Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
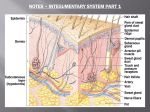
BLACK SPOT GROUP B2 SCENARIO A 35 years old woman came to the hospital with complaint of black spots on both of her cheeks. She has been having the problems since 4 months ago. No family history of similar diseases has ever recorded previously. Lab assessments reveal normal findings. KEYWORDS • • • • • 35 years old woman black spots on both of her cheeks since 4 months ago No family history Lab assessments reveal normal findings QUESTIONS 1. What is the anatomy of the skin? 2. What is the physiology of the skin? 3. What is the pathomechanism of black spots on the skin? 4. What is the differential diagnosis related to the case? ANSWERS What is the anatomy of the skin? • Epidermis – Stratum corneum – Stratum Lucidum – Stratum granulosum – Stratum spinosum – Stratum basale • • Dermis – Pars papilare – Pars retikulare Hypodermis (subcutis) – elastin and loose connective tissue – panikulus adipose – nerve endings, blood vessel, and lymph – fibroblasts, macrophages and adipocytes • • Skin gland – Gland. Sudorifera • Ekrin gland all over the skin (palm, soles, aksila) • Apokrin gland aksila, pubis, labia mayora, ear canal – Gland. Sebacea • Except palm and soles. Besides the hair follicle Hair – Lanugo baby – Terminal hair adult • Ungues – Thickening of terminal part stratum corneum. • Eponikium : skin that cover the nail at the proximal • Hiponikium : skin that covered by the nail What is the physiology of the skin? FUNCTIONS DESCRIPTION ABSORPTION • • • • • • • • Protects against physical or mechanical damage Impermeability of Stratum Corneum Sweat and sebum excretion ph 5-6.5 Heat sensation: Ruffini body Cold sensation: Krause body Touch: tactile Meissner, Merkel Ranvier Pressure: Paccini body O2, CO2 & water (steam) transepithelial junction EXCRETION • Glands metabolic wastes; NaCl, Urea, Uric Acid, Ammonia THERMOREGULATION PIGMENTATION • • • Sweat production Muscle contraction Melanocyte produce colour to the skin KERATINIZATION • Basal cells – Spinosum – Granulosum – corneum VITAMIN D PRODUCTION • 7 dehydroxyl cholesterol – sun light vitamin D production PROTECTION PERCEPTION What is the pathomechanism of black spots on the skin? Melanocyte Chromatophores/ melanophores Melanin Brown to black pigment Exposure to sun rays photooxidized Producing more melanin accumulated epidermis As protection for the underlying skin from sun’s radiation What is the differential diagnosis related to the case? 35 YEARS OLD WOMAN Yes BLACK SPOTS ON BOTH CHEEKS Yes NO FAMILY HISTORY Yes MELASMA Yes LENTIGO Yes Yes Yes Yes POST-INFLAMMATORY HYPERPIGMENTATION Yes Yes Yes Yes MELANOMA Yes Females : males Depends on subtypes and assymetrical No (usually with family history) EPIDEMIOLOGY MELASMA - Race: darker skin types > than in lighter skin types - Sex: women (90%) > men - Age: most commonly occurs in women in reproductive years. LENTIGO - Race: fair-skinned whites > darkskinned individuals - Sex: Women > men - Age: children – since birth Adults – acquired ETIOLOGY PATHOMECHANISM - UV light - Hormone - Drug - Genetic - Race - cosmetic Spectrum UV destroys sulfidril in the epidermis causes uncontrooled tyrosinase enzyme which later lead to melanogenesis - UV light Spectrum UV increase number of melanocyte at the dermo-epidermal junction without localized proliferation CLINICAL MANIFESTATION SUPPORTING EXAMINATION HISTOPATHOLOGICAL FINDINGS MELASMA Predilection: cheeks and nose (malar), chin (mandibular), forehead, supercilia and upper lip (centrofacial) Colour: Light brown or dark brown Border: Regular with irregular edge - Anamnesis - Physical examination - Wood lamp Epidermal pigment is enhanced during examination with a Wood light, whereas, dermal pigment is not. Epidermal melanin is found in keratinocytes in the basal and suprabasal area. In most cases, the number of melanocytes is not increased, yet the melanocytes that are present are larger, more dendritic, and more active. LENTIGO Predilection: Mucosal surface of the skin; buccal mucosa, gums, palatum durum, lips, nose, mouth, extremeties Colour: Brown to black Shape: Oval shape, irregular Size: 1-5 mm - Anamnesis - Physical examination -Wood lamp Increase number of hyperpigmentated macula consists of large amount of melanocyte at the stratum basale and macrophages with pigments at the upper dermis. Epidermis is covered by melanin granule. MELASMA TREATMENT AND PREVENTION Treatment Depigmenting agents – inhibit key enzymes involved in melanin synthesis. Hydroquinone USP 4% (Claripel cream with sunscreens) Retinoids regulate cell growth and proliferation. Tretinoin (Avita, Retin-A) Antibiotic agents inhibit DNA synthesis and mitochondrial enzymes to interrupt hyperactive melanocytes. Azelaic acid (Azelex) COMPLICATION Resistant cases or recurrences occur often and are certain if strict avoidance of sunlight is not rigidly heeded. It may return with additional pregnancies or use of these medications. PROGNOSIS Melasma often fades over several months after stopping birth control pills or HRT, or after delivering a child. In patients in whom lentigines are associated with systemic abnormalities or complications, the prognosis may depend on the severity of the associated conditions Good Prevention strict avoidance of sunlight Stop usage of :contraception oral, color cosmetic and drug can generate melasma LENTIGO Treatment Chemical peels – Removes several layers of sun damaged skin cells, leaving fresh skin which has a more even surface and colour Cryosurgery Laser; YAG laser Prevention The application of sunscreen Limiting exposure to sun tanning and the use of artificial sources of UV light THANK YOU QUESTIONS?