Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
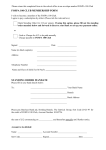
Campus Recreation Services SPORT CLUB MEDICAL HISTORY FORM NAME: _________________________________________________ DATE: __________________ (Last) (First) (MI) CSU ID: ______________________ CLUB: ___________________________ ADDRESS: ________________________________________________ DATE OF BIRTH: ________________________ PHONE: _________________________ AGE: _____________ EMERGENCY CONTACT: ________________________________ GENDER: ____________ RELATIONSHIP: ______________________ PHONE: __________________________ Have you ever been restricted from athletic/recreational participation due to health problems? If yes, please list reason and date: _______________________________________________ Yes No Do you have any known allergies? If so, list: __________________________________________________________________ Yes No Are you currently taking any medications? If so, list: __________________________________________________________________ Yes No Do you currently have a muscle, joint or back disorder that could be aggravated by physical activity? Yes No Do you have an ongoing medical condition such as diabetes or asthma? If so, list: __________________________________________________________________ Yes No Do you currently wear glasses or corrective lenses? Yes No Have you ever had a head injury or concussion? If so, when was your last one? __________________________________________________ If so, how many have you had? __________________________________________________ If so, do you have any current problems? __________________________________________ Yes No Have you ever had a stress fracture? Yes No Do you regularly use a brace or an assistive device? If so, list: ____________________________________________________________________ Yes No List any recent operations, serious illness or hospitalizations and the dates of each: _______________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ I certify that the medical history above is accurate and complete to the best of my knowledge. SIGNATURE: ____________________________ DATE: __________________