Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
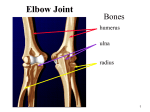
10 – Exam of Elbow, Radius and Ulna - - - - Elbow o Uniaxial hinge joint o 50% plus injuries sports/recreational related o Non-traumatic/overuseinjuries equal or exceed traumatic occurrences. Multifaceted articulation o Capitellum and Troclea of distal end of Humerus combine with: Radial Head and Olecranon of proximal radius and ulna Anular ligament holds the radius and ulna together Humeroulnar joint is TRUE elbow joint Capsule is reinforced and thickened by lateral and medial collateral ligaments Resists and prevents excessive AB and AD duction Does not impede supination of pronation o Ulnar Collateral Ligament Fan shaped – most important stabilizer Full extension provides 30% of stability 54% in 90degree flexion, possible up to 70% Radial head is an important secondary stabilizer in flex/ext – 30-33% of stability Innervation o Median Nerve Crosses elbow medially – passes through two heads of pronator teres o Ulnar Nerve – medial epicondyle Passes along medial arm and posterior to the medial epicondyle through the cubital tunnel o Radial Nerve – lateral epicondyle Descends arm laterally, divides into superficial (sensory) branch and deep (motor or posterior interosseus) branch. Deep Branch passes through Arcade of Frohse where it is most susceptible to injury H&P examination o History Inspection Palpation ROM Muscle/Neuro Testin Specific tests o PQRSTA Provocative or Palliative – what causes, what helps? Quality or Quantity – Character of symptom – dull, sharp? Region or Radiation – where, spread? Severity – 1-10 Timing – when did it begin? How long does it last? How often? Sudden/gradual? Associated signs and symptoms of chief complaint o Always examine joint above and below o Cardinal signs of inflammation Rubor Swelling - - - - - - Heat Pain Loss of function o Inspection Bilateral comparison – asymmetry Carrying angle – normal = 10-15 degrees of valgus Cubitus Valgus = Cubitus angle > 15 degrees o Results in forearm ab duction Cubitus Varus = Cubitus angle < 10 degrees o Results in forearm ad duction o Palpation TART – Tissue/Texture changes – Asymmetry – Restricted ROM – Tenderness Check joint above and below! Muscle Strength Grading o 0/5 – No muscle movement o 1/5 – visible movement but not at the joint o 2/5 – movement at joint but not against gravity o 3/5 – movement against gravity, but not added resistance o 4/5 – movement against resistance but less than normal o 5/5 – Normal strength Neuro Exam o C5 – Biceps o C6 – Brachioradialis o C7 – Triceps o Tinel’s test – tapping over a nerve to elicit pain/radiculopathy along the nerve Inability to extend suggests need for elbow x-ray Valgus/Varus Test o Collateral ligaments o Main stabilizers Medial collateral ligament – AKA ulnar collateral ligament o Test at 30 degrees flexion Milking Test o Elbow flexed to 55, hand supinated, pull down on thumb, induces valgus stresses. Pain = positive. Moving Valgus o Elbow maximally flexed o Modest valgus torque applied until shoulder reaches its limit of external rotation o Elbow is quickly extended o Positive test = reproduction of symptoms in an arc as the elbow passes from 120 to 70 of extension Elbow Regions o Anterior Pain = biceps tendinitis – excessive elbow flexion and supination activities – anterior elbow pain with flexion and supination, weakness secondary to pain Biceps Tendon Ruptur Popeye – 97% are proximal, weakness of supination and flexion o Posterior Triceps tendonitis – repetitive extension of the elbow – throwing, hammering – pain in posterior elbow, tenderness around insertion of triceps Pain with resisted extension of elbow Olecranon Bursitis – miner’s or student’s elbow – relatively painless posterior swelling o Medial Medial Epicondylitis – golfer’s elbow Overue of wrist flexors. MCL Ulnar Collateral Sprain Most important stabilizer of valgus stresses – mainly from 20130 degrees Pitching or throwing, racquet sports Pain increases by manual valgus stress Medial Apophysitis Young children – growth plates still open Any tension stress may partially or completely tear off the medial epicondyle. Multifaceted Treatment Prevention, education, biomechanics, limiting pitches, rest, NSAID’s, rehabilitation Medial Pain – Cubital Tunnel Syndrome 2nd most common compression neuropathy behind Carpo Tunnel Syndrome Mechanical compromise of ulnar nerve o Direct insult, excessive traction, compression or friction o Clumsiness of hand o Positive Tinel’s test Tx – night splint o Lateral Nursemaid’s elbow – young children girls > boys. Axial traction on extended and pronated arm, also FOOSH. Pulls radius distally, slips through the annular ligament Arm is flexed at elbow and forearm pronated held close to body. Easily reduced in the exam room Supination and flexion Hyperpronation Sling Recurrence 26-39% Epicondylitis – Tennis Elbow Overuse of wrist extensors 10X more common than medial Rest and ice, forearm splint, rehab, omm, steroid injection - Flexor-Pronator Mass Syndrome o Purely sensory syndrome o Median Nerve becomes trapped between heads of pronator terres muscle Pain and parasthesia o Mechanism Repetitive pronation Anomalous anatomy o Resisted flexion of FDS tendon of index/middle finger Hand of the benediction - Anterior Interosseous Syndrome o Branch of the median Nerve Mostly motor syndrome – minimal or no sensory loss Weakness of loss of flexion of DIP joint or thumb index finger LECTURE 10Lab - Carrying Angle o Adduction of Ulna will cause radius to be pulled proximal – results in AB duction of wrist o AB duction of ulna will cause radius to be pushed distal, this will result in AD duction of wrist. - Interosseous membrane o Anterior Fibers Run obliquely distally and medially o Posterior Fibers Run proximally and laterally 11 – Examination of Wrist and Hand - - - - - - - Wrist Joints o Radiocarpal, radioulnar, intercarpal – RC provides most flexion/extension Hand joints o Metacarpophalangeal MCP, proximal interphalangeal PIP, distal interphalangeal DIP Examination o Look at thenar and hypothenar eminences o Look for contractures of flexor tendons – dupuytren’s o Palpate 8 carpal bones – MCP, PIP, DIP, squeeze MCP from both sides between thumb and fingers PIP – RA or Bouchard’s nodes in DJD DIP – Heberden’s or psoriasis and base of thumb in DJD Motion Testion and Maneuvers o Wrist Adduction – ulnar deviation 30 degrees – FCU Abduction – radial deviation 20 degrees – FCR Flexion – 80-90 degrees Extension – 70 degrees Finkelstein’s o Patient grasp’s own thumb, then move wrist in ulnar deviation – de Quervain’s tenosynovitis – inflammation of abductor pollicus longus and extensor pollicus brevis tendons and sheaths. Tinel’s Sign o Tapping over coarse of median nerve Phalen’s sign – hold wrist in flexion for 60 xeconds Ganglion Cyst o Soft Tissue Mass of hand wrist – most commonly the scapholunate joint o Lining herniates out of ligamentous defect causing cyst o Inflammatory process produces jelly like fluid o Positive Transillumination – may be mistaken for bony prominence Dupuytren’s Disease o Fingers become progressively flexed at the MCP and PIP joints Diabetis, Smokers, Alcoholics Kienbock’s Disease – idiopathic avascular necrosis – Lunate - MRI o Repetitive compressive forces o Vascular impairment o Presents w/ vague aching wrist pain, stiffness o Dominant wrist, men 20-40 y/o, women later in life o Stages I-IV I – acute stage – indistinguishable from wrist pain, symptoms abate II – change in density of lunate, but size, shape, configuration are normal; pain and swelling due to reactive synovitis III – increasing wrist stiffness, collapse of lunate, proximal migration of capitate and disruption of carpal architecture IV – further degenerative changes present in carpal 12 – OMT for Non-Surgical Forearm, Wrist and Hand Somatic Dysfunctions - Allen’s Test for Carpal Tunnel Syndrome o Tests radial/ulnar artery insufficiency Pt rapidly open and lose fist then hold it closed Occlude ulnar and radial artery Open fist and release one artery –look for pink Positive is poor return of color.