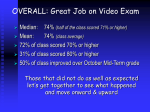
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Shoulder Rotator Cuff Tear MOI: fall on shoulder, trauma, progressive tear over time without trauma Etiology: usually male over 60 yo c/o: unable to initiate abduction, experiences pain if partial tear; cannot initiate abduction and will shrug shoulder instead if complete tear Best exam findings: o Complete Tear MSTT: weak and painless MMT: grade 0/5 o Partial Tear Palpation for condition (swelling) MSTT: weak and painful P for T: pain over RTC tendon o Positive Special Tests: empty cans, ER/IR lag signs, drop arm SLAP Lesion (Superior Labral Anterior Posterior) Tear in labrum from anterior to posterior on superior aspect disrupting suction cup effect within GH joint, which lessens stability MOI: FOOSH or deceleration with throwing Involves Long Head of Biceps Tendon Best exam findings: MLT, MMT (anything lengthening biceps tendon) Special test: comp with rotation , biceps load test I/II, OBRIEN’S Impingement Syndrome MOI: postural/functional, nerve, trauma, disease Humeral head is bumping into acromion when arm is raised – joint space decreased Signs & Symptoms: o Structural: spurs, shape of acromion, thickened rotator cuff tendon, increased prominence of greater tuberosity of humerus o Instability/laxity: humeral head does not sit in glenoid causing poor arthrokinematics, increased muscular effort, anterior/posterior/inferior hypermobility, Bankart lesion (etc). o Hypomobility: capsular pattern (er>abd>ir) of restriction (hypomobile inferior direction), adhesion commonly in inferior capsule o Muscle imbalance (tightness/weakness) Weakness posteriorly: rotator cuff, scapulothoracic musculature, humeral head depressors Tightness anteriorly: pec minor/major, shoulder internal rotators o Structural inspection: increased thoracic kyphosis, forward head, rounded shoulders, anterior scapula with internally rotated humerus o Tx: stretch, posture, activity mod, after 6 weeks tx refer to MD if not improved Tendinosis / tendinitis of biceps or any of the rotator cuff muscles Best exam findings: o Palp for cond: warmth, redness, swelling at biceps tendon OR supraspinatus o MSTT: strong and painful with flex and supination (biceps) OR ER and abd (supra) o MLT: pain with lengthening o Palp for tenderness over tendon Treatment: calm inflammation, trans-friction massage, effleurage, eccentric exercises, US, treat source of pain Subacromial bursitis c/o: pain over lateral brachial region of shoulder, usually gradual onset, Hx of tendonitis/osis, comfort in loose-packed position (20 flex/20 abd) Best exam findings: o Palp for cond: warmth/swelling over bursa o PROM: pain in any direction that compresses bursa o AROM: pain in any direction when contracting muscle is over bursa o Palp for tenderness: painful over bursa Hypo or hypermobility/instability of GH joint Dislocations Anterior GH Joint Dislocation o Complications include: long head of biceps tear, RTC tear, axillary nerve (delt, teres min) injury, AC joint dislocation, SC joint dislocation Adhesive capsule Etiology: o Gradual insidious onset o Result of immobilization or other pathology o Inflamed capsule that adheres to humeral head o Capsule can become fibroticshoulder stuck and ball bearing movement no longer is fluid o Occurs in perimenopausal women, diabetes, trauma, prolonged immobilization o c/o of sore to sleep on side, difficulty with doing hair and fastening bra Clinical manifestations: o Passive ROM limited in capsular pattern: Classical ROM: ER > Abd > IR Accessory ROM: anterior glide > inferior glide > posterior glide 5 best exam findings: 1. AROM: decreased ER > Abd > IR 2. PROM Classical – quantity: ER > Abd > IR 3. PROM Accessory – quantity: anterior glide > inferior glide > posterior glide 4. PROM Classical – quality: capsule tightness end-feel 5. PROM Accessory – quality: capsule tightness end-feel Peripheral nerve entrapments Suprascapular nerve entrapment (supra or infra mm) o Entrapped under suprascapular ligament or at tight, bony suprascapular notch o Presentation: pain with insidious onset; deep, dull aching pain at posterior shoulder; shoulder weakness, specifically of supraspinatus o Best exam findings??: MSTT: strong and painful ER and abd Palp for tenderness: discomfort over midpoint of superior scapular border Elbow Lateral Epicondylitis/tendinosis (Tennis elbow) Repetitive use injury that involves overuse of extensors; muscles primarily involved: ECRL, ECRB and ED – ECRB tendon is usually most inflamed Symptoms: pain over tendon, pain at lateral epicondyle, loss of function, pain with gripping Best exam findings o Positive P4C over lateral epicondyle (warmth, redness, edema); -osis will be unremarkable o Strong and painful MSTT for elbow/wrist extension, especially for ECRB (middle finger) o MLT: pain and limitation with lengthening involved muscles (extensors) o Positive P4T over ECRB tendon, lateral epicondyle o Other Exam findings Pain over lateral aspect of the elbow with radiating pain down the forearm Decreased strength with pain, especially while grasping something Rule out radial nerve (test supinator ) Medial Epicondylitis/tendinosis (Golfer’s elbow) Typically involves FCR and pronator teres muscles; occasionally palmaris longus, FCU and FDS Symptoms: pain and tenderness over involved muscles, loss of function Best exam findings o o o o o Positive P4C over medial epicondyle (warmth, redness, edema); -osis will be unremarkable Strong and painful MSTT for wrist flexion MLT: pain and limitation with lengthening involved muscles (flexors) Positive P4T over medial epicondyle and involved muscles Other Exam findings Pain over medial aspect of the elbow with radiating pain down the forearm Loss of function when picking something up with elbow flexion Biceps tendonitis/tendinosis Best exam findings o Positive P4C over tendon insertion (warmth, redness, edema); -osis will be unremarkable o Strong and painful MSTT for elbow flexion and possibly shoulder flexion as well as well as supination o MLT: pain and limitation with lengthening of biceps muscle o Positive P4T over biceps tendon Triceps tendinosis/tendonitis Usually results from a sudden severe strain to the triceps; could also be an overuse injury Best exam findings o Positive P4C over tendon insertion at the elbow (warmth, redness, edema); -osis will be unremarkable o Strong and painful MSTT for elbow extension and shoulder extension o MLT: pain and limitation with lengthening of triceps muscle o Positive P4T over tendon Myositis Ossificans Heterotopic bone formation between muscle fibers that results from trauma/bleeding in area; commonly seen in brachialis muscle with supracondylar fractures, posterior dislocations of elbow, and aggressive stretching of elbow flexors Best exam findings o P4C – increased warmth over muscle o Decreased A/PROM – going further into range is painful o Normal accessory PROM – the muscle is limiting, not the capsule o MSTT/MMT – resistance causes increased pain o Positive P4T over muscle, may feel a mass NO stretching, massage or possibly use US with caution, use pulsed settings Hypomobility due to prolonged immobilization Following surgery, injury/fracture Best exam findings o Decreased A/PROM with capsule tightness end-feels o Decreased accessory mobility Ulnar nerve entrapment/Cubital tunnel syndrome Can be the result of a fracture, dislocation or subluxation at elbow Motor to hypothenar muscles and small, deep muscles in hand (Interossei), adductor policis Sensory to the ulnar side of the hand, pinky and ulnar half of ring finger Best exam findings o If motor – decreased muscle strength (MMT) and possible positive MSTT o If sensory – diminished sensation in distribution, positive ULTT (shld dep, 10 abd, elbow flex ,sup, ER, wrist ext, ulnar dev) ulnar n. Median nerve entrapment/Pronator syndrome (sld dep, abd, elb flex-sup, ext wrist, er shld, ext elbow, abd) Motor to APB, OP, FPL, FPB, FDS, palmaris longus, FDP 1 & 2, lumbricals 1 & 2 Sensory to palmar surface of thumb, index and middle fingers Best exam findings o If motor – decreased muscle strength (MMT) and possible positive MSTT o If sensory – diminished sensation in distribution, positive ULTT for median n. Anterior interosseous nerve branch o Entrapped at the elbow by pronator teres and MOTOR only o Innervates: FPL, FDP, PQ o Unable to do pinch grip test Radial nerve entrapment/Radial tunnel syndrome Can be following trauma such as a fracture to the radial head Deep branch is motor only – EPL, EPB, APL; commonly entrapped at supinator muscle belly Superficial branch is sensory to the dorsal aspect of the hand; common entrapment at ECRB Best exam findings o o If motor – decreased muscle strength (MMT)/positive MSTT for supination, decreased MLT and + P4T of supinator If sensory – diminished sensation in distribution, positive ULTT (shldr, abd, pron, wrist flex, ulnar dev,) for radial n., MSTT/MMT reproduces symptoms, MLT – parasthesia with lengthening, + P4T at ECRB UCL- 0-60: ANT POSTION OF ANT BUNDLE/ POST PORTION OF ANT BUNDLE 60-120/ POST BUNDLE MOST TAUT AT 90-140 -P4C -PROM -SPECIAL TEST: MOVING VALGUS, MILKING, VALGUS- 0 DEG OSSEOUS, MM, LIG/ 30 DEG MORE ANT PORTION OF ANT, MORE POST FAT PAD: flex fat pat in fossa, as it ext fat pad has to move out to let olecranon move in -differentiat from triceps tendonopathy Wrist and Hand Carpal tunnel syndrome o Diagnosis: some irritation of the Median N at the wrist; decreased sensation and motor involvement from the wrist up o Best Exam findings Neurovascular: paresthesia in median nerve sensory distribution, derm, myo, ULTT MMT History: c/o night pain o Other exam findings History: aggravated by any movements of the wrist Weakness/atrophy of thenar muscles (esp. AbdPB) o Causes Trauma: fracture/fall, disease, space occupying lesion (cyst) Ergonomics: “overuse” of typing position with bad posture Displaced lunate: FOOSH injury Edema: increased intra-capsular fluid Flexor retinaculum tightness Tight flexors Pronator teres syndrome C5-T1 nerve root scalenes Hypomobility due to prolonged immobilization o Usually follows surgery or fracture/injury o Best exam findings Decreased A/PROM with capsule tightness end-feels Decreased accessory mobility in the direction of limitation with capsular tightness end feel Lateral epicondylitis/osis (aka: tennis elbow) o Repetitive use injury that involves overuse of the extensor muscles o Primary muscles involved: ECRB**, ECRL, ED o Best exam findings P for C: -itis: will have positive results; -osis: will not have any results MSTT: strong and painful elbow extension and wrist extension MLT: pain and limitations while lengthening ECRL, ECRB, ED P for T: tenderness just distal to lateral epicondyle and/or ECRB muscle o Other Exam findings Pain over lateral aspect of the elbow with radiating pain down the forearm Decreased strength with pain, especially while grasping something Medial epicondylitis/golfer’s elbow o Primary muscles involved: FCR and pronator teres (occasionally palmaris longus, FCU and FDS) o Best exam findings P for C: same as lateral epicondylitis MSTT: strong and painful elbow flexion and wrist flexion MLT: pain and limitations while lengthening FCR and pronator teres P for T: tenderness just distal to medial epicondyle o Other Exam findings Pain over medial aspect of the elbow with radiating pain down the forearm Loss of function with picking something up with elbow flexion De Quervain’s syndrome o Tenosynovitis on the APL and EPB o Pain in thumb with flexion and (+) Finkelstein’s test o Possible causes: tight pronators, hypermobility o o Rule out scaphoid fx and superficial radial nerve damage Exam findings Wrist pain that radiates proximally up the forearm and distally towards the thumb P for T: over APL and EPB tendinous sheath and radial styloid process Pain with contraction and/or lengthening of the two muscles (+) Finkelstein’s test Dupuytren’s contracture o Contracture of palmar fascia flexion deformity of MCP and PIP of 4th and 5th digit o Insidious onset o No muscle involvement o No sensory involvement Ulnar nerve entrapment o Three main areas of entrapment: cubital tunnel, guyon’s canal and forearm flexors o Motor to: FCR, FDP (medial half), ODM, AbdDM, FDM, 3rd/4th lumbricals, D/P interossei, AddP, PB o Sensation to: ulnar side of hand, ½ ring finger, pinkie o MOI: Direct trauma- fall on elbow Traction of nerve, changes in carrying angle Degeneration Fracture in area Dislocation and/or subluxation of elbow o Best exam findings If motor- decreased muscle strength (MMT) and possible positive MSTT If sensory- diminished sensation in distribution, positive ULTT for ulnar N. Medial nerve entrapment/Pronator teres syndrome o Sites of entrapment: carpal tunnel, scalene, medial humeral condyle, pronator teres, biceps aponeurosis, ligament of Struthers, cubital fossa o Motor innervation: AbdPB, FPL, FPB, lumbricals ½, PL, FDS, FDP, PT, FCR, PQ, OP o Sensory innervation: palm of thumb, first and second finger o Found in MLT o Anterior interosseous nerve branch Entrapped at the elbow by pronator teres and MOTOR only Innervates: FPL, FDP, PQ Unable to do pinch grip test Radial nerve entrapment o Entrapped by the supinator or ECRB (usually atraumatic) o Direct trauma- fracture to radial head or direct blow to area o Deep branch- motor only Entrapment at the supinator muscle belly (+) exam findings MSTT/MMT: weak contraction of the supinator MLT/PROM: pain with lengthening supinator P for T: at supinator o Superficial branch- sensory only to dorsal aspect of hand Entrapment at ECRB or CMC area (+) exam findings MSTT/MMT: reproduces symptoms with contraction of ECRB MLT: reproduces symptoms with lengthening of ECRB P for T: at ECRB o Intersection syndrome Differentiate Sx: 2nd tunnel Mstt, mlt, p4t, possible special test Foot & Ankle Hypermobilities resulting in excessive pronation Pronation involves DF, abd, and eversion Hypermobilities would present during joint accessory mobility: o A/P glide of talus on tib/fib o Medial glide of talus on tib/fib o Lateral arc glide of calcaneus Plantar Fasciitis MOI: increased hindfoot pronation (stressed/overworked/stretched) OR supination (tight/stressed when walking) Best exam findings: o MLT of plantar fascia (ankle and great toe DF) o Palp for tenderness: calcaneal insertion (medial calcaneal tubercle) Treatment: o Usually over-pronated so strengthen arch supporters, tapeorthotics or arch support, ionto, deep tissue stretching Hallux valgus Lateral deviation of 1st MTP, bone not properly aligned Difference between structural and positional hallux valgus: if structural, the valgus position will not be changed, the joint can’t maintain proper alignment MOI: Impairments that can cause hallux valgus: o Hypermobility of capsule o Effusion/edema o Muscle weakness o Muscle tightness Bunions Prominence of MT head at 1st MTP; exostosis and callus may form Causes: hallux valgus, instability at first TMTrotation of MT shaft=prominence Tendinosis/tendinitis of tibialis posterior MOI: overuse/overactivity, could be gradual onset Presentation: o Pain and swelling, loss of arch and development of flatfoot, inability to stand on toes Best exam findings: o Palp for cond: warmth, swelling, redness over medial ankle o MLT: pain with DF and eversion o MSTT: strong and painful for PF o Palp for tenderness: at medial ankle behind medial malleolus Tendinosis/tendinitis of Achilles tendon MOI: running, jumping, gradual onset Best exam findings: o Palp for cond: warmth, swelling, redness over posterior ankle o MLT: pain with DF (knee flexed) o MSTT: strong and painful for PF o Palp for tenderness: at distal tendo-Achilles Compartment syndrome MOI: increased pressure within a closed location results in increased pressure on neurovascular and muscle structures o Acute (trauma)chronic (exercise induced) Best exam finding: o Neurovascular: myotomes, dermatomes, capillary refill Compartment Contents: o Anterior compartment: Deep peroneal nerve (anterior tibialis, EHL, EDL, peroneus tertius), anterior tibial artery and vein o Lateral compartment: Superficial peroneal nerve (peroneals) o Deep posterior compartment: Tibial nerve (flexor digitorum, posterior tibialis, FHL), posterior tibial artery and vein, peroneal artery and vein Posterior tibial exertional compartment syndrome: o Common MOI: rearfoot pronation o Treat inflammation firect then decrease aggravating activity; maybe arch supports/orthotics Antero-lateral compartment syndrome: o Common MOI: trauma to anterior tibia; weak DF, tight gastroc/soleus Medial tibial stress syndrome: o Tibial periositis at medial soleus or posterior tibialis o Palp for tenderness: distal post-med border of tibia Ankle sprains Anterior talofibular o MOI: PF with inversion o Blends with joint capsuleleading to joint effusion Calcaneofibular o MOI: neutral PF/DF with inversion o Common injury to peroneal tendon Posterior talofibular o MOI: inversion Anterior tibiofibular (“high ankle sprain”) o MOI: ER/IR with eversion; talus driven up between tib/fib on landing o Fibular fractures common Deltoid ligament o MOI: eversion force, rarely damaged o More likely to avulse part of tibia before spraining this ligament Stress fractures Uni-malleolar fracture Bi-malleolar fracture Trimalleolar fracture: both malleoli and other structure, usually posterior distal aspect of tibia o Usually surgically resolved Pott’s fracture/dislocation o Any dislocation and fracture of malleoli Impairments: atrophy, capsule tightness, decreased ROM, swelling MD Treatment : closed reduction or ORIF, casted/immobilized o Complications: decreased ROM, swelling, malunion o Possible end-feels for classical DF s/p immobilization for distal tib/fib: abnormal muscle, tight muscle, swelling, capsule tightness Morton’s Neuroma c/o: pain over metatarsals; change in sensation in webspace of toes Best exam findings: o Palp for tenderness: between the metatarsal heads Cause: bundle of nerves inflamed o e.g. tight toe box in shoes, high heels Diff between neuroma and interdigital nerve entrapment: o If pressure removed from interdigital nerve the symptoms will dissipate, but there will be no change if it is a neuroma Shin Splints Causes: overuse, stress fractures, overpronation/flat feet Usually seen in runners c/o: dull, aching pain in anterior lower leg Anterior Compartment Syndrome Pain increases with exercise No pain at rest MSTT (-) Neurovascular symptoms Shin Splints/Anterior Tendonitis Pain decreases with exercise Pain remains after stopping activity MSTT (+) No neurovascular symptoms Knee ACL/PCL Injuries (pre-surgical) – I did what I could with this one based on the notes ACL tear symptoms: feeling of “giving way” while walking, possible effusion and hemarthrosis PCL tear – common MOI is a dashboard injury or falling on a flexed knee ACL tear best exam findings o Decreased A/PROM for knee extension o Positive anterior drawer/Lachman’s/anterolateral pivot shift tests PCL tear best exam findings o Positive posterior sag test and Godfrey’s test ACL reconstruction Performed if patient is an athlete or is high-functioning; this diagnosis would be obvious if they are coming from the doctor; treatment would follow protocol MCL Injury MOI: valgus stress with or without a combined rotational stress Symptoms o 1st degree sprain: pain with palpation and positive valgus stress test o 2nd degree sprain: severe pain with palpation and ligament stressing, swelling within 24 hours o 3rd degree sprain: ligament ruptured, knee unstable, no activity, fluid inside and/or outside of joint LCL Injury MOI: varus stress Symptoms o 1st degree sprain: pain with palpation and positive varus stress test o 2nd degree sprain: severe pain with palpation and ligament stressing o 3rd degree sprain: ligament ruptured, knee joint becomes unstable Meniscus tears Common injury with forced ER during flexion or forced IR during extension; also hyperflexion Symptoms: acute joint line pain, joint effusion gradually develops, pt. may complain of buckling or giving way of knee, difficulty with full knee extension, “locking” of knee experienced at 20-45°, squatting is painful Best exam findings o Decreased A/PROM o Positive McMurray’s and Apley’s compression ITB Syndrome Symptoms: pain WITH activity, not at rest; anterior, lateral and “deep” knee pain Best exam findings o Positive P4T over Gerdy’s, lateral retinaculum and/or lateral epicondyle o Positive Nobles compression or Patla’s variation of Nobles test Unhappy Triad Injury to the knee that consists of all of the following: ACL tear, MCL tear and meniscus tear You would see signs and symptoms of all of the above Patellar tracking disorders Patellofemoral syndrome is a generic name for anterior knee pain of gradual onset, especially while sitting or descending stairs; common with a lateral tracking patella Some causes of compression of lateral patellofemoral articulation: rotary limb mal-alignment (increased Q-angle), abnormal position of tibia relative to femur (genu varus/valgus), knee hyperextension (patella alta), increased foot pronation medial tibial rotation…, abnormal tracking and crepitus in weight-bearing, soft tissue restrictions such as a tight lateral retinaculum, VMO atrophy, pelvic instability, and where the medial retinaculum attaches (pain with lateral glide of patella) Any of these characteristics can lead to the anterior knee pain caused by compression at the lateral patellofemoral articulation Best exam findings with a lateral tracking patella: o Pain with active knee extension and passive knee flexion o Hypomobile medial glide of the patella o Strong and painful MSTT for knee extension o Positive patella compression special test o Positive P4T over medial retinaculum, patellar tendon, distal ITB and biceps femoris tendons Patellar tendon injuries Patellar tendonitis can be caused by excessive jumping, hip/foot problems (altered mechanics), or muscle imbalances Symptoms: pain with jumping/running, decreased pain with rest, pain with stairs, pain that limits function, some swelling Best exam findings o Positive P4C over knee (warmth, redness, edema) o Strong and painful MSTT for knee extension o Positive Thomas test (MLT) o Positive P4T over tendon Note – patellar tendonitis and Osgood Schlatter’s disease present the same; look at age and imaging to confirm Quadriceps and Hamstring injuries – FYI: I kind of made these up after reading through the notes Best exam findings will vary depending on the injury, but the most common theme will be: o Positive P4C over the site of injury o Decreased A/PROM with probable abnormal muscle end-feel o Strong and painful MSTT o Decreased MLT due to pain or inability to get into test position o Muscle weakness Osteoarthritis Best exam findings – not in the actual notes, but these were the best I came up with o Pain, especially with prolonged activity o Positive P4C – inflammation o Decreased A/PROM o Muscle weakness Knee Arthroplasty Straight-forward diagnosis coming from the doctor; treatment will follow protocol Hip OA o Best exam findings Pain especially with prolonged activity P for C: inflammation Decreased A/PROM (classical and accessory) Muscle weakness o Other exam findings History: pain is worst in the morning, pain and stiff joints THA o THA approaches and limitations Anterior: between sartorius/RF/TFL/Glut min-med No ABD, extension or IR beyond neutral Anterolateral: between glut med and TFL No ABD, extension or IR beyond neutral Direct lateral: release anterior ABD from greater trochanter Posterolateral: combination of posterior approach with distal limb No hip flexion >90, ADD past midline and IR past neutral Transtrochanteric: involves the osteotomy of greater trochanter NO active ABD o Exam findings Depends on the approach Probably going to find P for C Definitely decreased A/PROM, but don’t do accessory mobility Probably weak MSTT Definitely decreased length Definitely week Limited mobility due to hypomobile capsule and/or muscle imbalance o Decreased A/PROM with hypomobile capsular end feel or abnormal muscle end feel o Decreased accessory mobility with hypomobile capsular end feel o Decreased muscle length o Decreased strength o ** all of these depend on which direction of tightness and/or what muscles are weak Trochanteric bursitis o Pain assessments: On-set of pain is insidious or associated with particular activity o History: subjective – what your patient is telling you Aggravated by ascending stairs Pressure/lying on the involved side- awakened at night due to pain Complains of deep aching Pain with crossing legs o Palpation for condition One of the BEST exam findings (may not be seen in every patient) warmth and swelling seen o o AROM: Pain at end range of active motion PROM Passive ADD will be painful and limited Passive flexion with ADD and IR will be painful No pain with accessory joint movements o MSTT: Possible strong and painful for hip ABD, extension and ER due to contraction of muscles that run over the bursa o MMT: Possible pain o MLT: Positive Ober’s test with pain and tightness (both regular and modified) o Palpation for condition: tenderness over greater trochanter Piriformis syndrome: piriformis muscle has been implicated as a potential source of sciatic symptoms causing buttock and hamstring pain o Short piriformis syndrome (hip impingement syndrome) Typical symptoms No lower back pain Butt, thigh and LE paresthesia Patient complains of pain in butt which increases with prolonged WB and sitting Relief comes with standing or walking Structural inspection: standing foot turned out with leg ABD and ER, “flat” back Gait: lack of HS, short stride length, and walk with knee bent P for T: deep palpation of piriformis will provoke distal symptoms MLT: lengthening of piriformis with produce symptoms MMT: rotators will Neurovascular: (+) SLR and slump test Decreased A/PROM (classical and accessory) Adductor or iliopsoas strains o Adductor Usually the adductor longus MOI: most common in sports that involve rapid change in direction; often experienced with squatting, lunging and twisting; can be chronic from overuse Exam findings Pain with resisted hip ADD and passive elongation of ABD Tendinosis/tendinitis of iliopsoas/rectus femoris o Best exam findings Strong and painful MSTT for hip flexion and knee extension Positive P for C: over tendon insertion above the patella (warmth, redness, edema); not going to see with iliopsoas Positive P for T over tendon MLT: pain and limitation with lengthening of iliopsoas and rectus femoris ITB syndrome o Signs and symptoms Pain about 2cm above joint line over condyle with 30⁰ flexion History: complaint of lateral, deep knee pain, occurs when doing activity and not painful at rest Referred pain from the lower back Deep knee pain o Best exam findings P for T: at lateral condyle, gerdy’s tubercle and lateral retinaculum (+) Noble’s compression and Patla’s version of noble’s