Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Infection control wikipedia , lookup
Lyme disease microbiology wikipedia , lookup
Bacterial morphological plasticity wikipedia , lookup
Human microbiota wikipedia , lookup
Gastroenteritis wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Schistosomiasis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Globalization and disease wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Germ theory of disease wikipedia , lookup
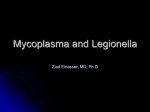
FUN2: 11:00-12:00 Monday, November 10, 2008 Dr.Waites Microbiology Scribe: Joan-Marie Manolakis Proof: Andrew Richardson Page 1 of 5 I. Introduction Mycoplasmas and Fastidious Gram-negative bacteria [S1]: II. Objectives [S2] a. Review and discuss: b. Microbiological characteristics c. Epidemiology d. Virulence Factors e. Associated diseases f. Laboratory Detection Of: g. Haemophilus h. Bordetella i. Mycoplasma j. Ureaplasma k. Legionella III. Haemophilus [S3] a. Haemophilus means “blood loving.” Blood is necessary for it to grow properly. b. Gram-negative coccobacillus. c. They are facultative anaerobes. d. Non-hemolytic-lack the enzymes to break open the red blood cells. e. They primarily invade the body through the respiratory tract. f. Non-encapsulated forms that may be forms of the respiratory flora of the upper respiratory tract. The encapsulated have more virulence there. g. Haemophilus: Pathogenesis[S4] i. They can be spread person to person through aerosol. ii. If you have underlying lung disease, like chronic obstructive pulmonary disease due to various causes (primarily smoking), you can get an exacerbation of bronchitis there so the organisms start growing and making more symptoms. It’s an endogenous infection from the bugs in the body. iii. The antiphagocytic capsule is the major virulence factor. 1. 6 capsular serotypes (a-f) 2. Type b causes the most disease-vaccine is made against it iv. Contains endotoxin which causes damage to the respiratory epithelium so it can spread through the blood stream, and it may go to the brain and cause meningitis. It does not produce exotoxins. v. Has an IgA protease so that it can bypass the immune system in respiratory secretions vi. 30% produce beta-lactamase h. Detection: H. influenza [S5] i. Grown in the lab on chocolate agar ii. Generally will not grow on blood agar because it’s non-hemolytic and can’t open the red blood cells to get what it needs. iii. Two things it needs are the X factor (hemin) and V factor (NAD)-in chocolate agar, they are both there. iv. It is capnophilic- needs additional CO2 to grow in the lab v. Use X or V to determine which species you are dealing with. There are several types of Haemophilus. To determine if an organism requires both of the co-factors, put them on an agar plate, put a filter paper strip with a V or X or combination, and if the organism only grows around the strip that contains both factors there, you know it’s H. influenzae. vi. Satellite formation- Put on a hemolytic strain and then put it on a blood agar plate, streak around the plate with organism, the H. influenzae will grow around the S. aureus and release the X and V factor for it. IV. Diseases: H. influenza [S6] a. The encapsulated form causes diseases: i. Otitis media in kids ii. Sinusitis iii. Bacteremia-blood stream infection iv. Epiglottitis-inflammation of the epiglottis-most important cause in kids v. Cellulitis-child with the swollen face vi. Laryngotracheobronchitis vii. Meningitis-previously a major cause of meningitis in kids viii. Community acquired pneumonia ix. Conjunctivitis-bacterial inflammation of the eyes is important V. Prevention: H. influenza [S7] FUN2: 11:00-12:00 Scribe: Joan-Marie Manolakis Monday, November 10, 2008 Proof: Andrew Richardson Dr.Waites Microbiology Page 2 of 5 a. This was previously a problem in kids because children under the age of 5 lacked the protective antibody against the capsule of type b. b. A vaccine against the polysaccharide capsule of type b is conjugated with a protein to make it more immunogenic in young kids (don’t make antibodies against the polysaccharide antigens without protein adjuvant). They get a series of injections in early infancy. c. The vaccine reduced the invasive disease by about 90%, so now Haemophilus meningitis is rare. d. The vaccine is only against type b, so nonencapsulated forms haven’t changed. It still can occur as a pathogen in respiratory infections. e. It still causes ear infections and sinus infections-they’re in the in-typable strains f. Epiglottitis is almost completely gone now-vaccines have impacted greatly VI. Other Haemophilus [S8] a. H. dureyi-causes chancroid (also called a genital ulcer) and is not as common as Chlamydia b. H. aegyptius-also a cause of conjunctivitis. It’s an important cause of bacterial conjunctivitis, so optometrists need to make note of that. VII. Bordetella pertussis [S9] a. Gram negative b. Agent of whooping cough c. Encapsulated coccobacilli-look like H. influenza d. Slow-growing e. Fastidious f. Strict aerobe g. Does not ferment carbohydrates but does oxidize amino acids VIII. B. Pertussis: Whooping Cough [S10] a. Previously had a high amount of morbidity and mortality in kids b. Reduced because of the vaccine c. 5-21 day incubation-very contagious d. Acquired in the respiratory tract and travel to the posterior pharynx and multiply on the pharyngeal epithelium. e. There are three disease stages after incubation i. Catarrhal stage-cough and sneeze period, while it’s getting revved up ii. Paroxysymal stage-a lot of necrosis in the epithelium of the upper airway and because of the toxins and their affect on the local epithelium, you cough. It is called paroxysmal because you cough very fast and can’t catch your breath. When you take a breath in between the coughing, there’s a whooping sound (deep breath between peroxisms of coughing). iii. Convalescent stage-several months of coughing while the epithelium regenerates. f. Lymphocytosis-develop antibodies against it, so you shouldn’t get it again IX. Pertussis Epidemiology [S11] a. It’s been known for a long time, dating back to Europe in the 16th century, describing people with these conditions. b. Vaccines are mandatory for kids to go to school. c. In 2001, >285,000 died worldwide d. In 2005, > 25,000 cases in the US, making it fairly common e. No environmental or animal reservoir, it’s just person to person f. Adolescents and adults are over half of the cases. g. Older persons often spread to children. X. Pertussis in Alabama [S12] a. Shows the data of reported cases b. It increases in 2005 with 82 cases XI. Reasons Pertussis is increasing [S13] a. Reasons why it’s increasing: i. Under-vaccination in infants-illegal immigrants don’t typically get vaccinated because they lack insurance and money ii. Under- or misdiagnosis-when it’s missed, the person can spread it from person to person iii. Vaccines in the past protect you while you’re little, but in the adult years, the antibodies begin to wear off and aren’t protected any longer. 1. Example: pediatric resident caught Pertussis from the child that she was treating because her immunity wore off. She had a bad case. iv. Adolescents and adults with worn-off immunity are a reservoir for the disease. They can spread it to young infants that are at risk and haven’t finished the vaccination series. XII. Pertussis Pathogenesis [S14] FUN2: 11:00-12:00 Scribe: Joan-Marie Manolakis Monday, November 10, 2008 Proof: Andrew Richardson Dr.Waites Microbiology Page 3 of 5 a. Bacteria get into respiratory tract, and the virulence factors are primarily these attachment mediators (FHAfilamentous hemaglutinins and Pertussis toxin). When it attaches and allows replication, it tries to block the host system from getting rid of it. It impairs the chemotactic mechanisms for white blood cells being drawn to the site. The toxins cause local tissue and systemic effects by damaging the cells where the bacteria are growing. XIII. Pertussis Toxins [S15] a. These toxins help it attach: i. Increase cAMP, inhibit phagocytic migration, inflammation and necrosis of cells, killing respiratory epithelium, stimulating the release of cytokines like IL-1, LPS endotoxin stimulate cytokines and activates alternative complement XIV. B. Pertussis: Detection [S16] a. Collect a Nasal Pharyngeal swab and put it on Bordet-Gengou or Regan-Lowe charcoal media, incubate it, and if it’s grown it can be detected by fluorescence. This is done primarily in public health labs. b. You should measure antibody titers and CDC recommends that PCR should be done in addition to culture. c. Can look for antigens in secretions with fluorescent antibodies, but you need a large number of organisms to be positive. d. SQ: Is PCR used as confirmation or just a recommendation? A: It’s recommended by the CDC. They want antibody-susceptibility tests done so they can determine if any resistance is developing. It is an important public health concern, so the PCR (being that it’s much more sensitive) should be done. The recommendation is to do both. XV. Pertussis Prevention [S17] a. The old vaccine was the vaccine that had killed organisms given with the series of diphtheria and tetanus toxoids. It begins in early infancy through childhood. It had side-effects, and the antibodies disappeared by late adolescence. In late 1996, a new vaccine, the accellular vaccine (DaPT), was introduced. It includes antigens for various toxins, including the fimbriae. They help them mediate disease. The antibodies that you get from taking the vaccine prevent them from attaching. If they can’t attach, they can’t cause disease. b. This series given is the first vaccine group started: 2 mo, 4 mo, 6 mo, 15-18 mo, and 4-6 yr (a final booster to put the immune system in high gear). c. Now the Tdap, introduced in 2005, is for ages 11-64 years. A single dose of it will boost up the immunity you may have lost as the old one wears out. d. Td-recommended every 10 years e. SQ: Do you think that the doctor that had Pertussis would have been okay if she’d had this new vaccine? A: I can’t say. It was years ago. That’s what it’s supposed to do. The old vaccine was Pertussis bacteria grown up and killed. Though they were dead, they had their antigens on them so it’d stimulate the immune system. It wasn’t a concentration of the disease-mediated antigen as the new one is. It now stimulates the immune system directly against the part of the bacteria that is causing disease. The old was good for kids, but when more people weren’t vaccinated and people with worn-off immunity (who were more susceptible and could contract it more easily) they were spreading it. We’ll see how it goes. Kids can’t go to school without their vaccines, but there’s nothing to make adults do it. There are fewer than 100 cases in Alabama, but it’s still there. XVI. Legionella pneumophila [S18] a. Fastidious b. Catalase-negative c. Facultatively intracellular gram negative rod d. It doesn’t ferment carbohydrates e. Doesn’t stain on a gram stain- often not seen in body fluids f. Over 30 species and multiple serogroups g. One of the causes of community acquired pneumonia h. Those named for community acquired pneumonia: i. Streptococcus pneumonia ii. Moraxella catarrhalis iii. Haemophilus influenza iv. Legionella pneumophila i. Story of naming: American Legion veterans were in Pennsylvania (WWII veterans). Many smoked and had impaired host defense. They got severe pneumonia and some died. They had inflammation in their lungs, but no bacteria could be grown in culture. The CDC detected it and grew it. It was named after the American Legion men and pneumonia. It was growing and multiplying in the air conditioning cooling towers, being piped through the air vents, aerosolizing multiple people. It spreads from water sources. Hospitals and the dental school must check their water supplies for this bacteria. In the summer it is typically worse. FUN2: 11:00-12:00 Scribe: Joan-Marie Manolakis Monday, November 10, 2008 Proof: Andrew Richardson Dr.Waites Microbiology Page 4 of 5 j. Pathogenesis of Legionellosis [S19] k. It is inhaled and complement deposits on bacteria. The bacteria bind macrophage C3 receptors and are taken up by macrophages in the lungs. They prevent the fusion of the phagolysosome and thus aren’t killed when taken up. They multiply in the macrophage. Then they’re released when the bacteria release enzymes, and they go on to infect other cells. l. This type of pneumonia is different because it’s not contagious from person to person. It’s a point-source outbreak, and many people can be infected at one time. m. You can get an acute purulent pneumonia and abscesses. XVII. Legionella Culture [S20] a. It may be grown in the lab but will be done with a special buffered charcoal yeast extract agar culture. Agglutination or immunofluorescence will be used to identify the species. b. Legionella Detection [S21] i. Can stain tissues from lung biopsies, do a direct fluorescent antibody (poor sensitivity so not often done), urine polysaccharide antigen, serology (IFA-paired sera required), and now we can use PCR (it’s slowgrowing and is difficult to grown, an atypical pathogens… others examples of atypical pathogens include Chlamydia pnuemoniae, Chlamydophila, Mycoplasma XVIII. Legionares Disease [S22] a. Cultures are important because it’ll actually pick up all the different species. b. 5-10% of community acquired pneumonia and about 20,000 cases each year in the US c. Systemic spread may cause nausea, vomiting, and diarrhea d. Older men with underlying lung disease and anyone that’s immunosuppressed (transplant recipients) e. Associated with air conditioning that don’t properly clean tank, so it’s more likely in the summer months. f. Prevention of Legionellosis [S23] i. No vaccine exists ii. Cell-mediated immunity more important than antibody-mediated iii. Identify sources and eliminate them XIX. Moraxella catarrhalis [S24] a. Related to Neisseria b. It’s an important cause of respiratory conditions, otititis, pneumonia, sinusitis c. Gram-negative coccus d. Grow regularly on blood agar-not as fastidious as Neisseria e. Many kids may carry it in the upper respiratory tract f. Causes bronchitis, pneumonia, sinusitis g. Most of them produce beta-lactamase so you can’t treat them with ampicillin XX. Mycoplasma Pneumoniae (his favorite) [S25,S26] a. It’s an important cause of respiratory disease in the US. b. This cartoon shows the relative size comparisons and appearances of different organisms. i. Streptococcus is about a micron. XXI. Mycoplasma [S27] a. Mycoplasma is the smallest bacteria-it’s about tenth the size of a streptococcus. They are the smallest free-living organisms (free-living: smallest bacteria that can be cultivated on artificial media). b. There are close to 200 species described with only 20 in humans. c. They cause plant diseases and are carried by insects (also occur in animals and affect the health of all of these categories). d. They have the smallest genome, only about 687 genes compared to 4,000 or so for E.coli or Streptococcus. e. They lack a cell wall. f. Don’t mix up with Mycobacteria- they’re acid-fast organisms. g. Both evolved from gram-positive bacteria, and the Mycoplasmas were derived through evolutionary degeneration. They can’t make cell wall anymore. h. They have a specialized cell membrane-must provide them with sterols for their cell membranes. i. Usually reside on extracellular mucosal surfaces of the respiratory tract or the lower genital tract. It may also reside inside cells. XXII. M. pneumoniae: Pathogenesis [S28] a. Causes walking pneumonia. b. It’s slow-onset condition c. If you inhale the Mycoplasma- it’s spread slowly from person to person (college dorms, military camps, kids bring it home to the household, etc.) d. When it’s inhaled, it has a specialized attachment mechanism on the tip so it can attach to the respiratory tract. Our bodies make antibody to protect against it. The organism’s variance allows it to change its antigens so you FUN2: 11:00-12:00 Scribe: Joan-Marie Manolakis Monday, November 10, 2008 Proof: Andrew Richardson Dr.Waites Microbiology Page 5 of 5 can get it over. When it’s in the lung and is attached, it releases H2O2 which damages the cell. It releases other enzymes and hemolysins that cause cilia to stop beating. It affects the metabolism of the cell, and has a toxin that’s been identified called the Community Acquired Respiratory Disease toxin. When it attaches, it induces inflammation and stimulates white cells to come there and stimulates cytokine production. The local inflammation causes coughing. You cough until your chest hurts and is sore. e. Walking pneumonia-you feel bad with various symptoms (scratchy sore throat, headaches, runny nose, itchy eyes, otitis, etc.) but you go on to school while you’re sick. You feel bad but not enough to stay in bed. f. You stimulate autoantibodies-some people get hemolytic anemia or encephalitis in the brain (severe cases), glomerulonephritis, skin lesions, rashes, etc. XXIII. Mycoplasma Detection [S29] a. Grown on SP4 agar but is slow growing (generation time is 6 hours) b. Hydrolyzes glucose c. Diagnosed by antibody testing and PCR d. Ab-testing is problematic: a positive IgM test means you have Mycoplasma. There are two problems: i. If you get past childhood with several infections, your body stops making IgM. ii. IgM or IgG may hang around for several weeks or years (IgG), so a positive antibody test is hard to do. iii. IgA can be measured, and sometimes it’s good but not any better than IgM. e. So, culture takes three weeks, antibodies (need two sera), PCR can be done (it’s the best but is expensive)… thus, most of the time there is no diagnosis made, they just treat for it. Unless you have repeated spells of it, often you don’t know if you have it. XXIV. M. Pneumoniae Disease [S30] a. Tracheobronchitis, walking pneumonia- up to half of the community acquired pneumonia may be due to Mycoplasma b. Similarity to other pneumonia make it hard to differentiate the two c. Once thought to be a disease of school-aged, high school and college kids d. Kids in daycare take it home now to their grandparents. e. Perhaps it plays an important role in wheezing and asthma-can make it worse XXV. Other Mycoplasmas [S31] a. Mycoplasma hominis b. Mycoplasma genitalium c. Ureaplasma species XXVI. Diseases due to Genital Mycoplasmas [S32, S33] i. Commensals in lower urogenital tract in normal sexually active adults. They don’t always cause disease. b. M.genitalium and Ureaplasma and Chlamydia trachomitus: causes of urethritis in men. c. M. genitalium, Chlamydia and Gonorrheae: cause pelvic inflammatory disease and cervicitis d. M. hominis: causes pyelonephritis, occasional cause of pelvic inflammatory disease, postpartum fever and endometritis in women who’ve delivered e. Ureaplasma: Important in immunocompromised people and infants. The main thing to know is: Most common cause of chorioamnionitis (inflammation of the fetal membrane). Implicated in pre-term birth. It’s present in many women, and if it’s in the lower genital tract, it can invade the amniotic cavity and cause inflammation and lead to premature birth and delivery. It also may attach to sperm and cause impaired fertility. Like M. hominis it can cause postpartum fever and pneumonia and meningitis (as can Mycoplasma) in newborns. It’s an important cause of arthritis in people with antibody deficiency (septic arthritis). Biggest thing recently: its role in development of chronic lung disease (bronchopulminary dysplasia) f. If the mom has an intrauterine infection with Ureaplasma, it can gain access to the respiratory tract of the developing fetus. If born prematurely, the Ureaplasma causes inflammation in the lung, causing a greater oxygen demand. You give oxygen longer but you have inflammation in the lung, so it leads to lung damage to the baby (oxygen toxicity). No doubt it’s connected to chronic lung disease in newborns. Certainly there’s a connection between those who’ve had an intrauterine infection and the babies that are colonized with it at the time of birth. They are at great risk for developing bronchopulminary dysplasia. g. Ureaplasma and M. hominis-grown easily, faster growing, PCR can also be used to grow them i. Antibody isn’t a good test for these organisms because so many people have these in there body and thus have antibody. So, antibody doesn’t really have a role. h. M. genitalium-the smallest free-living organism, smallest genome, very slow-growing and very fastidious, PCR assay is the way to find it. [end 48:41 min]