Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Sexually transmitted infection wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Hepatitis C wikipedia , lookup
Oesophagostomum wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
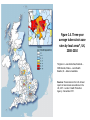
IOSH Presentation 2012 Tuberculosis Kim Cartlich 2012 Aims • Basic awareness of Tuberculosis (TB) • Gain knowledge of the disease process • Be aware of local epidemiology / prevalence • Recognise why TB is making a come back •To understand the role of BCG vaccination and who requires it • Know the role of the TB nurse • Where to seek advice What is TB? •TB is an airborne communicable disease •TB is caused by a bacteria called mycobacterium tuberculosis •It is spread by tiny airborne particles expelled by individuals with infectious TB by cough, sneeze or spit •If another person inhales air containing these bacteria transmission can occur •TB bacteria prefer the lungs but can infect any organ in the body TB History •Consumption •Galloping consumption •Scrofula •Kings Evil •White plague •Phthisis Famous people who had TB •Bronte sisters •Robert Burns •George Formby •Desmond Tutu •Eleanor Roosevelt •Vivian Leigh •Tom Jones •Nick Knowles “It was the fashion to suffer from the lungs; poets especially; it was good form to spit blood after any emotion that was at all sensational, and to die before reaching the age of thirty.”Alexandre Dumas Past treatment for TB 2010/2011 TB Global facts • • • • 1.7 million people died from TB in 2009 This is equal to 4700 deaths per day There were 9.4 million new TB cases in 2009 In 2010 the WHO reported the highest ever rates of MDR TB, with peaks of 28% in some settings of the former soviet Union • XDR TB cases have been confirmed in 58 countries However ! • 2008 saw the highest level ever of people successfully treated at 86% World Health Organisation 2012 Why the resurgence? • Migration • Poverty / war / civil unrest • HIV • Longevity • Poor treatment and control in third world countries Figure 1.4. Three-year average tuberculosis case rates by local areas*, UK, 2008-2010 *England – Local Authorities,Scotland – NHS Boards, Wales – Local Health Boards, NI – data not available. Sources: Tuberculosis in the UK: Annual report on tuberculosis surveillance in the UK, 2011. London: Health Protection Agency. December 2011. Figure 1.3. Tuberculosis case reports and rates by region, England, 2010 Number of cases 3,500 50 Rate (per100,000) and 95% CI 45 41.9 40 2,500 35 30 2,000 25 1,500 1,000 20 16.0 11.9 15 12.0 11.1 8.8 500 10 8.2 5.4 0 5.3 5 0 Region CI – Confidence interval Sources: Enhanced Tuberculosis Surveillance (ETS), Office for National Statistics (ONS) midyear population estimates. Data shown in Appendix B; ii, iii. Prepared by: TB Section - Health Protection Services, Colindale. Rate (per 100, 000) Number of cases 3,000 10,000 15 14 13 12 11 10 9 8 7 6 5 4 3 2 1 0 9,000 Number of cases 8,000 7,000 6,000 5,000 4,000 3,000 2,000 1,000 0 2000 2001 2002 2003 2004 Number of cases 2005 Year 2006 2007 2008 2009 Rate per 100,000 and 95% CI CI - Confidence interval Sources: Enhanced Tuberculosis Surveillance (ETS). Enhanced Surveillance of Mycobacterial Infections (ESMI). Office for National Statistics (ONS) mid-year population estimates. Prepared by: TB Section - Health Protection Services, Colindale. 2010 Rate (per 100, 000) Figure 1.1. Tuberculosis case reports and rates, UK, 2000-2010 511 157 121 125 281 194 286 47 115 519 353 322 553 361 488 71 124 73 69 2,713 194 208 27 35 1,837 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 5,504 Percentage of cases* Figure 1.6. Tuberculosis case reports by place of birth and region/country, UK, 2010 Country/Region (% where place of birth known) Non-UK-Born UK-born *Numbers of cases stated in bars Sources: Enhanced Tuberculosis Surveillance (ETS). Enhanced Surveillance of Mycobacterial Infections (ESMI), Office for National Statistics (ONS) mid-year population estimates. Prepared by: TB Section - Health Protection Services, Colindale. How is TB caught • TB bacteria inhaled • Most lodged in the upper respiratory tract (70-90%) • Some may reach the lungs and multiply (10-30 %) • 2-10 weeks after infection immune system usually intervenes and prevents spread of infection (latent) • Only 10 % will go on to develop TB at some time in their life time Signs & Symptoms of TB • Cough • Weight loss • Night sweats • Chest pain • Extreme tiredness and lethargy • Coughing up blood TB Treatment •TB treatment in the UK is free to the patient •Medication is taken for minimum of 6 months •Key to cure is concordance •Occasional side effects •Closely monitored •Poor concordance can result in drug resistance •Drug resistant TB is much more difficult to treat and much more expensive Who is at risk of catching TB? •Elderly •The very young (under 2yrs) •Those with weakened immune systems e.g. HIV •Pre existing lung conditions •Homeless / alcoholics / Drug addicts •Travel to a high risk area i.e.. more than 3 months •New entrants to the country from high risk areas are most at risk in the first 3-5 years of settling in their chosen country of reactivating any latent TB MDR TB and XDR TB Multi drug resistant TB Extensively drug resistant TB • Poor treatment compliance • Single drug therapy • Poor calculation or regimes • Malabsorption of drugs • Prescribing / dispensing errors Map showing MDR TB 2010 Why the problem • Gaps in TB control • Extremely weak services M/XDR-TB • management and care • Health workforce crisis • Inadequate laboratories • Quality of anti-TB drugs not assured • No restriction or regulation of anti-TB drug use • Absent infection control • Insufficient research • Major financial gaps How to protect against TB There is no 100% protection against TB • • • • BCG vaccination affords some protection ,for high risk groups Knowledge about the disease is the best defence Knowing who to contact for advice Seeking professional advice if you know you have come in contact with a case of TB • Promote general good cough hygiene Remember ! TB is not as infectious as you think The TB team TB Clinicians TB Nursing Team HPA TB Incident , What to expect Incident involving large numbers i.e. educational, establishment, nursing residential home ,prison , factory • Health protection agency lead • Incident meeting is held , all relevant parties invited all information is assessed. • Plan of action –timetable, screening , communication , press statements, • TB nurses screen, collate results inform HPA • Further meeting to assess need for further screening • Final outcome meeting The role of the TB nurses • To support and visit all newly notified TB patients • To instigate TB contact tracing • Hold TB screening clinics in the community and Hospital setting • Provide nurse Led prophylaxis clinic • To provide a BCG vaccination service • To screen new entrants from high prevalence areas of TB • To and act as a resource for information on TB Useful contact numbers North Yorkshire & Humber Health Protection unit 01904 468900 TB Nursing Team CHCP 01482 617994