Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Germ theory of disease wikipedia , lookup
DNA vaccination wikipedia , lookup
Common cold wikipedia , lookup
Rheumatic fever wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Molecular mimicry wikipedia , lookup
Globalization and disease wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Innate immune system wikipedia , lookup
Schistosomiasis wikipedia , lookup
West Nile fever wikipedia , lookup
Hepatitis C wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Henipavirus wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Marburg virus disease wikipedia , lookup
Infection control wikipedia , lookup
Neonatal infection wikipedia , lookup
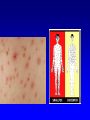
Human Herpesvirus Infections Dr. Ghazi F. AI- Haji Cardiologist 2010 lessons Epidemiology:. Pathogenesis Clinical manifestations Diagnosis Patient management Prevention Characteristics of herpes viruses • • • • Persistence Latency Reactivation Tissue tropism Human Herpes Viruses • Alphaherpesviruses • HSV-1 and HSV-2 • Varicella-zoster virus (VZV) • Betaherpesviruses • Cytomegalovirus (CMV) • HHV-6 and HHV-7 • Gammaherpesviruses • Epstein-Barr Virus (EBV) • Kaposi’s sarcoma-associated herpesvirus (KSHV,HHV-8) Cell types infected by different herpesviruses • VZV and HSV • Epithelial cells and neurons • CMV • Ductal epithelium, leukocytes • EBV •Oropharyngeal epithelium, B lymphocytes • KSHV •Endothelium, B cells Herpes simplex virus Ubiquitous virus that infects greater than 75% of the adult population (HSV-1) and to varying degrees in the case of HSV-2, depending on the population studied. There are many manifestations of HSV infection in addition to the common cold sore or fever blister. Manifestations depend on anatomic site involved, age, immune status of the host Herpes labialis Genital herpes Herpes gladiatorum Herpetic whitlow Eczema herpeticum Congenital HSV infection Herpetic gingivostomatitis Disseminated infections Pneumonia Esophagitis Hepatitis Encephalitis Chronic and resistant infections Infection Type Lesions/ Symptoms Type-specific antibody at time of presentation HSV-1 HSV-2 First episode, Primary (Type 1 or 2) +/Severe, bilateral - - First episode, Non-primary Type 2 +/Moderate + - First episode, Recurrence Type 2 +/Mild +/- + Symptomatic, Recurrence Type 2 +/Mild, unilateral +/- + Asymptomatic, Infection Type 2 - +/- + Oral-Facial Herpes Gingivostomatitis and pharyngitis most common manifestation of primary HSV−1 infection. in children and young adults and may be subclinical, symptoms and signs include fever, malaise, myalgias, inability to eat, irritability, and cervical adenopathy, may last 3– 14 days. Recurrent herpes labialisreactivation from trigeminal ganglia-lesions Rx: Acyclovir, Famciclovir, Valacyclovir. Antivirals-HSV Require TK phosphorylation for activity ACV binds to replicating viral DNA causing premature chain termination ACV and Famciclovir both inhibit viral DNA polymerase Resistance mediated by reduction in viral TK Valacyclovir rapidly converted to ACV and higher levels achieved Excellent activity against HSV Moderate activity against VZV Genital Herpes Primary episode: Fever, headache, myalgias, dysuria, vag/urethral discharge lymphadenopathy Lesions: vesicles, pustules, erythematous ulcers Can be caused by HSV-1 & 2 Recurrence rate higher with HSV-2 infection HSV proctitis (ulcerative lesions on sigmoidoscopy) and perianal lesions: HIV, rectal intercourse Trigeminal ganglia & sacral ganglia- most common sites of HSV-1 and HSV-2 latency Rx: Acyclovir, Famciclovir, Valacyclovir Neonatal Herpes Neonates may develop primary HSV infection following vaginal delivery in the presence of active genital HSV infection in the mother. Caesarean section should therefore be considered. < 6weeks of age Without therapy mortality is approx 65% Skin lesions most commonly recognized feature - may not appear or may be delayed Acquired perinatally from contact with genital secretions or close contact with family member 30% due to HSV-1 and 70% HSV-2 ---Rx- IV Acyclovir Infection of the finger Occurs as complication of primary oral or genital herpes, direct innoculation, occupational exposure Vesicular or pustular lesion Abrupt onset erythema, localized tenderness Fever, lymphadenitis, lymphadenopathy are common Prompt diagnosis Herpes Gladiatorum Any skin area may be infected Transmission facilitated by trauma Prompt diagnosis to contain the spread Eczema Herpeticum Potentially life-threatening viral infection that arises in pre-existing skin conditions like atopic dermatitis In some cases may lead to fulminant life threatening disseminated infection Acyclovir, Valacyclovir. Antibiotics may be needed as well Rare entity Skin lesions, chorioretinitis, microcephaly H in TORCH infections Herpes Encephalitis Accounts for 10-20% of viral encephalitis 2.3 cases per 1 million HSV-1 >95% cases Biphasic- 5-30, >50yrs Primary infection or reactivation Fever, altered mental status, bizarre behavior, seizures Temporal lobe involved Diagnosis: LP: Increased CSF protein, leucocytes with lymphocytic predominance and increased CSF RBCs due to hemorrhagic necrosis CSF HSV PCR: High sensitivity and specificity Treatment: IV Acyclovir, reduces mortality. Despite treatment mortality upto 15% with survivors with longterm cognitive impairments Eryrthema Multiforme EM is a acute self limiting, sometimes recurring skin condition considered to be a Type IV hypersensitivity reaction associated with certain infections, medications. Cell mediated immune reaction associated with HSV antigens Antigens may be detected in keratinocytes by IF or HSV DNA detected by PCR Typical “Target Lesions” Suppression of HSV may prevent EM. Once EM erupts antivirals not effective “B” virus, Herpesvirus simiae • • • • Endemic HSV homolog of nonhuman primates Risk for those handling animals Causes a fulminant neurologic syndrome in humans May be treatable with acyclovir Varicella-Zoster Virus Infections Varicella (Chickenpox) Bacterial superinfection CNS: aseptic meningitis, transverse myelitis, GBS, encephalitis, Reye’s syndrome Varicella pneumonia Myocarditis, nephritis, hepatitis Perinatal varicella: high mortality Herpes Zoster (Shingles) T3-L3 dermatomes most frequently involved Zoster opthalmicus: Opthalmic branch of Trigeminal Nerve involved Ramsay Hunt syndrome: vesicles , loss of sense of taste in ant 2/3rds of tongue, ipsilateral facial palsy: geniculate ganglia of sensory branch of Facial Nerve involved. Chickenpox Childhood disease Highly contagious: pt infectious 48hrs prior to rash. IP: 10-21 days Fever, malaise, skin lesions: maculopapules, vesicles, pustules, scabs in various stages of evolution Early lesions “dew drop on rose petal” Diagnosis: clinical, VZV DNA PCR, Tzanck smear demonstrating multinucleate giant cells, Direct immunofluorescence Acyclovir therapy efficacious if used <24hrs Immunocompromised: IV Acyclovir Chickenpox pulmonary x-ray Herpes zoster(shingles) Shingles never occurs as a primary infection but results from reactivation of latent VZV from dorsal root and/or cranial nerve ganglia. It produces skin lesions similar to chickenpox, although classically they are unilateral and restricted to a sensory nerve (dermatomal) distribution. Shingles occurs at all ages but is most common in the elderly, immune deficiency state or after intra-uterine infection. The onset of the rash of shingles is usually preceded by severe dermatomal pain (Burning pain), due to involvement of sensory nerves. complication The most common and troublesome complication is post-herpetic neuralgia: (persistence of pain for 1-6 months or more following healing of the rash). Shingles involving the ophthalmic division of the trigeminal nerve can result in blindness in the absence of antiviral therapy. Herpes Zoster Opthalmic division of Trigeminal Nerve Adapted from: gb.udn.com HZ: Involvement of tip of nose is classic indicator of ocular involvement (Hutchinson’s sign) Herpes Zoster treatment Treatment with acyclovir, Famciclovir or valacyclovir is beneficial with accelerated healing of lesions and resolution of neuralgia Immunocompromised should receive initial reaction with IV Acyclovir CMV disease β Herpes virus dsDNA Spread by repeated prolonged exposure CMV present in breast milk, saliva, feces, urine, semen, cervical secretions Daycare centers Once infected person carries CMV for life. Reactivation syndromes: T cell mediated immunity compromised Pneumonitis Bone marrow transplant Colitis AIDS, solid organ transplantation Retinitis AIDS Hepatitis SOT Nephritis Kidney transplantation Mononucleosis: F/C, malaise, fatigue, splenomegaly, atypical lymphocytosis, leucopenia, LFT abnormalty Congenital infection: microcephaly, chorioretinitis When GCV(ganciclovir) enters cells, it must undergo a series of phosphorylations until it is active to be able to inhibit viral DNA polymerase. The initial phosphorylation step is done by a viral protein kinase that's encoded by UL97. Mutations in UL97 or in the viral DNA polymerase are the 2 major mechanisms that underlie ganciclovir resistance and antiviral resistance in general Activity: CMV, HSV, varicella Adapted from: medscape.com Cidofovir Analog of deoxycytidine monophosphate causes premature chain termination of viral DNA and inhibits DNA polymerase Does not require TK ACV resistant strains usually not resistant to cidofovir HSV, CMV, HHV6 & 8, VZV Nephrotoxic and BM toxicity Foscarnet Blocks binding of deoxynucleotidyl triphosphate to viral DNA polymerase CMV, HSV, VZV CMV retinitis and ACV resistant HSV, GCV resistant CMV Nephrotoxicity and electrolyte abnormalities CMV Retinitis Normal Fundoscopic exam www.kellogg.umich.edu/.../cmv-retinitis.html Hemorrhages, vessel sheathing, retinal edema AIDS with CD4<50 IV Ganciclovir then oral Valganciclovir until CD4>100-150 CMV Pneumonitis Highest risk in Lung transplant and BMT patients High mortality Diagnosis with BAL(bronchoalveolar lavage) with cells showing viral and inclusions body, PCR. Lung biopsy-gold std Treatment with IV Ganciclovir CMV inclusions in lung http://library.med.utah.edu/WebPath/TUT ORIAL/AIDS/AIDS021.html CMV colitis The transplanted organ is particularly vulnerable as a target for CMV infection Patients may present with diarrhea, heartburn, odynophagia Diagnosis made with biopsies obtained on endoscopy CMV immunostain positive IV Ganciclovir Thank you for attention True( T) or false (F) Properties of transforming herpesviruses • Drive infected cell proliferation • Prevent apoptosis of infected cells • Avoid immune attack • Infect new cells Epstein Barr virus (EBV)-associated diseases •Infectious Mononucleosis •Burkitt lymphoma •Nasopharyngeal carcinoma •Lymphoproliferative Disease •Hodgkin’s Disease, EBV-assoc. NHL •Gastric carcinoma Infectious mononucleosis: Kissing disease Oral Hairy Leukoplakia White plaques on lateral surface of tongue Seen in HIV/AIDS, immunocompromised individuals Burkitt’s Lymphoma Rapidly growing NHL 15% of cases in US and 90% cases in Africa associated with EBV Extremely responsive to chemotherapy and recurrence is rare from thacher’s.org NPC and EBV Figure 135-4 Nasopharyngeal carcinoma. A, Nests of metastatic undifferentiated nasopharyngeal carcinoma in a fibrous stroma in a lymph node (hematoxylin and eosin). Metastases often lack infiltrating lymphocytes. B, In situ hybridization for Epstein-Barr virus (EBV)-encoded RNA (EBER) (brown) demonstrates EBV infection in most cells in the same area of the tissue. (Magnification ×100.) (Courtesy of Dr. Miguel Rivera.) Downloaded from: Principles and Practice of Infectious Diseases (on 28 February 2006 03:59 PM) © 2005 Elsevier Hodgkin’s lymphoma and EBV Figure 135-3 Mixed cellularity classic Hodgkin's lymphoma. A, Lymph node architecture is effaced by an infiltrate comprised of small lymphocytes, epithelioid histiocytes, plasma cells, eosinophils, and Hodgkin and Reed-Sternberg cells (arrow) (hematoxylin and eosin). B, In situ hybridization for Epstein-Barr virus (EBV)-encoded RNA (EBER) (brown) demonstrates EBV infection in the malignant Hodgkin and Reed-Sternberg cells. (Original magnification x400.) (Courtesy of Dr. Jeffery Kutok.) Downloaded from: Principles and Practice of Infectious Diseases (on 28 February 2006 04:00 PM) © 2005 Elsevier PTLD and EBV Figure 135-2 Post-transplantation lymphoproliferative disease involving the colon. A, The tumor is composed of large, atypical lymphoid cells (hematoxylin and eosin). Scattered macrophages (arrow) are seen, producing a "starry-sky" appearance. B, In situ hybridization for Epstein-Barr virus (EBV)-encoded RNA (EBER) (brown) shows variably intense nuclear staining in the majority of tumor cells, indicating EBV infection. (Original magnification x400.) (Courtesy of Dr. Jeffery Kutok.) Downloaded from: Principles and Practice of Infectious Diseases (on 28 February 2006 04:00 PM) © 2005 Elsevier Kaposi’s sarcoma-associated virus (KSHV, HHV8) •Kaposi’s sarcoma (KS) •Multicentric Castleman’s disease •Primary Effusion Lymphoma (PEL) Kaposi’s sarcoma Classic Kaposi's sarcoma (CKS) is a neoplasm characterized by abnormal angiogenesis that requires infection with a human herpes virus, HHV-8, along with other cofactors. purplish, reddish blue, or dark brown/black macules, plaques, and nodules on the skin. mucous membranes of mouth and gastrointestinal (GI) tract and regional lymph nodes may be affected later in the course. Biopsy for definitive diagnosis radiation therapy, excision, cryotherapy, laser ablation, chemotherapy emedicine.medscape.com/article/279734-overview Kaposi’s sarcoma: Seen in AIDS patients Figure 137-2 Kaposi's Sarcoma Involving a Lymph Node. Left panel, Spindle cell proliferation (white arrows) containing poorly formed vascular spaces with entrapped red blood cells (black arrows). Areas of uninvolved lymph node (LN) are seen at the top (H&E). Right panel, Immunohistochemical detection of Kaposi's sarcoma-associated human herpesvirus (KSHV) latency-associated nuclear antigen 1 (LANA1) (brown) in the nuclei of many spindle cells indicates KSHV infection (×200). (Courtesy of Dan Jones, MD, PhD.) Downloaded from: Principles and Practice of Infectious Diseases (on 28 February 2006 03:59 PM) © 2005 Elsevier Fever, LAN, hepatosplenomegaly, night sweats Most patients with MCD die due to fulminant infection, progressive disease or related malignancy Human Herpes Viruses • Alphaherpesviruses • HSV-1 and HSV-2 • Varicella-zoster virus (VZV) • Betaherpesviruses • Cytomegalovirus (CMV) • HHV-6 and HHV-7 • Gammaherpesviruses • Epstein-Barr Virus (EBV) • Kaposi’s sarcoma-associated herpesvirus (KSHV,HHV-8) Cell types infected by different herpesviruses • VZV and HSV • Epithelial cells and neurons • CMV • Ductal epithelium, leukocytes • EBV •Oropharyngeal epithelium, B lymphocytes • KSHV •Endothelium, B cells Take Home points Latency and potential for reactivation Immunocompromised with defective cell mediated immunity at risk of severe disease HSV- Acyclovir HSV encephalitis: IV ACV improves mortality Chickenpox: lesions in various stages of development Zoster Opthalmicus: opthalmic division of Trigeminal Nerve VZV diagnosis: Tzanck smear- mulinucleate giant cells, PCR CMV : Mononucleosis without exudative pharyngitis CMV retinitis, colitis, pneumonia CMV dx: PCR, cells with classic inclusions on biopsy EBV: IM, Heterophile antibody positive Transforming virus: EBV, KSHV, HHV-8