Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Myocardial infarction wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
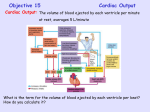
CARDAIC OUTPUT AND ITS REGULATION Learning Objectives By the end of this lecture, the students should be able to understand: • The terminology of cardiac function: Cardiac output, venous return, stroke volume and ejection fraction • The factors regulating cardiac output • Effect of preload, contractility, and afterload on stroke volume and cardiac output. • Positive and negative chronotropic and inotropic effects Cardiovascular System • The goal of the cardiovascular system is to maintain adequate blood flow to all body tissues – The heart works in conjunction with cardiovascular centers and peripheral blood vessels to achieve this goal Definition of Cardiac Output Cardiac output is the volume of blood pumped by heart each minute. • It is product of heart rate and stroke volume and averages about 5.25L/min. Cardiac output = heart rate x stroke volume Heart Rate=number of beats per minute Stroke volume=amount of blood ejected in each beat • Venous Return • Quantity of blood flowing from the veins into the right atrium per minute • In steady state, the heart pumps blood at the same rate at which blood enters the heart ; Cardiac Output (CO)=Venous Return (VR) • For the normal heart, CO is largely determined by events in peripheral circulation • Venous Return derives Cardiac Output Factors Affecting Cardiac Output Heart rate • Heart rate is no. of beats /min. • It is typically 70 to 80 beats/min in young adults but higher in children and elderly. • Adjustments in HR are important in the short term control of CO and BP. • A persistent high resting HR above 100bpm is called tachycardia and a persistent low resting rate below 60bpm is called bradycardia Cardiovascular Center • Nervous system regulation of heart originate in the cardiovascular center in medulla oblongata • This region of the brain stem receives input from variety of sensory receptors and from higher brain centers, such as limbic system and cerebral cortex • The cardiovascular center then directs appropriate output by increasing or decreasing the frequency of nerve impulses in both sympathetic and parasympathetic branches of ANS Autonomic Activity • • Sympathetic stimulation – Positive inotropic effect – Increases HR and SV – Releases NE – Dominant during exercise and stress Parasympathetic stimulation – Negative inotropic effect – Decreases HR and SV – Releases Ach – Dominant at rest Stroke Volume • The amount of blood that leaves the heart with each beat or ventricular contraction. – Not all blood ejected – Normal Adult 70 ml / beat Stroke volume = end-diastolic volume – end-systolic volume • End-diastolic volume = volume in ventricle before ejection (ml). • End-systolic volume = volume remaining in the ventricle after ejection (ml) • Ejection fraction: The fraction of end-diastolic volume ejected in each stroke volume Ejection fraction = stroke volume/End- diastolic volume Preload/Afterload • Determinants of stroke volume • Preload tension on ventricular muscle before contraction determined by left ventricular end diastolic volume • Afterload pressure against which ventricles pump blood determined by total peripheral resistance Frank-Starling Mechanism “within physiological limits, the heart pumps all the blood it receives without allowing excessive damming of blood in the veins” • Increased Venous return • Increased cardiomyocyte contractility • Increased stroke volume Frank-Starling Mechanism • • • • • Increased venous return increases the ventricular filling (end-diastolic volume) and therefore preload Myocyte stretching increases the sarcomere length The myocardial fibers are stretched, the force of contraction is increased The length of the fiber is determined primarily by the volume of blood in the ventricle, thus EDV is the primary determinant of preload This mechanism enables the heart to eject the additional venous return, thereby increasing stroke volume. End Diastolic Volume • Two factors determine : 1- The duration of ventricular diastole. 2- Venous return • When HR increases, the duration of diastole is shorter. Less filling means a smaller EDV. • When venous return increases, a greater volume of blood flows into the ventricles and EDV is increased. • SV is directly proportional to EDV Contractility • Second determinant of SV • Contractility of the myocardium refers to its contraction force for a given preload. • An increase in tension resulting from increased stretch and increase that make the myocytes more responsive to stimulation. Contractility • Factors that increase the contractility are called positive inotropic agents • positive inotropic agents produce increase in SV and cardiac output for a given end diastolic volume. • Thus a larger fraction of the end diastolic volume is ejected and there is increase in ejection fraction. • Agents that decrease contractility have negative inotropic effect. • They produce decrease in SV and cardiac output for a given end diastolic volume. • So smaller fraction of the end diastolic volume is ejected per beat and there is decrease in ejection fraction Afterload • It is the load against which myocardial fibers contract or shorten during systole. • It includes: • aortic pressure • peripheral resistance • blood volume • viscosity of blood Measurement of Cardiac Output • • The oxygen Fick method Indicator dilution method Fick method of measuring cardiac Output Cardiac output = O2 absorbed per minute by the lung (ml/min)/ Arteriovenous O2 difference (ml/L of blood) REFERANCE MEDICAL PHYSIOLOGY GUYTON & HALL 12TH EDITION Pg # 229 – 231 ************************************************************************