Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Discovery and development of beta-blockers wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Plateau principle wikipedia , lookup
Discovery and development of TRPV1 antagonists wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
CCR5 receptor antagonist wikipedia , lookup
Neuropharmacology wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
Psychopharmacology wikipedia , lookup
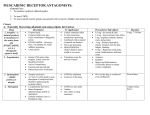
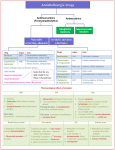
HuBio 543 September 24, 2007 Neil M. Nathanson K-536A, HSB 3-9457 [email protected] Muscarinic Antagonists Tertiary Muscarinic Antagonists H2 C CH CH2 O CH2OH NCH3 CHO C H2 C CH CH2 Atropine C H C H CH NCH3 O C CH H CH2 O CH2OH CHO C C H CH2 Scopolamine Tertiary Antagonists Atropine * Scopolamine * Homatropine Tropicamine Tolterodine Oxybutynin Quaternary Antagonists N- methyl atropine * N- methyl scopolamine Ipratropium * Propantheline Tiotropium* QuickTime™ and a TIFF (LZW) decompressor are needed to see this picture. QuickTime™ and a TIFF (LZW) decompressor are needed to see this picture. Biphasic Effect of Atropine on Human Heart Rate 80 Heart 70 Rate 60 50 0 2 6 4 Dose of Atropine (µg/kg) 8 10 Why the biphasic dose-response curve to atropine? 1. CNS- Low doses of atropine may act preferentially in the CNS to increase parasympathetic outflow 2. Presynaptic effect- Low doses of atropine may act preferentially on presynaptic mAChR on parasympathetic terminals, resulting in increased ACh release onto the heart Presynaptic Muscarinic Receptors Inhibit ACh Release From Parasympathetic Terminals ACh ACh ACh ACh mAChR XX ACh mAChR ACh Presynaptic Muscarinic Receptors Inhibit ACh Release From Parasympathetic Terminals ACh ACh ACh mAChR XX mAChR ACh Therefore: Less ACh is released, Heart Rate is not slowed as much Increased ACh Release and Bradycardia When Presynaptic mAChR Are Blocked by (Low Doses of) Atropine ACh ACh ACh ACh mAChR ACh Atropine mAChR ACh Biphasic Effect of Atropine on Human Heart Rate 80 Heart 70 Rate 60 50 0 2 6 4 Dose of Atropine (µg/kg) 8 10 Biphasic Effect of Atropine on Human Heart Rate QuickTime™ and a TIFF (LZW) decompressor are needed to see this picture. Low doses preferentially: 1. Act in CNS to increase parasympathetic outflow- decreases HR 2. Blocks presynaptic receptor on parasympathetic nerve terminal-increases ACh release, decreases HR Parasymp. Ganglion MR MR High doses: Block mAChR on heartBlock effects of ACh, increases HR Sensitivity of Target Organs to Atropine Increase or Decrease (%) 80 60 Salivary Secretion (-) Micturition Speed (-) 40 20 Heart Rate (+) Accomodation (-) 0 0.5 1 Atropine (mg/70 kg) 2 Toxic Effects of 3o mAChR Antagonists • • • • • • Visual problems Constipation and urinary retention Glaucoma in predisposed individuals Hallucinations and delirium Decreased sweating and salivation Erectile problems/impaired vaginal lubrication Can use AChE inhibitors as an antidote (of smooth muscle) Tricyclic anti-depressants can act as mAChR antagonists Physostigmine reverses anti- muscarinic CNS effects of tricyclic anti-depressants Quaternary Muscarinic Antagonists H2 C H2C CH + H3CNCH3 CH2 O CH2OH CHO C C H CH2 CH N-methylatropine H2 C CH + (H3C) 2HCNCH3 H2 C CH CH2 O CHO C CH2 CH2OH C H Ipratropium Tertiary Antagonists Atropine * Scopolamine * Homatropine Tropicamine Tolterodine Oxybutynin Quaternary Antagonists N- methyl atropine * N- methyl scopolamine Ipratropium * Propantheline Tiotropium* N-methylatropine does not cross membranes as well as atropine N-methylatropine does not cross membranes as well as atropine 100 80 Cumulative Adsorption 60 (%) Atropine 40 20 N-methylatropine 0 50 100 150 200 Distance From the Nose (cm.) Therapeutic uses of mAChR Antagonists • • • • • • • (Preanesthetic medication) Ophthalmological- mydriasis and cylcoplegia GI and Urinary Tract- decrease tone & motility Decrease excessive sweating CV- block vagally-mediated bradycardia CNS- motion sickness Respiratory tract- bronchodilation Therapeutic uses of mAChR Antagonists • • • • • • • (Preanesthetic medication) Ophthalmological- mydriasis and cylcoplegia GI and Urinary Tract- decrease tone & motility Decrease excessive sweating CV- block vagally-mediated bradycardia CNS- motion sickness Respiratory tract- bronchodilation Cholinergic Innervation of the Airways Lumen Lumen Gland Cholinergic Innervation SMOOTH MUSCLE Rates of Hospitalization in Control and Ipratropium Groups 60 50 Patients Hospitalized (%) Control Ipratropium 40 30 20 10 0 All Patients Moderate Asthma Severe Asthma Patient compliance is a big problem Patients prescribed ipratropium inhalers: -Self- reported compliance was 60- 70% -This was confirmed by canister weight BUT: Compliance was also determined by electronic monitoring and found to be much poorer Medilog: electronic inhaler monitor Monitoring showed that only 15% of subjects actually used the inhaler as prescribed. Patients want to be liked by their physicians 14% of patients actuated inhaler more than 100 times on the day of a visit. Synaptic Transmission Through a Sympathetic Ganglion: From CNS N Main Pathway To Target ACh M Modulatory Pathway Effect of Ganglionic Stimulants BP HR + DMPP + Hexamethonium: + McN-A-343 BP HR + DMPP + McN-A-343 Muscarinic Receptors in Sympathetic Ganglia • Excitatory (normally modulate transmission through the nicotinic pathway) • Selectively activated by McN-A-343 • (McN-A-343 therefore causes increased BP) • Selectively blocked by pirenzepine Pirenzepine Selectively Blocks mAChR in Sympathetic Ganglia Atropine (atria or ganglia) Pirenzepine (ganglion) Pirenzepine (atria) DRUG CONCENTRATION Subtypes of mAChR • Five different mAChR in humans (all in CNS) • M1- in sympathetic ganglia (and adrenal medulla), activated by McN-A-343, blocked by pirenzepine • M2- cardiac mAChR; can contribute to contraction of some smooth muscles; a presynaptic receptor on some nerve terminals • M3- mediates contraction of smooth muscle, relaxation of vasculature, and secretion from many glands Cevimeline • Selective M3 agonist • Used for treatment of xerostomia and Sjorgren’s syndrome • Long-lasting sialogogic agent • May have fewer side effects than pilocarpine Tiotropium • Selective M3 antagonist – Very slow dissociation from M3 mAChR – 4° antagonist – like ipratropium, is an inhaled bronchodilator • Used for treatment of COPD Effect of Ganglionic Stimulants BP HR + DMPP + McN-A-343 + Hexamethonium: BP HR + DMPP + McN-A-343