Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
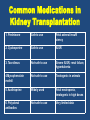
Pregnancy & Kidney Prof. (Dr.) Iffat Yazdani Aga Khan University Hospital / Clifton Kidney & General Hospital Normal Renal Alterations in Pregnancy Changes in G.F.R. • GFR and RBF rise markedly • Glomerular hyperfiltration results in normal reduction in the plasma creatinine concentration to about 0.4 to 0.5 mg/dL • Blood urea nitrogen (BUN) and uric acid levels fall for the same reason Before Pregnancy Women with chronic kidney disease often have amenorrhoea but may still occasionally ovulate and thus conceive • Contraceptive measures that consider clinical comorbidities should be taken by those who do not wish to become pregnant. • Folic acid 400 μg, until 12 weeks’ gestation. • Low dose aspirin (50-150 mg/day) reduces the risk of pre-eclampsia • Fetotoxic drugs - such as ACE inhibitors and angiotensin II receptor blockers—should be stopped. 2 questions, when a woman with underlying kidney disease becomes pregnant: • What is the effect of pregnancy on the kidney disease ? • What is the effect of the kidney disease on pregnancy ? 1. Pregnancy in mild to moderate Kidney Disease 2. Pregnancy in Dialysis Patients 3. Pregnancy in Renal Transplant 4. Pregnancy in Diabetic Nephropathy 5. Pregnancy in Lupus Nephropathy 6. Pregnancy in Glomerulonephritis Renal Function may decline as a result of Pregnancy among patients with renal disease, determined in part by the severity of underlying renal disease. Effect of Pregnancy on Renal Function GRF Mildly reduced Plasma Creatinine < 1.5 mg % Permanent decline in Renal Function 0-10% Others Transient Decline GFR moderately reduced Plasma Creatinine 1.6-2.9 mg % SCreatinine rises as pregnancy progresses 40% of women decline in renal function Risk of Irreversible loss of GRF exceed s in patients who have uncontrolled hypertension During Pregnancy Care of Women with Chronic Kidney Disease Urine 4 – 6 Weeks Check (1) Prophylactic antibiotics, (2) proteinuria – thromboprophylaxis with low molecular weight heparin if > 1g proteinuria /24 h (3) haematuria – perform microscopy Blood Pressure Aim to keep it between 120/70 & 140/90 mm Hg Renal Function Full Blood Count Check serum Keep creatinine & Urea Haemoglobin depending on the at 10-11 g/l stage of the disease. More frequently for disease stages 3-5 and in the second half of pregnancy. Ultrasound of Renal Tract Perform Base line renal ultrasound – 12 weeks CKD in mild to moderate kidney disease Nevis IF American Society of Nephrology - 2011 – Mother • Gestational HTN • Pre Eclampisa / Eclampsia (2nd trimester) – Child • Preterm Birth • Small for age • Still birth Frequency of conception among women of childbearing age on dialysis ranges from 0.3 - 1.5 % per year. Management of Pregnant Dialysis Patient • Intensification of dialysis Keep B.U.N. ↓ 50 mg/dl to avoid polyhydramnios. 5 to 7, Hemodialysis sessions with slow rate U.F. minimal heparinization bicarbonate buffer hypotension to avoid volume contraction • Adequate supply of calories and protein Protein intake should be - 1 g/kg per day - Additional 20 g/day for fetal growth. - Supplemented with water soluble vitamins and zinc • Antihypertensive regimen Acceptable antihypertensives include labetalol, Nifedipine XL, methyldopa, and metoprolol. Avoidable antihypertensives Diuretics, ACE inhibitors, ARBs. • Correction of Anemia Give Erythropoietin with Iron & Folic Acid supplemented. Keep Hb % > 10. • Treatment of premature labor The use of β agonists is preferred & NSAIDs should be avoided. • Avoidance of metabolic acidosis • Prevention of hypocalcemia • Reinforced fetal monitoring as soon as viability is reached Common Themes in Dialysing Pregnant Patients 1. Keeping BUN < 50 2. Increasing dialysis time and frequency 3. BP control 4. Managing anemia with increasing doses of ESA 5. Fetal monitoring once viability reached Women who Start Dialysis During Pregnancy • Likelihood of infant surviving is good • Termination of a pregnancy after renal function has begun to deteriorate rarely rescues the kidneys • NEJM, Jones and Hayslett, 1996, looked at 82 pregnancies in 67 women w/CRI, only 15% of those w/deteriorating renal function had a return of renal function to baseline in 6 mths post partum Medications Common medications in CKD/ESRD 1. Erythropoietin Safety issues Comments Safe to use Limited data. 2. Iron Safe to use Low dose intravenous iron recommended 3. Vitamin D Widely used Limited data. 4. Heparin Safe to use Minimize dose of heparin Renal Transplant & Pregnancy Women are advised to wait at least one year after living, related-donor transplantation and two years after deceased transplantation to avoid complications. The renal allograft should be functioning well, with a stable serum creatinine level <1.5 mg/dL (132 micromol/L) and urinary protein excretion <500 mg/day. Common Medications in Kidney Transplantation 1. Prednisone Safe to use Fetal adrenal insuffi ciency 2. Cyclosporine Safe to use IUGR 3. Tacrolimus Not safe to use Severe IUGR, renal failure, hyperkalemia 4.Mycophenolate mofetil Not safe to use Teratogenic in animals 5. Azathioprine Widely used Fetal neutropenia, teratogenic in high doses 6. Polyclonal antibodies Not safe to use Very limited data C.K.D. and Pregnancy – Diabetic Nephropathy • 6% of pregnant women with type I DM have : – overt diabetic nephropathy (<20/40: U prot>300mg/d – macroalbuminuria >300mg/d – alb/creat. ratio >0.3mg/mg) • Effect of nephropathy on pregnancy – prematurity(22%) – IUGR(15%), pre-eclampsia Pregnant women with diabetes & risk of developing kidney diseases With normal albumin With microalbuminuria and normal kidney function With poorly controlled HTN or reduced G.F.R. and S.Cr. > 1.5 mg/dL, proteinuria >3 g in 24 hours) ↓ low risk ↓ low risk ↑ high risk Maternal Complications in Pregnancies Complicated by Diabetic Nephropathy (2001 to 2012) Ekbom P, Damm (Diabetes Care 2001) /Young EC, Pires ML / Carr DB, Koontz GL, Gardella C. Am J Hypertens / Yogev Y, Chen R, Ben-Haroush (Neonatal Med 2010; 23:999) / Nielsen LR, Damm P, Mathiesen ER. (Diabetes Care 2009; 32:38) • Pregnant women with diabetes, microalbuminuria, and normal kidney function appear to be at low risk for loss of kidney function, but may have a transient increase in albuminuria • Women with poorly controlled hypertension or reduced glomerular filtration rate (GFR) and increased proteinuria (serum creatinine level >1.5 mg/dL, proteinuria >3 g in 24 hours) at the onset of pregnancy are at risk of permanent kidney damage, including endstage kidney disease. • Recommended B.P. 110-129/ 65-79 mm Hg Diabetic Kidney Disease Complications • Fetal growth restriction • Abnormal antenatal fetal assessment • Preeclampsia, even in women with good glycemic control. The occurrence of these pregnancy complications may necessitate preterm delivery and increases the chance of cesarean birth C.K.D. and Pregnancy - Lupus • Rate of relapse not different between pregnant women and concurrent controls (9-60%). • Major factor determining a pregnancy related exacerbation is the stability of the disease before conception • If in remission for > 6 months pre-conception, low incidence of clinical flare during pregnancy. • Women with intracranial aneurysms may be at increased risk of subarachnoid hemorrhage during labor. Lupus Flare-up Versus Preeclampsia SLE + + PE + + RBCs cast + - Azotemia Low C3, C4 + + - + +/- Low platelet count + +/- Low leukocyte count + - Proteinuria Hypertension Abnormal liver function test results Causes of Proteinuria in Pregnancy Primary renal diseases • • • • • • • IgA nephropathy Minimal change disease Membranous nephropathy Focal segmental glomerulosclerosis Primary glomerulonephritis Allergic interstitial nephritis Polycystic kidney disease Systemic causes • • • • • • • • • • Preeclampsia Diabetic nephropathy Lupus nephritis (diffuse proliferative, focal proliferative, membranous) Hypertensive nephrosclerosis Thrombotic thrombocytopenic purpura (TTP) Infection-associated glomerular disease (eg, HIV, hepatitis B/C) Systemic vasculitis Multiple myeloma Chronic vesicoureteral reflux Antiphospholipid syndrome • Preeclampsia is the most common cause of proteinuria in pregnancy and must be excluded in all women with proteinuria first identified after 20 weeks of gestation. • If preeclampsia is excluded, then the presence of primary or secondary renal disease should be considered. Criteria for the diagnosis of preeclampsia Systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg on two occasions at least four hours apart after 20 weeks of gestation in a previously normotensive patient If systolic blood pressure is ≥160 mmHg or diastolic blood pressure is ≥110 mmHg, confirmation within minutes is sufficient and Proteinuria ≥0.3 grams in a 24-hour urine specimen or protein (mg/dL)/creatinine (mg/dL) ratio ≥0.3 Dipstick 1+ if a quantitative measurement is unavailable In patients with new-onset hypertension without proteinuria, the new onset of any of the following is diagnostic of preeclampsia: Platelet count <100,000/microliter Serum creatinine >1.1 mg/dL or doubling of serum creatinine in the absence of other renal disease Liver transaminases at least twice the normal concentrations Pulmonary edema Cerebral or visual symptoms Adapted from: Hypertension in pregnancy: Report of the American College of Obstetricians and Gynecologists' Task Force on Hypertension in Pregnancy. Obstet Gynecol 2013; 122:1122. Graphic 79977 Version 9.0 Women with Nephrotic Syndrome • Discomfort from severe leg edema can be managed with sodium restriction (1.5 g, approximately 60 mEq), bedrest, and leg elevation. • Prophylactic anticoagulation is reasonable in pregnant women with nephrotic syndrome and severe hypoalbuminemia (serum albumin <2.0 mg/dL, or <2.8mg/dL in membranous nephropathy), especially if another risk factor (eg, bedrest) is present. • Bile acid sequestrants and fibrates can be safely used in pregnancy to treat severe hyperlipidemia due to nephrotic syndrome; statins should be avoided. Kidney Biopsy During Pregnancy • There are few Indications for Kidney Biopsy s • May be performed if there is a sudden unexplained deterioration in renal function or markedly symptomatic nephrotic syndrome occurring before 32 weeks gestation. • Biopsy after week 32 is not recommended. The Treatment for Pregnancy Associated AKI • Preeclampsia-associated AKI is an indication for delivery. Delivery generally results in completely recovery of renal function, although moderately increased albuminuria may persist. • TTP-HUS-associated AKI is primarily treated with plasma exchange. • AFLP-associated AKI includes the treatment of disseminated intravascular coagulation (DIC) and delivery of the fetus. Hypertension • In women with chronic primary or secondary hypertension or previous pregnancy-related hypertension, low-dose aspirin from the 12th week of gestation until delivery is suggested, but should be determined on a case-by-case basis. Thank You