Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
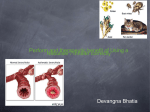
F or last 4000 years it is known that inhaled therapy for treatment of lung diseases is superior to oral therapy. However, making an ideal inhaler has been excessively challenging mainly because of difficulty in achieving appropriate particle size required for lung deposition and making a safe medication that does not lead to bronchoconstriction or large systemic absorption. Invention of hundreds of inhalers over last 4000 years has led to the effective and safe inhalers of present day. India is fortunate to have the widest range of inhaled products available at cheaper costs compared to rest of the world. Unfortunately, many patients having obstructive lung diseases still continue to rely on oral therapy or use inhalers incorrectly. The major reasons are inadequate knowledge and awareness of the prescribing physician, lack of adequate patient education and cost of inhalers. This issue of Respimirror covers some excellent articles discussing clinically important issues related to inhalation therapy. Compared to oral therapy, delivery of drugs by inhalation leads to rapid and direct deposition of the drugs into the airways which allows high local drug concentrations and limits systemic toxicity. Hence, inhaled aerosol therapies administered mainly through dry powder inhalers (DPI), metered dose inhalers (MDI) and nebulizers are the mainstay of treatment of obstructive lung diseases. However, in order to have adequate therapeutic efficacy patients must be able to use the proposed device effectively. Studies have shown that improper inhalation technique and Drug Launcher Dr. Rahul Kodgule, CRF “We contend that no remedy, or combination of remedies, however potent, whether allopathically or homeopathically administered through the medium of the stomach has ever nor can ever cure a single case of asthma. For the reason that they do not reach the seat of the disease, their principal force is spent upon the general system, and long before they find their way to the lungs, their power is lost.” - Charles Broadbent, 1862 poor drug compliance are important causes of loss of symptom control in asthma. A reduction of 25% (due to poor compliance or improper inhaler technique) in the time of usage of inhaled steroids doubles the rate of hospitalization for asthma. Poor compliance with treatment is the most important cause (responsible for 61%) of deaths due to asthma. Hence, educating the patient about the disease, the importance of treatment compliance and ensuring proper inhaler technique are the cornerstones of successful management of obstructive lung Nitin Vanjare, CRF A vians are adapted to fly at great heights and for longer durations. e.g. the Amur Falcon can fly from Nagaland to South Africa over a two months period, including a nonstop flight for 3½ days over the Arabian sea. How do they manage to do this, so efficiently? The answer is their efficient and unique respiratory system. Their lungs are small and rigid, they do not have a diaphragm but a network of air sacs instead, no alveoli are present gas exchange occurs in air capillaries. The respiratory system takes up about one fifth of its body weight and the presence of air sacs makes the bird light in weight and makes flying an easier task. The air sacs act as bellows, which help in moving air in and out of the respiratory system due to the pressure changes in the air sacs. In birds, the air travels through the lungs in one direction (unidirectional) unlike humans where the air travels in and out of the lungs by the same pathway (bidirectional flow). Respiratory system of birds is more efficient compared to humans i.e.more oxygen is transferred with each breath. Along with oxygen the toxins in air also get transferred more efficiently in the system. This is one of the possible reason why Teflon fumes are toxic to birds but not to humans at the same concentration. diseases. A complete prescription for asthma or COPD does not end by signing over it but has to end by proper choice and training of inhalers. Choosing a right inhaler for the patient is like finding a matrimonial match. All the forms of inhaled therapy have equivalent efficacy and hence, patient preference plays an important role in choosing the inhaler. However, all the aerosol inhalation devices have their own strengths and limitations. Dry powder inhalers (DPI) are the easiest for the patients to understand and use, and consume least time to train. Being breath-actuated, DPIs lead to a more reliable drug delivery with minimal training. Inhalation technique mainly involves fast inhalation right from the beginning and complete inhalation. However, proper use of a DPI requires the patients to have adequate inspiratory flow rates (>30 L/min) which can be measured using an inspiratory flow meter/in-check dial. Patients with very severe obstruction and children below 5 years of age may not be able to generate adequate inspiratory flows to effectively use the DPI. Metered dose inhalers (MDI) can be used by patients with any severity of disease. Inhalation technique mainly involves slow and complete inhalation followed by a breath-hold of about 10 seconds. Effective use of MDIs requires proper coordination during actuation and inhalation. Hence, many patients fail to use the device effectively. Another important problem with >>Continued on page 8 Breathing in Birds Fig : It takes two full inhalation-exhalation cycles for a specific volume of air (blue) to pass through bird lungs. Adapted from Bretz and Schmidt-Nielson, 1972 |Volume IV, Issue I, January 2014|RespiMirror 1 History of inhalation therapy I Ancient chinese treatment for asthma nhalation route is the safest, fastest and most effective way to administer drugs in patients suffering with asthma and chronic obstructive pulmonary disease (COPD), and should be the method of choice in these patients.” These are guidelines stated by the Global Initiative for Asthma (GINA) and the Global Initiative for Chronic Obstructive Lung Disease (GOLD). And yet, several years before these guidelines were even thought about, the inhalation route of therapy existed. Inhalation therapy in ancient times: Roman Bath It is interesting to learn how inhalation therapy actually evolved to what we know of it today. The very first traces of inhalation therapy were seen in China in 2600 BC. Inhaling fumes of Ma Huang was the prevalent treatment then for asthma. It is now known that Ma Huang actually contains ephedrine, a potent bronchodilator. Around the same time, ancient India practiced the inhalation of fumes from burning Datura Stramonium and hemp, a potent anti-cholinergic (scopolamine). As early Dr. Komalkirti Apte, CRF fumes to relieve asthma symptoms was strongly advocated in 1802 which led to the invention of asthma cigarettes. These were in use until recently (1985). However, the first concept of a device for inhalational route of therapy was conceptualized in 1654 by the English physician Christopher Bennet. It bore a striking resemblance to the Turbohaler® in markets today. A little over a century later (1764), another English physician, Philip Stern stated the use of inhalation route of treatment for lung ailments. In the next decade, English physician, John Mudge described his invention of an inhaler to be used for the treatment of a catarrhous cough using opium vapors. The concept of this inhaler was to add opium extract to boiling water in a pewter tankard with a lid and a mouthpiece or vent through which the patient would inhale the vapors. The early 1800s brought in easier ways to advocate inhalation therapy. Cavallo suggested the use of a teapot for holding the boiling liquid and the subsequent fumes and the Ancient Inhaler Ancient Greek treatment for asthma: inhalation of fumes Asthma Cigarettes made with rolled ‘dhatura’ leaves 2 RespiMirror|Volume IV, Issue I, January 2014| as 1554 BC, ancient Egyptian Ebers papyrus has shown evidence of inhalation of vapors of black henbane (hyoscyamine), again a potent anti-cholinergic. Roman Baths, natural hot water springs in England, were a site of treatment for several centuries since 836 BC. Geothermal energy in the area heated the percolated rain water to high temperatures. This heated water would surface through fissures and faults in the surrounding limestone along with fumes infused with various minerals and chemicals. Patients with respiratory complaints as well as arthritic complaints benefitted immensely from bathing at these hot springs. Hippocrates (460-377 BC), in ancient Greece, advocated the inhalation of vapors of herbs and resins boiled with vinegar and oils through a tube. Almost 10 centuries later, Rhazes (c850 AD – c923 AD), a physician in Baghdad, advocated the inhalation of arsenic vapors for medical treatment. At the end of the 12th century (1190 AD), a Spanish physician Maimonides wrote the first book on the treatment of asthma which included inhalation of vapors generated from herbs thrown into a fire. The invention of inhaler devices: The ancient Indian practice of burning of Datura Stramonium and inhalation of the spout for inhaling the vapors. This seemed to be the inspiration for the subsequent Nelson’s inhaler in 1865. Pressurized metered dose inhalers: The first powdered or pressurized inhaler was invented by a French physician Sales-Girons in 1858. It involved the use of a holding chamber which housed the liquid medication. A pump handle mechanism similar to a bicycle pump propelled the liquid medication through an atomizer based upon the force of use. A similar technique was used in the rubber bulb vaporizer. The glass top is removed to add the drops of medication into the rubber bulb. After re-arranging the instrument, the rubber bulb is squeezed to vaporize the liquid medication for use through the inhalational route. The inhalational route of therapy gained worldwide acceptance post a medical treatise from the American physician Charles Broadbent which stated that “the soothing and quieting effects of these vapors is brought immediately to act upon the parts locally irritated and diseases, by gentle inhalation of the vapor from a bottle arranged expressly for the purpose”. In 1926, Erik Rotheim, a Norwegian engineer, came up with a spray can which would effectively >>Continued on page 3 >>Continued from page 2 English physician Christopher Bennet and his drawing of an inhaler. deliver liquids in an aerosolized manner. He used this technique primarily for spraying insecticides in farms. Philip Meshberg developed a special valve called as the Meshberg valve. This valve emitted a fixed dose of aerosol at every actuation. This technology was then used in hair spray cans and perfume sprays. A young 13 years old, Ms. Susie Mason, a known asthmatic used the rubber bulb vaporizer in that era. Invariably, she would break the apparatus very often prompting her father to buy a new vaporizer every week. She had observed her mother use hair sprays which was made of metal and had the Meshberg valve. In frustration, after having broken her umpteenth vaporizer, she retorted to her father to put her medicine in the metal and valved spray can which her mum used for her hair. This spearheaded the revolution in inhalation therapy. Her father was a chemist with Riker industries, now 3M Pharmaceuticals. Inspired by his daughter’s demand, Mason along with Charles Thiel, developed the first cold fill pressurized metered dose device (pMDI). They used an old cola bottle, a Meshberg valve and Freon from an old refrigerator as the propellant. This device was then used for the first time as an inhaler device for the drug Vitamin C. By 1956, isoprenaline and adrenalin were approved for use through the pMDI and were marketed as Medihaler-iso and Medihaler-epi respectively. Dry powder devices: The first dry powder inhaler was patented in 1864 by an English physician Newton. He had then observed that the powder to be used in this manner needed to be very finely pulverized and kept dry at all times. Today, we know that these are the prerequisites of all dry powder inhalers. Frederick Roe patented another dry powder device called the Carbolic Smoke Ball. This could be refilled at repeated intervals. Soon dry powder devices were also patented. The first to arrive in the market were rotahalers (single dose) and diskhalers (multi dose). The single dose inhalers evolved from every pharmaceutical company. Today there is a wide range of single dose dry powder inhalers such as revolizer, handihaler, lupihaler, redihaler and many more. Complications of recharging English physician John Mudge and his pewter for every dose were tackled by inventing a tankard inhaler which contained hot medicated water device which could store a certain number of doses. This brought about a revolution in dry powder inhalers. These newer devices were called multi dose inhalers and today we have a large variety of multi dose dry powder inhalers such as accuhaler, easyhaler, novolizer, turbohaler, multihaler and more. Nebulizers: Nebulizer therapy also initiated in the early 1860’s. The story of the hot springs is what brought about a revolution in nebulizer therapy. As mentioned previously, patients with respiratory and arthritic complaints benefitted immensely from the fumes emitted at the hot springs. Some patients however could not reach the hot springs due to their disease conditions. This is when people then began to transport the water from the hot springs to the patient. A pump would infuse the chemical and minerals into the water before the patient would inhale the steam. German physician, Siegle patented the steam spray which used the Venturi principle to atomize liquid medication. This was the first form nebulization. The effect of the droplet size on the lung penetration was noticed in 1878. Today, we have come a long way to understand the correct droplet size for effective nebulization. Inhalation therapy has come a long way in the past centuries. Newer and improved devices are being invented and would be in the public domain soon. This has drastically improved patient outcomes in the field of obstructive airway diseases. First pMDI Carbolic Smoke Ball First Nebulizer |Volume IV, Issue I, January 2014|RespiMirror 3 DO DOCTORS KNOW HOW TO USE INHALERS CORRECTLY? Dr. Sneha Limaye, CRF D espite the great benefits offered by the wide range of aerosol therapy available in country, a huge percentage (more than 70%) of Asthma & COPD patients are never prescribed inhaled medications. A major reason for this can be attributed to the fact that many doctors themselves are unaware of the correct inhaler techniques. Inefficient inhaler technique is a common problem resulting in poor drug delivery, decreased disease control, non adherence and increased inhaler use ultimately resulting in shifting the patient back to oral therapy for control and management of symptoms. Chest Research Foundation conducted a study amongst qualified and in-training doctors and nurses from a tertiary care teaching hospital in Pune to understand their knowledge, skill and perceptions about inhaler use. The study group consisted of 100 final year MBBS students, 100 Interns, 50 PostGraduate Students (Medicine, Pediatrics and Chest), 107 qualified nurses and 53 qualified physiotherapists. Every participant was given a placebo inhaler and requested to demonstrate the technique of using a pMDI and scoring was done to see if every step was followed properly. A questionnaire was used to understand their perceptions about inhaler use. In a shocking revelation, about 50% of the doctors, nurses and physiotherapist believed that inhalers were addictive. It was more worrying to learn that less than 1 percent of the entire study population (doctors and nurses) knew how to use an inhaler correctly. The best were the postgraduate students of respiratory medicine. 9% of them knew how to use inhalers correctly. If majority of the doctors believe that inhalers are addictive and less than 1% know how to use a pMDI correctly, one can only imagine what must be happening in clinical practice. Doctors need to be educated about how to use inhalers correctly and their importance in the management of asthma STEPS FOR MDI USE and COPD. Many doctors complain time of constraints due to busy OPD and patient care and despite understanding the need for communication and patient training on devices, are not able to devote enough time to explain the correct techniques. The most feasible solution for this is train your nurse or hire and train an educator for your clinic/ hospital. Any of the existing staff members can also be identified and trained by the doctor in correct use of inhalers and devices. Once the doctor has written a prescription, the nurse/ educator can spend the required amount of time in training the patient on the prescribed inhaler device and also counsel the patient to dispel the myths associated with inhaler use. STEPS FOR DPI USE 1. Remove protective cap and shake the inhaler 1. Prepare the inhaler before usage 2. Hold inhaler upright 2. Keep inhaler horizontal 3. Exhale to residual volume 3. Exhale to residual volume 4. Place mouthpiece between lips and teeth 4. Place mouthpiece between lips and teeth 5. Inhale slowly and simultaneously activate the canister 5. Inhale forcefully and deeply 6. Continue slow and deep inhalation 6. Take the inhaler out of the mouth 7. Hold breath for 5-10 Sec 7. Hold breath for 5 s Practical Updates for Respiratory PGs via Web 16th Purview Announcement Topic: Systemic Manifistations of COPD Date :15th March 2014 Time : 5 to 7.30 pm 15th Purview on Obstructive Sleep Apnoea, CRF, Pune, 4th Jan 2014 4 RespiMirror|Volume IV, Issue I, January 2014| log on to www.crfindia.com to attend this webcast O Types of Inhaler Devices Ms. Monika Chopda, CRF ne of the biggest advancements in the management of Obstructive Airways Diseases has been the delivery via the aerosol route. This has revolutionised the way asthma and COPD are treated. One of the earliest inhaler devices to be introduced was the nebulizer. Subsequently the dry powder inhalers and metered dose inhalers were developed, and more recently the small volume nebulizers have been introduced to deliver drugs directly to the airways. There are at least 65 different types of inhaler devices that are available through which one can deliver at least 20 different types of drugs including short, long and very long acting betaagonists, anticholinergics and steroids for the treatment of asthma and COPD. This route of delivery is also used to administer antibiotics to the lungs as well as insulin, other hormones and anaesthetics. The principle 4 types of inhalation devices that are widely used are: 1. Metered dose inhalers ( MDI) 2. Dry powered inhalers (DPI) 3. Small volume Nebulizers 4.Nebulizers 1. Metered dose inhalers (MDI): This is the most widely available and used inhalation device for the treatment of OAD’s. It contains propellants, surfactants, solvents, ethyl alcohol & the active drug. The active drug is either in a solution or suspension under pressure. On activation, the metered valve dispenses a fixed volume of the suspension or solution. MDI’s contain between 100-200 doses that can last for one to several months. MDI’s are small, easy to carry and relatively cheap (cost per dose) than other inhaler devices. Facts of inhalers 1) Speed : The speed with which plume comes out after activation is 160km/h. One needs to co-ordinate inhalation with actuation, which not many people can do effectively. 2) Temperature of plume: The temperature at which the drug comes out from pMDI after actuation is -20°C. If you put your finger you will feel the temp -20 degrees. When the plume comes Pressurized MDI Physical Components Metal Can Elastomers Valve Actuator Formulation Drug Substance Propellants Surfactants/ Co-solvents Canister Plastic Mouthpiece Metering Valve Spray Orifice out it has a temp of 0°C. This low temperature is the reason for Cold Freon effect of pMDI’s. This temperature may cause bronchospasm in some patients leading to sudden cough after taking inhaler. 3) Propellant: The Propellant are the most important parts of the inhaler. One of the most commonly used propellants over the years has been chlorofluro carbon or CFC. It is also used in whole host of other industries. In the 1980’s it was realized that because of the widespread use of CFC’s, there was an Ozone hole formed in the Stratosphere. This is because CFC’s deplete ozone and the ozone layer in the stratosphere protects us against the UV radiation from the sun. As a result, a resolution was made that CFC’s will be phased out from all the industries including inhaler industry. It is nowadays mandatory to manufacture all MDI’s with a non CFC propellant. Now use of CFC has been actually shown to be harmful to the earth because it can cause Ozone hole in the Stratosphere. Because of this all CFC propellants are replaced with non CFC propellants. One of the newer non CFC propellants used is HydroFluoroAlkane (HFA). Many of you may have started using inhalers with the HFA propellant. There are three important points one should know while shifting a patient from CFC inhaler to HFA inhaler. Advantages of HFA over CFC 1) Different taste: HFA MDI’s contain a small amount of ethanol. Adding ethanol changes the active properties of meter dose inhaler like the taste of the inhaler, speed of the plume etc. There are chances that patient may complain that the new HFA inhaler tastes different. Plume will tests sour & the speed with which plume comes out is much slower in HFA propellant as compare to CFC because of ethanol contained in it. 2) Plume is warmer (less cold Freon effect): The plume from HFA inhaler is warmer as compare to the plume from CFC inhaler. Due to this patient feels less cold Freon effect with HFA inhaler as compare to inhaler with CFC propellant. (1, 2 are the important differences patients will notice when the inhaler is changed from CFC to HFA propellant). 3) After 12 wks change the HFA inhaler: It is also important to know that all HFA propellants need to be stored at 0-4degre before they are dispensed. Once it is dispensed at room temperature they should be ideally used within 12 weeks because their shelf life remains only for that period of 12 weeks. After 12 weeks it is wise to change the inhaler. Speed with an MDI needs to be inhaled: It is important to appreciate the fact that while using pMDI the inhalation should be slow & deep. How to overcome co-ordination problem? To overcome the co-ordination problem & to improve deposition different types of accessory devices and advanced inhalers are developed like Spacer, Neohaler, and Breath activated MDI’s. a. Spacer: Many patients can’t coordinate actuation with inhalation so there is need of an accessory device called as a spacer. Spacers |Volume IV, Issue I, January 2014|RespiMirror 5 make aerosol inhalers easier to use and more effective. Spacer traps the medicine inside, so patients don’t have to worry about pressing the inhaler and breathing in at exactly the same time. There are two types of spacer, a large and small volume. The material of the spacer can be static or non-static. Now-a-day’s non-static inhalers are widely used. On page 9, Dr. Monica discusses this in detail. b. Neohaler: It has a small spacer like chamber at the bottom which actually reduces the speed of the drug that comes out. c. Breathe Activated MDI’s: Recently breathe activated inhaler devices has been introduced to overcome the problems of co-ordination. These are called as Breath activated metered dose inhaler. The patient needs to activate the device by pulling the red tag upwards & when patient start inhaling; device automatically releases single dose of the drug. So there is no question of bringing up co-ordination with this device. medication solution is forced through it, two fine jets of liquid are produced. The two jets of liquid converge at an optimised angle, and the impact of these converging jets generates the soft mist. This mist is extremely fine (the majority of the droplets fall into the fine particle fraction of 5.8 µm average). It moves slowly, which is the basis for many of its potential benefits. It has high lung deposition with the Soft Mist Inhaler Mouthpiece Uniblock Dose-release button Capillary tube Upper housing 2. Dry Powder Inhaler (DPI): DPI is a device used for generation of aerosol powder by the patient’s inspiratory effort. First DPI used was with penicillin to treat pneumonia a way back. Now whole host of DPI’s are available. In the DPI’s the drug is mixed with a powder, usually lactose, and then it is packed in gelatin capsules. After breaking or piercing the capsule releases the power. Then patient needs to breathe in rapidly. Due to the air currents generated by the patient’s breath, the drug particles get deaggregated and are carried into the lungs along with the inspired air. DPI is available in unit dose & multidose. Dry Powder Inhaler Hole for inserting rotacap Mouthpiece Tin Rota Chamber DPI has unique advantages over PMDI: • DPI’s doesn’t require coordination after activation, • DPI’s doesn’t contain CFC so it is environmental friendly • Many people find it is very easy to use The only problem with DPIs is that patient needs to generate sufficient energy to suck this drug into the airways. Patient needs to inhale with more force to bring the drug out. Particles in powder are aggregated; the only way they will deaggregate in smaller size is by the force inspiratory efforts. 3. Small Volume Nebulizers: Small Volume Nebulizers (Soft Mist Inhaler) has a unique delivery mechanism, which is propellant-free and delivers a metered dosage of medication as a fine mist. It is the nozzle system that provides the Soft Mist. When the 6 RespiMirror|Volume IV, Issue I, January 2014| Transparent base Spring Cartridge associated reduced oropharyngeal deposition and no requirement for forceful inspiration. Due to the very low velocity of the mist, the Soft Mist Inhaler in fact has higher efficiency compared to a conventional MDI. 4. Nebulizer: Nebulizers use oxygen, compressed air or ultrasonic power to break up medical solutions and suspensions into small aerosol droplets that can be directly inhaled from the mouthpiece of the device. The definition of an aerosol is a “mixture of gas and liquid particles,” and the best example of a naturally occurring aerosol is mist, formed when small vaporized water particles mixed with hot ambient air are cooled down and condense into a fine cloud of visible airborne water droplets. The liquid drug to be nebulized is put in the nebulization chamber, which is then attached to the compressor with the help of a connecting tube. A mask or a mouthpiece is then attached to the chamber to aid inhalation. The mist thus generated is inhaled by the patient either through the mouth using a mouthpiece or through the nose, using a face mask. The first “powered” or pressurized inhaler was invented in France by Sales-Girons in 1858. This device used pressure to atomize the liquid medication. The pump handle is operated like a bicycle pump. When the pump is pulled up, it draws liquid from the reservoir, and upon the force of the user’s hand, the liquid is pressurized through an atomizer, to be sprayed out for inhalation near the user’s mouth. In 1864, the first steam-driven nebulizer was invented in Germany. This inhaler was known as “Siegle’s steam spray inhaler”. The first electrical nebulizer was invented in the 1930s and was called a Pneumostat. In 1964, a new type of electronic nebulizer was introduced: the “ultrasonic wave nebulizer”. Types of Nebulizers: a. Large volume Nebulizers Large volume nebulizers are used to turn liquid in to the mist so that it can be inhaled or to deliver the mist required to moisturise the patient’s airways in the patients with thick, tenacious secretions, with any of the following indications: a) Administration of pentamidine to patients with HIV, pneumocystosis, and complications of organ transplants b)Bronchiectasis c) Cystic fibrosis d) Tracheobronchial stent e)Tracheostomy A large volume nebulizer and related compressor are considered experimental and investigational for all other indications because their effectiveness for indications other than the ones listed above has not been established. b. Jet nebulizer The most commonly used nebulizers are Jet nebulizers, which are also called “atomizers”. They use compressed air to generate a fine mist. Jet nebulizers are commonly used for patients in hospitals who have difficulty using inhalers, such as in serious cases of respiratory disease, or severe asthma attacks. The main advantage of the jet nebulizer is its low operational cost. The noise (often 60dB during use) and heavy weight are however still the biggest drawbacks of the jet nebulizer. c. Ultrasonic Nebulizers Ultrasonic wave nebulizers were invented in 1964 as a new more portable nebulizer. An ultrasonic nebulizer does not use compressed air; instead, an ultrasonic nebulizer uses high frequency vibrations to aerosolize the medication into a very fine mist. Since ultrasonic nebulizers don’t compress air, they operate very quietly, tend to be much smaller in size, and can fit in nearly any container. The only drawback is medication restrictions because heat is transferred to the medication Which is a better device? There are so many different types of inhaler devices available. From an efficacy point of view all of them are similar. They all produce the same effect. If patients can not generate sufficient inspiratory flow then DPI will be less helpful similarly if co-ordination is not good only MDI will be less effective so pMDI can be used with spacer. Now a day’s one good replacement to MDI plus spacer is use of breathactivated meter dose inhaler. Pooled meta-analysis of 394 clinical trials between the years 1982 – 2001, showed that there is no significant difference between devices in efficacy outcome & in patient group for each of the clinical settings that were investigated. Both study groups showed similar adverse event profile. Let the patient decide which inhaler to be used because 1) if a patient does not like the inhaler device or is unable to use it correctly, it is useless. 2) A preferred device that is taken by the patient and is effective represents a better value for money. How inhalers are made? Introduction Pharmaceutical aerosols have been playing an important role in the health and well being of millions of people throughout the world for many years. The origin of inhaled therapies can be traced back 4000 years ago to India, where people smoked the leaves of the Atropa belladonna plant to suppress cough. In the 19th and early 20th centuries, asthmatics smoked asthma cigarettes that contained stramonium powder mixed with tobacco to treat the symptoms of their disease1. People suffering from chronic obstructive pulmonary disease (COPD) or other lung conditions often take their medications through inhaled drug delivery systems. Administration of drugs by the pulmonary route is technically challenging due to high oral deposition and variations in inhalation technique which can affect the quantity of drug delivered to the lungs. Therefore, there have been considerable efforts to provide more efficient and reproducible aerosol systems through improved drug delivery devices and through better formulations that disperse more readily during inhalation. Formulation Design Metered dose inhaler formulation The pressurized Metered Dose Inhaler (pMDI) consists of a pressurized canister inside an actuator. Drugs in pMDIs take the form of either particulate suspensions or solutions. The pMDI comprises several components each of which is important to the success of the whole device as shown in Fig 1. Fig. 1. Schematic of typical pressurized Metered-dose inhaler. Invited article by Ms. Geena Malhotra, Ms. Pragati Rege, Cipla process. The most useful technique to reduce particle size is by Jet milling (or air-attrition milling). The pMDIs are formulated with chlorofluorocarbons (CFCs) propellants along with micronised active ingredients but current global regulations require pharmaceutical aerosols to be reformulated to contain non-ozone-depleting propellants. The two current alternatives to CFC propellants for pharmaceutical aerosols are hydrofluorocarbon (HFC) 134a (also known as hydrofluoroalkane (HFA) 134a or 1,1,1,2- tetrafluoroethane), and HFC-227ea (HFA-227a or 1,1,1,2,3,3,3heptafluoropropane)2. Advantages: • Small size, portable, unobtrusive • Quick to use • More than 100 doses available • Pressurization of contents protects against moisture and bacteria Disadvantages: • Require propellants • Drug delivery highly dependent on good inhaler technique • Possible to get no drug in lungs with bad inhaler technique • Most products have low lung deposition • Most products have high oropharyngeal deposition Dry powder inhaler formulation Development of Dry Powder Inhalation Formulation (DPI) is of a particular challenge, as it involves the preparation of a formulation and the selection of a device for aerosol dispersion (Martin et al Respiratory care; September 2005; Vol 50;No 9). DPIs were designed to eliminate the co-ordination difficulties associated with the MDI ( Labiris et al. Br J Clin Pharmacol.56, 600–612).DPI medications are taken in the form of a dry powder, using a dry powder inhaler, which is also a handheld device. A DPI delivers medication to the lungs as you inhale through it. It doesn’t contain propellants or other ingredients. There is a wide range of DPI devices in the market, from single-dose devices loaded by the patient (e.g. Rotahaler) to multiunit dose devices (e.g. Diskus, MultiHaler) or reservoir-type (bulk powder) systems (e.g. Turbuhaler). Most DPI formulations consist of micronized active ingredient (particles below 5 micron process by jet milling) blended with larger carrier particles (preferably Lactose), which enhance flow, reduce aggregation, and aid in dispersion. A combination of intrinsic physicochemical properties of lactose with active ingredient such as particle size, shape, surface area, and morphology affects the forces of interaction and aerodynamic properties, which in turn determine fluidization, dispersion, delivery to the lungs, and deposition in the peripheral airways. When a DPI is actuated, the formulation is fluidized and enters the patient’s airways. Under the influence of inspiratory airflow, the drug particles separate from the carrier particles and are carried deep into the lungs, while the larger carrier particles impact on the oropharyngeal surfaces and are cleared. Advantages of the Dry Powder Inhaler • Environmental sustainability, propellant- free design • Requires less patient coordination required Disadvantages of the Dry Powder Inhaler • Deposition efficiency dependent on patient’s inspiratory airflow • Potential for dose uniformity problems • Development and manufacture more complex/expensive Assessment of drug delivery The inhalation aerosol formulations are characterized to find out its physicochemical properties with the suitable analytical method. Crystallanity of the micronised active ingredient drug particles is examined by X-ray diffraction and by Differential Scanning Colorimetry. Particle size and its distribution are measured with laser diffraction techniques. Fig. 2. Principle of dry powder inhaler design. These key components are: • API (micronized Active Ingredient) • Surfactant, bulking agent & Co-solvent (Optional) • Propellant (CFC’s, HFA134a/HFA227) • Container • Metering valve • Actuator The quality of pMDI & DPI could be influenced by a variety of factors associated with these components, of which particle size of the micronized active ingredient is a key factor, because particles below 5 microns are required for lung deposition. To create particles in the expected size range of below 5 micron diameter, the active ingredient undergoes micronization Powder Reservoir (e.g. Turbuhaler) Blister disk (e.g. Rotadisk) Passive Active Blister strip (e.g. Diskus) Capsule (e.g. Rotahaler) Formulation Metering Dispersion Passive/Active Oropharyngeal Deposition Pulmonary Delivery |Volume IV, Issue I, January 2014|RespiMirror 7 Particle morphology is measured by scanning electron microscopy. Water content in the blend is measured by using Automatic Karl-Fischer Titrator. Dosage unit sampling apparatus (DUSA) is used for sampling and testing of dry powder inhaler. Drug content and solubility is analyzed with LC-MS, HPLC, UV or other suitable system. Bulk density, Tap density, and Carr’s index have to be determined to evaluate powder flowability(Kumaresan Pharma Times - Vol. 44, No.10, October 2012). Conclusion: Fig. 3. Anderson Cascade Impactor - Simulation of the Human Respiratory System Does drug deposition affect clinical decision making? P Inhalation is the preferable way of drug delivery to the respiratory tract for the treatment of respiratory disease. The choice of inhaler device is most important in the treatment of asthma and COPD. Dr. Rahul Kodgule, CRF hysicians are often confronted with marketing efforts from pharmaceutical companies claiming better drug delivery through their device. Almost all the dry powder inhalers (DPI) and metered dose inhalers (MDI) deliver about 5-25% or even more drug into the lungs if used properly. The question often arises whether an inhaler delivering 25% drug into the lungs is better than the inhaler delivering only 10% (note: deposition in lung means deposition below vocal cords). Hundreds of studies and dozens of meta-analyses have clearly found that the differences in devices or particle deposition do not affect symptoms, lung function and exacerbation/hospitalization risk. Most of the studies, comparing several devices having different percent particle deposition in the lung and when used to deliver same dose of bronchodilator, found that the improvement in symptoms and lung function is same with any of the device. As a result differences in the amount of drug deposition are presently irrelevant. Hence, choosing an inhaler with better lung deposition is not as important. What matters to some extent, is the distribution of deposition of drug particles in the lungs. Larger particles are deposited in the upper respiratory tract and larger airways while smallest ones reach the lower airways and alveoli. Large and mid-sized airways have larger smooth muscle mass and are more amenable to bronchodilator effects. Hence, targeting larger airways with bronchodilators having larger aerodynamic diameter (size) may be a useful strategy. It is shown that as the aerodynamic diameter of the bronchodilator particle increases (maximum up to 10µg) the bronchodilator response increases. Most of the available inhaled bronchodilators have similar sized particles and hence there is hardly anything to choose from. However, the opposite is true with corticosteroids. The predominant sites of inflammation in asthma and majorly in COPD are peripheral airways and alveoli. Hence, it is important to achieve delivery of anti-inflammatory drugs in this region. Antiinflammatory molecules of smaller sizes like Ciclesonide and Beclomethasone can reach peripheral lung. In addition smaller molecules are likely to have lesser deposition in upper respiratory tract leading to lesser systemic absorption. However, smaller molecules also get absorbed from the lung in to the systemic circulation leading to systemic effects. Ciclesonide is a pro-drug which gets activated only in the lung and is rapidly eliminated from systemic circulation. This means ciclesonide is likely to be more effective and safe. However, at present there are no well designed clinical trials published that suggest Ciclesonide or Beclomethasone lead to better clinical improvements or are safer than other corticosteroids. In nutshell, inhaler devices are not major determinants of clinical outcomes in patients. Rather, what is known to be most important determinant of clinical outcomes is proper technique of inhaler use and good compliance with inhaled drugs. It has repeatedly been shown that poor inhaler technique leads to lack of control in asthma or poor bronchodilation in COPD. Hence, it is important that the right device is chosen for each patient, the patient should like and understand the device usage, the patient should be effectively able to use the device and the patient should remember the inhalation technique over a period of time. Drug Launcher their use. However, nebulizer use demands only normal tidal breathing and is highly convenient for use in the hospitals. Nebulizers are also least efficient as most of the drug coming out is either lost to the atmosphere or is retained in the nebulizer while only a modest amount (2-4%) reaches lung. During emergencies drugs can be administered with an MDI or DPI in one minute while a nebulizer may take 5-15 minutes for drug administration. another problem which is further compounded by confusion of using several inhalers. This has led to the development of combination inhalers. Combination of rapid and long-acting bronchodilator with inhaled steroid in a single inhaler for asthma and combinations of longacting beta-agonist, long-acting anti-muscarinic and anti-inflammatory drug for COPD are now available. Using combination inhalers has not only been shown to increase therapeutic efficacy, but also improves compliance with therapy. Developing novel and more effective drugs for asthma and COPD appears to be difficult at present. However, a lot of research is taking place to improve the delivery of available drugs to the lungs. Development of newer devices for drug delivery holds promise for better clinical outcomes in these diseases. All the efforts towards developing effective and safe drugs and delivery systems need to be complimented by motivated efforts by the physicians toward improved drug and inhaler acceptance and compliance. >>Continued from page 1 the use of MDIs is that the patients do not know when the inhaler got emptied. Hence, MDIs with dose-counters should be preferred. During actuation of an MDI pressurized propellant expands and evaporates out of the device. This accelerates the drug particles to high speeds (around 33 m/s) and leads to cooling of these particles to temperatures below freezing point. These particles then hit the back of the throat and prematurely stop inhalation causing a “Cold Freon” effect. Use of a spacer along with the MDI prevents the problems related to co-ordination and Cold Freon. In addition, use of spacer also reduces drug deposition in the mouth and hence, any adverse effects related to oral deposition. Use of nebulizers should be reserved for inhospital management. An important problem with at-home use of nebulizers is infection of the device and clogging of the system leading to inefficient drug delivery. Nebulizers are also bulky, expensive and dependent on power for 8 RespiMirror|Volume IV, Issue I, January 2014| Hence, the inhaler devices should be chosen smartly and patients must be trained efficiently. Compliance with inhaler therapy is SPACERS: USEFUL DEVICES FOR INHALATION THERAPY I nhaled medications delivered in aerosol form is widely prescribed for the treatment of Obstructive Airways Diseases, both Asthma and COPD. The Pressurized Metered Dose Inhaler (pMDI) has emerged as one of the most useful devices amongst all the inhaled drug delivery systems and is popular due to its convenience, portability and efficiency. However it comes with its own drawbacks, the most important ones being the need for actuation inhalation coordination, high oropharyngeal deposition and cold-freon effect. Scientists realized that these issues could be overcome by introducing devices which will slow down or space the aerosol dispersion between the patient and the pMDI. Numerous pMDI accessory tubes, cylinder drums and air chambers have been developed to overcome this drug delivery deficiency. Advantages of using a spacer are: 1. Spacers act as holding chambers for the drug once it is actuated thus eliminating the need for actuation inhalation coordination by the patient. The patient can inhale after a delay of a few seconds (not more than 10 seconds). 2. Because of this, spacers are extremely useful for patients of the pediatric as well as geriatric age groups for whom even a dry powder inhaler is a challenge to take. 3. Spacers reduce the aerosol velocity as well as the particle size of the aerosol thus decreasing the oropharyngeal impaction of the drug and reducing the complications of oropharyngeal candidiasis, dysphonia and cold freon effect. 4. Spacers create a more natural respirable flow. By maneuvering medicine past the upper airways spacers help pMDI’s deliver more medicine to the lungs. 5. Spacers have been found to be as effective as nebulizers in controlling an acute exacerbation of Asthma. The modern day spacer which is a valved holding chamber made of non-static material and is transparent has actually gone through several levels of development. Spacers were first developed by Newman et al in 1981 described as extension chambers or holding chambers that decreased oropharyngeal deposition. These spacers were made of various materials including plastic and metal and came in various shapes like accessory tubes, cylinder drums, collapsible bags and air chambers. The holding chambers were of large volumes between 600 to 800 ml. The most widely used shapes and material were cylindrical and plastic respectively. It was later observed that the movement of inhaler-generated aerosols is significantly influenced by electrostatic charge on the particles and on the adjacent surfaces. Spacers and valved holding chambers used with pressurized metered dose inhalers were shown to have electrostatic charge which increases variability in the amount of medication available for inhalation, and hence inconsistent medication delivery. Conditioning the device by washing it with a conductive surfactant (detergent) or by deposition of the drug particles on the surface were some of the earlier methods to combat the loss of drug due to electrostatic charge till scientists came up with the newer non static material which allowed for lesser drug deposition on the walls of the holding chambers. It was once again Newman et al who showed that the deposition of aerosol in the whole lung is improved by using a pear shaped spacer rather than a tubular spacer. Valves were added to spacers to ensure one way flow of the inhaled air. This is important because otherwise, the aerosol particles will absorb moisture from the exhaled air, become heavier and settle down, thus becoming unavailable for inhalation. Thus features of the modern day spacer are as follows: Important practical notes: • • • • Spacers of one company should be used only for pMDIs of the same company to avoid issues of leakage of drug due to improper fitting of the spacer to the pMDI. If two doses are advised using a spacer, the doses should be actuated separately with a gap of 1 minute between the two doses. A spacer should be prescribed even for adults when high doses of inhaled corticosteroids are to be administered. For children less than 3 years, the spacer should be used along with a baby mask. The mask should be held in place for at least one Dr. Monica Barne, CRF minute and the child may breathe normally • When using with a mask, ensure that the child generates sufficient peak inspiratory flow rate to open the valve during inhalation. • In case a child cannot generate sufficient inspiratory flow, the spacer may be tilted upwards slightly so that the valve opens up by gravity and the drug is made available for inhalation. In this case, the spacer would then behave like a non valved spacer. • Children older than 3 years and who can generate sufficient inspiratory flow rate, may hold the mouthpiece in his/her mouth directly without using the mask. • In resource limited and economically challenged settings doctors are tempted to advise the patients to use homemade spacers with the help of plastic/thermacol cups or empty plastic bottles cut into half. When considering the various feature that have been incorporated to develop a most efficient spacer, one may realize how inadequate a plastic bottle may be to be used as a spacer. One should always insist on a proper spacer. • A child should never be given a pMDI without a spacer and only with a mask. Not only will the drug made available for inhalation be reduced but most of the drug will get deposited on the face and in the eyes resulting in complications like thinning and bruising of facial skin as well as ocular complications of steroids. Care and maintenance of spacer devices: It is very important to clean the spacers regularly not only to ensure maintenance of the zero-static coating but also because in some recent studies spacers have been shown to culture Methicillin Resistant Staphylococcal Aureus Bacteria. |Volume IV, Issue I, January 2014|RespiMirror 9 • • • • • • Spacers should be washed under running tap water once every week. No detergents or warm water to be used as they will destroy the electrostatic coating of the spacer. After washing, the spacer should be shaken to remove any excess water. Leave it for air drying indoors. Never should the spacer be wiped dry as this also destroys the non-static coat. The spacer should be changed every 6 months Never do this CRF Programme Calendar Oman Doctors’ Spirometry Workshop, CRF, 12th December 2013 CRF Programme Place Date ICONIC Pune 1st & 2nd February 14 ROAD Jalgaon 15th Feb 2014 Spirometry Simplified Dubai 28th February 14 Spirometry Simplified Muscat 1st March 14 OAD Muscat 2nd March 14 CASPER Dubai 14th March 14 Purview CRF, Pune 15th March 14 Advanced PFT Workshop CRF, Pune 15th & 16th March 14 For more details mail to [email protected] - CRF’s training programmes - - To read the previous issues of Respimirror visit www.crfindia.com - Chest Research Foundation Marigold Premises, Survey No 15, Kalyaninagar, Pune 411014, Maharashtra, INDIA. Phone: +91 20 27035361/66208053 Fax: : +91 20 27035371. Website: www.crfindia.com NOTE : FOR PRIVATE CIRCULATION ONLY. 10 For your feedback / queries write to [email protected] Do you want to conduct a training programme in your city? Please write to Mrs. Monika Chopda at [email protected] Edited by : Mrs. Monika Chopda Published by : Chest Research Foundation, Pune n Printed by : Bookmark Publications, Pune RespiMirror|Volume IV, Issue I, January 2014|