Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
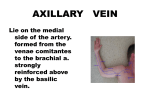
Elbow, Radius, and Ulna Anatomy - Annular ligament holds the radius & ulna together Humeroulnar joint is the true elbow joint Innervation o Median nerve Crosses elbow medially Passes through the 2 heads of the pronator teres o Ulnar nerve Passes along medial arm & posterior to the medial epicondyle Through the cubital tunnel o Radial nerve Descends the arm laterally, dividing into the superficial (sensory) branch & the deep (motor or posterior interosseous) branch The deep branch passes through the arcade of frohse, where it is most susceptible to injury History & PE - - - - History most important Inspection o Expose the area! Actually look at the skin o Carrying angle Normally 10-15 degrees Female > Male Valgus >15 degrees Varus <10 degrees If not able to bend/extend elbow all the way, get an XR! Grading muscle strength o 0/5 no muscle movement o 1/5 visible movement but not at the joint o 2/5 movement at the joint but not against gravity o 3/5 movement against gravity but not against added resistance o 4/5 movement against resistance but less than normal o 5/5 normal strength Neuro Exam o Tinel’s test: Tapping over a nerve to elicit pain/radiculopathy along the nerve Diagnosis o Flexor-Pronator Mass Syndrome Median nerve becomes trapped between heads of pronator teres muscle Repeated protation Resisted flexion of FDS tendon of middle/index finger Papal sign o See below for rest of dx SDLS - Room 1 o HPI = 2 y/o crying, refused to move right arm; brother yanked arm but denies trauma o - - - - - Significant signs: No tenderness over shoulder, wrist, forearm; neuro signs normal; No flexion at elbow/stuck in Extension and pain when testing ROM; No fracture Dx = Nursemaid's elbow (Radial head Subluxation) Tx = NSAIDs o o Room 2 o HPI = 59 male RUE pain/swelling; was bowling when sudden pop in upper arm; has visible balled up muscle/bruising o Significant signs = Apparent pain but cooperative; Triceps/brachioradialis 2+/4 in right upper extremity; No biceps reflex in right upper extremity; Muscle strength 3-4/5 in right arm with supination/flexion; 5/5 in left; Anterior soft tissue mass in right arm with tenderness and muscle guarding/patient is holding arm at 90 degrees; Ecchymosis noticed on right upper arm; no Fx o Dx = Right biceps tendon rupture o Tx = naproxen and icing; considering OMM if needed; refer to surgery for complete rupture, PT for partial rupture Room 3 o HPI = 47 yo male with right elbow pain described as sharp/achy on inside part of right elbow that started after he golfed; Tylenol has minimal benefit; moving aggravates pain; mild pain radiation towards wrist but not encompassing hand o Significant signs = Equal Deep tendon reflexes on both arms; with normal upper bilateral strength without atrophy; pain in medial epicondyle that is aggravated with wrist abduction against resistance; No pain on lateral epicondyle o Dx = Medial epicondylitis with posterior radial head o Tx = Naproxen; ME for posterior radial head/IO membrane release Room 4 o HPI = 42 female with right elbow pain starting after racquetball; pain worse when extending arm/wrist and improves with rest; mild radiation towards hand o Significant signs = Equal Deep tendon reflexes on both arms; with normal upper bilateral strength without atrophy; Normal flexion/extension at elbow/wrist; increased tenderness over lateral epicondyle worsened with resisted supination and resisted extension of third finger in pronated position; Anterior radial head o Dx = Lateral epicondylitis, Anterior Radial head o Tx = Naproxen; ME for anterior radial head/IO membrane release Room 5 o HPI = 22 College pitcher with right elbow pain worsening over past month; constant aching pain when he pitches/plays; 800 mg of Ibu not helping, rest helps slightly; occasional popping/catching/grinding after 40+ pitches; medial elbow pain when gripping ball o Sig Signs = Equal Deep tendon reflexes on both arms; with normal upper bilateral strength without atrophy; maintains flex/ext and sup/pronation with only mild crepitus upon flex/ext; direct palpation also elicits mild pain; valgus stress has mild gapping with proximal ulna pain; anterior radial head; No fx, bone spurs, loose fragments o Dx = UCL injury (possible tear); anterior radial head -> test with valgus/varus test by checking the collateral ligaments (main stabilizers) at 30 degree flexion o Tx = Naproxen 550, ME for ant radial head/IO membrane release Room 6 o HPI = 48 male with right elbow pain without trauma after golfing; constant elbow pain, aching, nonradiating o Sig Sings = swelling/redness at posterior elbow; Right upper extremity edema; erythema overlying right olecranon; tender to palpation; decreased extension; Strength/DTR norm; Right shoulder/wrist and left arm normal; no bony destruction - o Dx = Olecranon bursitis o Tx = NSAID and potential aspiration/injection if no improvement; IO membrane release Room 7 o HPI = 39 male has difficulty moving index/middle finger with weakness; difficulty bending IP joint in thumb; Upper forearm pain radiating to elbow o Sig signs = normal neuro; joints in thumb/index finger are straight instead of bent when pinching; enveloped biceps tendon bursa upon US; no Fx o Dx = Anterior Interosseous syndrome (compression of anterior IO nerve- branch of median nerve) -> innervates Flexor digitorum profundus, Flexor pollicis longus, Pronator quadratus (Almost only motor loss) **issue with DIP joint o Tx = NSAID, steroids, rest, PT, surgery as last option