Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
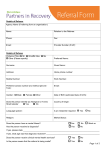
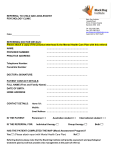
Careplus Physiotherapy Referral Form Patient Details: Male Name: Female D.O.B: NHS No. Patients Address including postcode: Home Tel No.: Work No: Translator required : Yes No Mobile No: Email: Language/dialect: Transport required Yes GP Name & Address: (see PCT policy) Practice Stamp: Urgency of referral Urgent (2 weeks) Type of referral No Physio Routine (4 weeks) Specialist Pathway Team Not able to advise (access to diagnostics, onward referral and injections) Reason for referral: (Clinical history, duration and severity of symptoms:- comments) First episode Flare up First line management by GP Previous Treatment Exclusion Red flags ;- Suspected malignancy, infection, fracture or dislocation, significant worsening neurology or cauda equina symptoms. (If suspected, patient needs secondary care referral or GP investigation. Do not use this form for patients requiring admission emergency treatment or cancer fast track.) Please complete additional information below to assist the triage process. Knee referrals: Shoulder referrals: Previous investigations (please attach results and relevant letters) History of significant trauma History of significant trauma Immediate swelling History of intermittent locking X-rays History of locking/giving way on twisting the knee Suspected distal biceps rupture Blood Test Recurrent dislocation/subluxation Yellow Flags e.g. catastrophising behaviour, fear of movement, work related issues, emotional issues PMH Signature of refer: Other: (e.g. MRI/US) Previous Pain Clinic attendance Drug History inc. current pain management (please attach printout if necessary) Print Name: BMI Date: Please refer via Choose and Book or fax form to 01709 424062 BP