Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
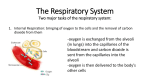
BIO 161 – Respiratory - Answers T Dic Charge – Winter 2008 Review Worksheet 1) Can you name, in order, the major structures by which air passes as it makes its way into the lungs (that is, all the way to the alveoli)? Nostrils – Nasal cavity – Pharynx (naso-, oro-, pharyngo-), larynx, trachea, bronchi (primary, secondary, tertiary), bronchioles (primary, terminal, respiratory), alveoli 2) The structures known as the nasal conchae are found in the nasal cavity. What functions do they perform? These scroll-like folds increase surface area and turbulence of inspired air and therefore increase trapping of particulate matter in inspired air humidification of inspired air warming of inspired air 3) What are the three pairs of salivary glands called, and where are they found? Parotid glands – found anterior to the ear on the lateral surface of the face. Sublingual glands – found inferior to the tongue at its base, where it attaches to the floor of the mouth. Submandibular glands – found below the mandible lateral to the sublingual glands. 4) The junction at which the trachea divides into the primary bronchi is called what? The carina 5) The epithelial layer lining the sinuses, the nasal cavity, the pharynx, the trachea, and the bronchi is what kind of epithelium? Pseudostratified ciliated columnar epithelium 6) Name all the paranasal cavities (sinuses), in order from largest to smallest. Maxillary – 10-20 ml Sphenoid – 7-9 ml Frontal – 6-7 ml Ethmoid – Did you know? The ethmoid and maxillary sinuses are the first to develop and are visible even in newborns, but that the sphenoid sinuses don’t develop until about the age of six, and the frontal sinuses are not fully developed until about the age of 12. Their communication with the nasal cavity is also incomplete until those ages. 7) What is the connection from the nasal cavity to the larynx called and what 3 divisions exist? In each division, what normally is expected to travel in that tube? The pharynx is a funnel-shaped tube running from the back of the nasal cavity past the opening of the oral cavity and down to the top of the larynx. Each region is named according to the adjacent structure. The nasopharynx usually only carries respiratory gasses. The oropharynx usually carries both food and water and the respiratory gasses, as does the laryngopharynx. 8) The pharyngotympanic tubes connect what two places in the head? What is their purpose? What 2 other names are they known by? Also known as the Eustachian tubes or simply the auditory tubes, they connect the middle ear to the nasopharynx and thus allow the equilibration of the pressure in the middle ear with that outside the tympanic membrane. 9) Name 4 cartilages and 3 purposes of the larynx? From largest to smallest, the cartilages are the thyroid, cricoid, arytenoid, and the corniculate cartilages. The 3 purposes of the larynx are: To provide the voice To separate food and water from air (this includes protection to the glottis so that food does not usually enter the trachea) To provide a patent airway 10) What is the epiglottis? How does swallowing work? The epiglottis is a flap of elastic cartilage that is depressed by food as it is swallowed, covering the glottis and preventing food from entering the airways. In swallowing, the larynx is lifted by muscles attached to the hyoid bone superiorly, and moved slightly anteriorly to better ensure that the epiglottis fully blocks the entrance to the larynx. See this link for a good diagrammatic movie: http://www.linkstudio.info/images/portfolio/medani/Swallow.swf 11) Can you label the following diagram of the larynx? A-D are cartilages, the rest are other structures you should know. A Thyroid Cartilage E Hyoid Bone B Cricoid Cartilage C Corniculate Cartilage D Arytenoid Cartilage F Epiglottis G Vocal cords H Trachea or tracheal cartilage 12) How is the voice produced and what causes changes in pitch and in loudness? The glottis is opened partially so that expired air causes the vocal chords to vibrate. By tightening the chords using laryngeal muscles attached to the arytenoids cartilages, pitch is increased/elevated (sound note gets higher). Volume/loudness is adjusted by how much air is allowed/forced out of the lungs via the glottis. 13) Identify all of the branches of the respiratory tree from the trachea down to the alveoli in the alveolar sacs. For this tree, identify what part is the conducting zone (define conducting zone) and what part is the respiratory zone (define). Indicate what the endothelial layer tissue type is at each level of branching and whether cartilage is present. Trachea divides at the carina into the 2 main/primary bronchi, 1 each to the left and right lungs. The primary bronchi branch into the secondary bronchi as each enters a lobe of the lung – left has 2 secondary bronchi to two lobes, right has 3 secondary bronchi to three lobes. Secondary branch into tertiary bronchi, which then divide into primary and then terminal bronchioles. Cartilage is present up until the level of the primary bronchioles fall below about 1mm in diameter, at which point it disappears. Up to and including the 2nd (terminal) level of bronchioles, PSCCE (Pseudostratified Ciliated columnar epithelium) is the endothelial layer, and this marks the end of the conducting zone (carries gases into/out of the lungs, without incurring any gas exchange with the blood). Beyond this point, we are in the respiratory zone (gas exchange can/does occur – defined by presence of alveoli) and we have simple cuboidal epithelium in the tubes and simple squamous (diffusion of resp. gases) and cuboidal (secretion of surfactant) in the alveoli. Terminal bronchioles branch into respiratory bronchioles, which branch to alveolar ducts (both support sparse alveoli) and then terminate in alveolar sacs (a cluster of alveoli). 14) For the secondary bronchi, indicate the count on both sides of the thoracic cavity and indicate why this count is so (as in, what does the count of these airways match as far as lung structure?). 3 right – into 3 lobes (1 EACH) 2 left – into 2 lobes (1 EACH) 15) Please place the following labels on the diagram of the lungs below. Hilum, Apex, Costal surface, Cardiac notch, Base. As well, please draw and label both sides of a pleural sac on the diagram, and indicate where the pleural cavity is found. as per your notes – the pleural cavity lies between the visceral (on the organ) and the parietal (towards the cavity walls) pleura. 16) Describe 3 changes in lung function that are a result of aging. Kyphosis – curvature of the spine may reduce respiratory volume Osteoporosis - calcification of cartilage reduces compliance (flexibility) of chest wall Respiratory muscles weaken decreasing elastin reduces compliance of lung and it’s recoil alveoli increase in size - reduces the surface area to volume ratio # of cilia reduced # of macrophages reduced 17) What is RDS (a.k.a. HMD)? Respiratory Distress Syndrome (Hyaline Membrane Disease) represents damage done to the lung tissues by mechanical ventilation (use of a ventilator). Lungs are less compliant and harder to inflate, causing respiratory distress of the newborn 18) What two areas of the brainstem are responsible for control of respiration? Name the areas within each, and indicate how they control respiration. Could you label a diagram? Pons apneustic area increases inspiration pneumotaxic area decreases inspiration Medulla Ventral respiratory group (VRG) – moderates forceful inspiration and expiration by influencing changes in DRG Dorsal respiratory group (DRG) – regulates normal/relaxed breathing – pacemaker 19) What are the three areas of chemoreception in the body with regard to respiration, where are they located, and to what chemistry to they respond? What change results from the changes they detect? Central chemoreceptors – in medulla adjacent to VRG - respond to rising CO2 indirectly – as CO2 enters medulla, dissolves in CSF to form H+ - response is to H+ (increasing H+ results in increasing depth and rate of respiration) Peripheral chemoreceptors Carotid – at junction of internal and external carotids - respond to rising CO2, rising H+, and VERY LOW O2 – each causes increasing rate and depth of respiration Aortic – on the aortic arch – respond only to gases – rising CO2 and VERY LOW O2 – results in increasing rate and depth of respiration 20) What other signals inform the brain of the need for increased respiration? Proprioceptors provide information that joints are in motion Stretch receptors in the muscles provide information that muscles are active. Both indicate that metabolic needs are increasing (muscle is using more energy and so inform the respiratory centre (the VRG) to increase breathing. Note that this information initiates respiratory increases even before blood gases begin to inform the chemoreceptors of that requirement. 21) By what nerves do the peripheral chemoreceptors communicate with the medulla, and to which control centre do they transmit their information? Carotid – via Cranial Nerve IX – Glossopharyngeal – to the VRG Aortic – via Cranial Nerve X – Vagus – to the VRG 22) Via what nerves are the muscles controlled for inspiration? Name the muscles. T1-T11 – the intercostal nerves innervate the external intercostals C3-C5 – the phrenic nerve innervates the diaphragm 23) What is the Hering-Breuer reflex? What nerve carries the information to what structure in the brainstem? Stretch receptors in the smooth muscles of the lung (along the bronchi and bronchioles) inform the pneumotaxic centre of the Pons via the Vagus nerve to cut off inspiration during large inspirations. Prevents over-inflation of the lung. Not active in adults during normal breathing but is thought to be active in infants, at least initially, during normal breathing. Probably active in adults during exercise, or with COPD (with air trapping), when normal tidal breathing results in inflation of the lungs above normal levels of tidal breathing. 24) During normal breathing, indicate what phases of respiration are active or passive, and how long (on average) each phase endures. Inspiration – active – involves contraction of diaphragm and external intercostals – lasts ~ 2 sec. Expiration – passive – elastic recoil of the chest wall and the elastin around the alveoli causes air to leave the lungs. – lasts ~3sec 25) What muscles are activated during active/forceful expiration? internal intercostals 26) Explain what HAPE and HACE refer to and describe what is happening when they occur. At high altitude (HA) you have pulmonary edema (HAPE) or cerebral edema (HACE) – extremes of high altitude sickness. Both result for the lower pressures at high altitude that result in leakage of fluid into the lungs or around the brain, respectively. HAPE results in severe respiratory limitations and can result in Hemoptysis (coughing of blood). HACE can lead to reduced cognitive abilities, coma or even death 27) What treatments exist for HAPE and HACE? Dexamethazone is an anti-inflammatory intended to reduce the irritation in the lungs the precedes HAPE Diamox is a diuretic taken as a prophylactic (preventative) measure prior to ascent. It causes loss of HCO3-, which stimulates breathing (metabolic acidosis) 28) Name 3 normal longer term adaptations when one acclimatizes to higher altitudes. EPO (Erythropoietin) is released by the kidney and results in increased production of RBCs Lung capillary density increases Muscle capillary density increases New alveoli are produced in the lung 29) Explain what the “bends” are in relation to deep diving. The greater pressure at depth induces more nitrogen to enter the tissues. This is a relatively slow process, so occurs only over extended diving at depth. The release of pressure as the diver ascends has to be slow enough to allow the nitrogen to diffuse out of the tissues without forming bubbles – if bubbles form, they may cause an embolism in arterioles or even arteries, resulting in ischemia (lack of blood flow) to tissues. Permanent damage may result to sensitive (nonregenerative) tissues (brain or myocardium) and painful muscle cramps cause the distorted, bent configuration of the body of a “bent” diver. treatment usually involves repressurizing the diver in a hyperbaric chamber to force the bubbles smaller and to re-enter the tissue, and the slowly decompressing to allow time for the nitrogen to diffuse without bubble formation. 30) 31) Please draw and label, with appropriate volumes, a spirogram. In addition to the four fundamental volumes, indicate two capacities that are the sum of 2 or more of the volumes. the 4 volumes are Residual Volume (RV - 1200ml) , Expiratory Reserve Volume (ERV – 1200ml) Tidal Volume (TV – 500 ml), and Inspiratory Reserve Volume (3100 ml) – Total lung capacity is the sum of all 4 (6000 ml). Vital capacity is the volume of air that can be moved in and out of the lung with maximal effort (TV + ERV + IRV = 4800 ml See the diagram in your notes or text for the proper labeling. 32) What is Bronchial Asthma? Describe the 4 factors that make bronchial asthma a disease that limits air movement in the lungs. An immune response in the lungs results in hypersensitive airways that result in: mucus accumulation in the lumen the epithelial layer swells with edema due to inflammation the smooth muscle layer is grown larger and thicker (reducing lumen diameter when contracting due to irritation (bronchoconstriction) Increased size and number of goblet cells increases mucus production Treatment modalities now include treatment of the underlying inflammatory response, rather than just using bronchodilators that target the symptoms 33) What is COPD and what are the results? A constellation of diseases that result in air-trapping with the lung, hyperinflation and diminished flow through the airways. Smoking is the number one contributor, but may also result from chronic bronchial asthma, chronic bronchitis, or emphysema. alveoli are damaged and non-functional in gas exchange. reduced # of functional alveoli increased # of dead air spaces that don’t communicate with the outside (never exchange with fresh air) reduced capillary network in lungs long-term hyperinflation results in a barrel chest 34) Describe a pulmonary embolism, how it happens, what happens, and what the consequences are. What is a saddle embolism? A clot, usually from the leg veins but can also result from arm veins or even from with the heart itself, travels up to and through the heart and travels into the pulmonary circulation, eventually lodging where it is larger than the vessel through which it is traveling (artery or arteriole) and resulting in a loss of blood flow through that vessel. Results in loss of gas exchange in that area of the lung (blood isn’t getting to those alveoli) and, if not treated, death of the pulmonary tissue. If the vessel is large enough, it may result in death, but is most often not fatal. Results in Dyspnea (shortness of breath), higher heart rate (tachycardia) and pain which may be localized to the chest or may radiate down the arms or up the neck. Treatment with “clot-busters” (anti-clotting medications) can be successful. A saddle embolism is one in which the clot (embolus) blocks both branches of an artery as it divides. If it is at the level of the pulmonary trunk as it branches to left and right pulmonary arteries, it is a cause of sudden death. 35) Be aware of the health factors that smoking impacts, and the progression of improvements if one quits (from page #17 in your notes) 36) Define or describe the following terms: a) Hypoxia low oxygen in the tissues b) Hypoxemia low oxygen in the blood specifically c) Hypercapnia high levels of carbon dioxide in the tissues d) Dyspnea difficulty breathing or shortness of breath e) Apnea absence or lack of breathing f) Eupnea normal breathing g) Cyanosis blue appearance of tissue (the lips esp.) due to hypoxemia h) Laryngitis inflammation of the larynx i) Lysozymes enzymes found in the mucus secretions of the respiratory tract that actually cause lysis of bacterial cells that are inspired and caught on the mucus membranes j) Defensins enzymes that are also found in the same mucus secretions that attack viral invaders of the respiratory system k) glottis – opening to trachea between the vocal folds (chords) l) Rima glottides opening between arytenoids cartilages in larynx – incompletely covered by epiglottis during swallowing m) Valsalva maneuver increasing abdominal pressure (as in birthing or defecating) by tensing abdominal muscles and making expiratory efforst while holding breath (glottis is voluntarily closed) – can also stabilize lower spine during weight lifting – potentially dangerous due to increase in blood pressure (over 300 mm Hg possible) – best to allow some breathing and only partially close glottis n) laryngitis inflammation of the larynx – often involves loss of voice as vocal chords are inflamed and therefore do not vibrate normally o) influenza an upper respiratory viral infection characterized by sudden onset of a high fever, headache, body aches – does not involve GI effects (no diarrhea or vomiting) p) laryngoscope an endoscope designed to examine the larynx q) surfactant produced by type II (cuboidal) cells in the alveoli, this phospholipid reduces surface tension of the moist endothelium of the alveoli and prevents alveolar collapse r) Hemoptysis coughing of blood