, van Zonneveld AJ, Rabelink TJ, Verhaar MC. Endothelial
progenitor cells: mainly derived from the monocyte/macrophage containing CD34- but also
partly derived from the hematopoietic stem cell containing CD34+ mononuclear population.
Circulation 2003;108:150e.
25. Ingram DA, Mead LE, Tanaka H, et al. Identification of a novel hierarchy of endothelial
progenitor cells utilizing human peripheral and umbilical cord blood. Blood 2004;104:2752–
60.
26. Urbich C, Heeschen C, Aicher A, Dernbach E, Zeiher AM, Dimmeler S. Relevance of
monocytic features for neovascularization capacity of circulating endothelial progenitor cells.
Circulation 2003;108:2511–6.
27. Kalka C, Masuda H, Takahashi T, et al. Transplantation of ex vivo expanded endothelial
progenitor cells for therapeutic neovascularization. Proc Natl Acad Sci U S A 2000;97:3422–
7.
28. Urbich C, Dimmeler S. Endothelial progenitor cells: functional characterization. Trends
Cardiovasc Med 2004;14:318–22.
29. Nishikawa SI. A complex linkage in the developmental pathway of endothelial and
hematopoietic cells. Curr Opin Cell Biol 2001;13:673–8.
30. Oswald J, Boxberger S, Jorgensen B, et al. Mesenchymal stem cells can be differentiated
into endothelial cells in vitro. Stem Cells 2004;22:377–84.
31. Reyes M, Dudek A, Jahagirdar B, Koodie L, Marker PH, Verfaillie CM. Origin of
endothelial progenitors in human postnatal bone marrow. J Clin Invest 2002;109:337–46.
32. Al-Khaldi A, Eliopoulos N, Martineau D, Lejeune L, Lachapelle K, Galipeau J. Postnatal
bone marrow stromal cells elicit a potent VEGF-dependent neoangiogenic response in vivo.
Gene Ther 2003;10:621–9.
33. Kuznetsov SA, Mankani MH, Gronthos S, Satomura K, Bianco P, Robey PG. Circulating
skeletal stem cells. J Cell Biol 2001;153:1133–40.
34. Kinnaird T, Stabile E, Burnett MS, et al. Local delivery of marrow-derived stromal cells
augments collateral perfusion through paracrine mechanisms. Circulation 2004;109:1543–9.
35. Zuk PA, Zhu M, Mizuno H, et al. Multilineage cells from human adipose tissue:
implications for cell-based therapies. Tissue Eng 2001;7:211–28.
36. Planat-Benard V, Silvestre JS, Cousin B, et al. Plasticity of human adipose lineage cells
toward
endothelial
cells:
physiological
and
therapeutic
perspectives.
Circulation
2004;109:656–63.
37. Beltrami AP, Barlucchi L, Torella D, et al. Adult cardiac stem cells are multipotent and
support myocardial regeneration. Cell 2003;114:763–76.
38. Wurmser AE, Nakashima K, Summers RG, et al. Cell fusion-independent differentiation
of neural stem cells to the endothelial lineage. Nature 2004;430:350–6.
39. Dan YY, Riehle KJ, Lazaro C, et al. Isolation of multipotent progenitor cells from human
fetal liver capable of differentiating into liver and mesenchymal lineages. Proc Natl Acad Sci
U S A 2006;103:9912–7.
40. Shalaby F, Rossant J, Yamaguchi TP, et al. Failure of blood-island formation and
vasculogenesis in Flk-1-deficient mice. Nature 1995;376:62–6.
41. Carmeliet P, Ferreira V, Breier G, et al. Abnormal blood vessel development and lethality
in embryos lacking a single VEGF allele. Nature 1996;380:435–9.
42. Coultas L, Chawengsaksophak K, Rossant J. Endothelial cells and VEGF in vascular
development. Nature 2005;438:937–45.
43. Wilting J, Brand-Saberi B, Kurz H, Christ B. Development of the embryonic vascular
system. Cell Mol Biol Res 1995;41:219–32.
44. Asahara T, Takahashi T, Masuda H, et al. VEGF contributes to postnatal
neovascularization by mobilizing bone marrow-derived endothelial progenitor cells. EMBO J
1999;18:3964–72.
45. Imanishi T, Hano T, Matsuo Y, Nishio I. Oxidized low-density lipoprotein inhibits
vascular endothelial growth factor-induced endothelial progenitor cell differentiation. Clin
Exp Pharmacol Physiol 2003;30:665–70.
46. Kalka C, Tehrani H, Laudenberg B, et al. VEGF gene transfer mobilizes endothelial
progenitor cells in patients with inoperable coronary disease. Ann Thorac Surg 2000;70:829–
34.
47. Kalka C, Masuda H, Takahashi T, et al. Vascular endothelial growth factor (165) gene
transfer augments circulating endothelial progenitor cells in human subjects. Circ Res
2000;86:1198–202.
48. Iwaguro H, Yamaguchi J, Kalka C, et al. Endothelial progenitor cell vascular endothelial
growth factor gene transfer for vascular regeneration. Circulation 2002;105:732–8.
49. Kawamoto A, Murayama T, Kusano K, et al. Synergistic effect of bone marrow
mobilization and vascular endothelial growth factor-2 gene therapy in myocardial ischemia.
Circulation 2004;110:1398–405.
50. Ripa RS, Wang Y, Jorgensen E, Johnsen HE, Hesse B, Kastrup J. Intramyocardial
injection of vascular endothelial growth factor-A165 plasmid followed by granulocyte-colony
stimulating factor to induce angiogenesis in patients with severe chronic ischaemic heart
disease. Eur Heart J 2006;27:1785–92.
51. Zentilin L, Tafuro S, Zacchigna S, et al. Bone marrow mononuclear cells are recruited to
the sites of VEGF-induced neovascularization but are not incorporated into the newly formed
vessels. Blood 2006;107:3546–54.
52. Cho HJ, Kim HS, Lee MM, et al. Mobilized endothelial progenitor cells by granulocytemacrophage colony-stimulating factor accelerate reendothelialization and reduce vascular
inflammation after intravascular radiation. Circulation 2003;108:2918–25.
53. Takagi Y, Omura T, Yoshiyama M, et al. Granulocyte-colony stimulating factor augments
neovascularization induced by bone marrow transplantation in rat hindlimb ischemia. J
Pharmacol Sci 2005;99:45–51.
54. Minamino K, Adachi Y, Okigaki M, et al. Macrophage colony-stimulating factor (MCSF),
as
well
as
granulocyte
colony-stimulating
factor
(G-CSF),
accelerates
neovascularization. Stem Cells 2005;23:347–54.
55. Sesti C, Hale SL, Lutzko C, Kloner RA. Granulocyte colony-stimulating factor and stem
cell factor improve contractile reserve of the infarcted left ventricle independent of restoring
muscle mass. J Am Coll Cardiol 2005;46:1662–9.
56. Woo YJ, Grand TJ, Berry MF, et al. Stromal cell-derived factor and granulocytemonocyte colony-stimulating factor form a combined neovasculogenic therapy for ischemic
cardiomyopathy. J Thorac Cardiovasc Surg 2005;130:321–9.
57. Zbinden S, Zbinden R, Meier P, Windecker S, Seiler C. Safety and efficacy of
subcutaneous-only granulocyte-macrophage colony stimulating factor for collateral growth
promotion in patients with coronary artery disease. J Am Coll Cardiol 2005;46:1636–42.
58. Hill JM, Syed MA, Arai AE, et al. Outcomes and risks of granulocyte colony-stimulating
factor in patients with coronary artery disease. J Am Coll Cardiol 2005;46:1643–8.
59. Kang HJ, Kim HS, Zhang SY, et al. Effects of intracoronary infusion of peripheral blood
stem-cells mobilised with granulocyte-colony stimulating factor on left ventricular systolic
function and restenosis after coronary stenting in myocardial infarction: the MAGIC cell
randomized clinical trial. Lancet 2004;363:751– 6.
60. Ince H, Petzsch M, Kleine HD, et al. Preservation from left ventricular remodeling by
front-integrated revascularization and stem cell liberation in evolving acute myocardial
infarction by use of granulocyte-colony-stimulating factor (FIRSTLINE-AMI). Circulation
2005;112:3097–106.
61. Wilson RF, Henry TD. Granulocyte colony-stimulating factor and granulocytemacrophage colony-stimulating factor: double-edged swords. J Am Coll Cardiol
2005;46:1649–50.
62. Anderlini P, Przepiorka D, Champlin R, Korbling M. Biologic and clinical effects of
granulocyte colony-stimulating factor in normal individuals. Blood 1996;88:2819–25.
63. Cho HJ, Kim TY, Cho HJ, et al. The effect of stem cell mobilization by granulocyte-
colony stimulating factor on neointimal hyperplasia and endothelial healing after vascular
injury with bare-metal versus paclitaxel-eluting stents. J Am Coll Cardiol 2006;48:366–74.
64. Zohlnhofer D, Ott I, Mehilli J, et al., REVIVAL-2 Investigators. Stem cell mobilization by
granulocyte colony-stimulating factor in patients with acute myocardial infarction: a
randomized controlled trial. JAMA 2006;295:1003–10.
65. Hiasa K, Ishibashi M, Ohtani K, et al. Gene transfer of stromal cell-derived factor-1alpha
enhances ischemic vasculogenesis and angiogenesis via vascular endothelial growth
factor/endothelial nitric oxide synthase-related pathway: next-generation chemokine therapy
for therapeutic neovascularization. Circulation 2004;109:2454–61.
66. Shirakawa Y, Sawa Y, Takewa Y, et al. Gene transfection with human hepatocyte growth
factor complementary DNA plasmids attenuates cardiac remodeling after acute myocardial
infarction in goat hearts implanted with ventricular assist devices. J Thorac Cardiovasc Surg
2005;130:624–32.
<3>67. Sales VL, Engelmayr GC Jr., Mettler BA, Johnson JA Jr., Sacks MS, Mayer JE Jr.
Transforming growth factor-beta1 modulates extracellular matrix production, proliferation,
and apoptosis of endothelial progenitor cells in tissue-engineering scaffolds. Circulation
2006;114 Suppl:I193–9.</3>
68. Liu YJ, Lu SH, Xu B, et al. Hemangiopoietin, a novel human growth factor for the
primitive cells of both hematopoietic and endothelial cell lineages. Blood 2004;103:4449–56.
69. Kirchmair R, Egger M, Walter DH, et al. Secretoneurin, an angiogenic neuropeptide,
induces postnatal vasculogenesis. Circulation 2004;110:1121–7.
70. Mieno S, Ramlawi B, Boodhwani M, et al. Role of stromal-derived factor-1{alpha} in the
induction of circulating CD34+CXCR4+ progenitor cells after cardiac surgery. Circulation
2006;114 Suppl:186–92.
71. Hellstrom M, Kalen M, Lindahl P, Abramsson A, Betsholtz C. Role of PDGF-B and
PDGFR-beta in recruitment of vascular smooth muscle cells and pericytes during embryonic
blood vessel formation in the mouse. Development 1999;126:3047–55.
72. Sato N, Beitz JG, Kato J, et al. Platelet-derived growth factor indirectly stimulates
angiogenesis in vitro. Am J Pathol 1993;142:1119–30.
73. Miyata T, Iizasa H, Sai Y, Fujii J, Terasaki T, Nakashima E. Platelet-derived growth
factor-BB (PDGF-BB) induces differentiation of bone marrow endothelial progenitor cellderived cell line TR-BME2 into mural cells, and changes the phenotype. J Cell Physiol
2005;204:948–55.
74. Hao X, Mansson-Broberg A, Gustafsson T, et al. Angiogenic effects of dual gene transfer
of bFGF and PDGF-BB after myocardial infarction. Biochem Biophys Res Commun
2004;315:1058–63.
75. Richardson TP, Peters MC, Ennett AB, Mooney DJ. Polymeric system for dual growth
factor delivery. Nat Biotechnol 2001;19:1029–34.
76. Li X, Tjwa M, Moons L, et al. Revascularization of ischemic tissues by PDGF-CC via
effects on endothelial cells and their progenitors. J Clin Invest 2005;115:118–27.
BONE
MARROW
77. Dimmeler S. Platelet-derived growth factor CC:a clinically useful angiogenic factor at
last? N Engl J Med 2005;352:1815–6.