Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
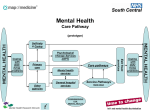
Current and Future Developments in the National Ambulance Service Dr Cathal O’Donnell Medical Director NAS Rural Island & Dispensing Doctors of Ireland Annual Conference 2013 325,000 calls per year 228,000 999 calls per year = 625 every day 20 million kilometres annually Recent clinical developments • • • • STEMI Stroke Trauma Helicopter service Future Developments • Treat and discharge • New therapies Donegal Clinical Society Sept 2013 Donegal Clinical Society Sept 2013 Resus Conference 2013 Future Developments Treat and discharge NIV Tranexamic acid Treat and Discharge Q. Do all 999 callers need transport to hospital? Q. If not, how can we safely identify those that do not? Q. How will stakeholders feel about this? Patients GPs and GP co-ops Emergency Departments 5/6.9.1 Version 2, 01/13 From relevant CPGs Clinical Care Pathway Decision – Treat & Referral P AP Non serious or non life threat Administer specific treatment & provide patient with the opportunity to recover/ respond Patient responds to intervention(s) No Yes Conduct complete patient assessment Focused history Systematic physical examination All generic inclusion criteria present No Yes Practitioner satisfied with non ED care Generic patient inclusion 1. ≥ 18 years & ≤ 60 years. 2. Not pregnant. 3. Social support available. 4. Demonstrates capacity and willing to engage. 5. Reliable history. 6. Vital signs within normal range (following care). 7. Compliant with treatment, including own medications. 8. Clinical status of ‘Non serious or non life threat (following care). 9. Absence of self-inflicted injury or assault. 10. No observed significant relevant co-morbidity. 11. 1st call for same condition within 30 days. 12. Registered with general practitioner. If in any doubt about generic inclusions the practitioner should transport to ED No Yes CPG for treat & referral available for condition If medical practitioner is present; follow direction on transport decision No Transport to ED Yes An adult carer, both capable & willing to accept responsibility, available No Yes Explain clinical pathway options to patient and carer Vital sign Normal range Respiratory Rate Patient & carer accepts non ED care Yes Go to appropriate T&R CPG No 12 – 20 ≥ 96% SpO2 Inspired O2 Room air Systolic BP 111 - 150 Pulse (BPM) 51 - 90 AVPU/CNS Response Temperature (oC) Alert 36 – 37.5 Clinical Care Pathway options CP1 Treat & Transport to an Emergency Department CP2 Treat & Referral for follow up care within 2 hours (arranged with local practitioner) CP3 Treat & Referral for follow up care within 48 hours or as soon as practicable CP4 Treat & Referral to self care with after care instructions Reference: Ambulance Service of NSW, 2008, CARE Clinical Pathways HSE Acute Medicine Programme, 2011, Guiding Framework and Policy for the National Early Warning Score System to Recognise and Respond to Clinical Deterioration 5/6.9.2 Hypoglycaemia – Treat & Referral Version 2, 01/13 From Clinical Pathway Decision CPG Previously diagnosed with diabetes Yes Exclusions present No P AP Specific Hypoglycaemic exclusion 1. First ever hypoglycaemic episode. 2. < 30 days since last episode. 3. Unable or unwilling to eat. 4. Latest blood glucose < 4.0 mmol/L (after treatment). 5. No serial improvement of blood glucose. 6. On oral hypoglycaemics (sulphonylurea tablets in particular). 7. Recent medication change or additional medications prescribed (within 30 days). 8. Seizure in association with hypoglycaemia 9. Insulin or oral hypoglyacemics overdose If in any doubt about 1 to 9 above the practitioner should transport to ED CP 1 CP 2 CP 3 CP 4 Transport Immediate 48 hours Self care 1. Complete after care Instructions and give a copy to the patient or carer 2. Complete the PCR and mark for Clinical Audit Ensure patient takes in both quick (lucozade, fruit juice or sweets) and longer acting (bread, toast, biscuit) carbohydrates Flush line with 10 mL NaCl following removal of 10% Dextrose infusion If the patient expresses a wish to attend an Emergency Department then arrangements shall be made to transport him/her there