Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
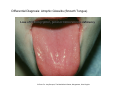
Burning Mouth Syndrome Mariona Mulet, D.D.S., M.S. [email protected] Adjunct Assistant Professor TMD & Orofacial Pain Division Case • 49 y.o. female • Clinical features: Burning, metallic taste, swelling Tongue and lips Intensity: 6-7/10 Duration: 8 months Continuous pain, worsens towards end of the day Pain does not disturb sleep Aggravated by spicy & acidic foods Sudden onset (placement of dental implants) • Prior diagnostic testing: Negative medical examination Normal Hemogram Negative allergy testing • Past treatment: Antifungal Elimination of local irritating factors • Physical examination: Increased anxiety, related to the condition Patient is frustrated and disapointed Normal extraoral exam Normal intraoral exam Burning Mouth Syndrome (BMS) Definition International Association for the Study of Pain (IASP) Burning mouth syndrome (BMS) burning pain in the tongue or other oral mucous membrane associated with normal signs and laboratory findings lasting at least four to six months. International Classification of Headache Disorders II - by the International Headache Society Burning mouth syndrome (BMS) Cranial neuralgias and central causes of facial pain Other used terms: Glossodynia (ICD-9) Glossopyrosis Stomatodynia Syndrome Symptomatic triad & NO SIGNS A. Oral mucosa pain B. Dysgeusia altered taste perception (bitter, metallic, salty, icky) C. Xerostomia A. Pain Quality: Burning, scalded, on fire, numbed Intensity: 5-8/10; constant; progressive through out the day Location: bilateral tongue, palate, labial mucosa B. Dysgeusia Neurosensory testing Decreased pain threshold to heat Changes in CNS or PNS C. Xerostomia 46-67% of patients complain of dry mouth Decreased salivary function not always objectively demonstrated Onset • • • • • Spontaneous – 50% of patients Previous illness Previous dental procedures Medication use Traumatic life stressors Epidemiology • Prevalence: 0.7% (Lipton 1993) – 15% (Tammiala 1993) • Female : male: 7:1 – 16:1 • Age: 38-78 – prevalence increases with age • Duration – average 2-7 years IHS Diagnostic Criteria A. Pain in the mouth present daily and persisting for most of the day. B. Oral Mucosa is of normal appearance. C. Local and systemic diseases have been excluded. Classification • Primary – essential, idiopathic • Secondary – underlying clinical abnormality • Local factors • Systemic factors Local factors • Denture factors • Mechanical irritation • Parafunctional habits Clenching, bruxism, tongue posturing • Allergic contact stomatitis Dental restorations, materials, foods, preservatives, additives, flavorings • Infectious (Bacteria, Fungal, Viral) Systemic factors • Deficiencies Iron (anemia), Vitamin B12, Folate, Zinc, B complex vitamins • Endocrine Diabetes, Thyroid disease, Menopause, Hormonal deficiencies • Hyposalivation • Connective tissue disease Sjogren’s syndrome • Medication ACE inhibitors Anti-hyperglycemic • Esophageal reflux • Depression, anxiety, somatoform disorder Burning Mouth – Primary Two current etiological theories: 1. Taste and sensory system interactions • • • CN V – lingual nerve and CN VII – chorda timpani taste disturbance: abnormal interactions between taste receptors and nociceptors – BMS patients demonstrate chorda timpani dysfunction Supertasters at increased risk 2. BMS neuropathic pain disorder – neural alteration • Peripheral – • altered sensory thresholds upon QST or altered blink reflex Small sensory fiber axon degeneration – histology Central Reduced central pain suppression Central sensitization Major goals for the clinician: • • • • • • • Is the pain nociceptive or neuropathic? • Can a specific diagnosis be made with confidence, and is it the cause of pain? • Is the condition self-limiting or progressive? • Am I able to deliver [evidence based] treatment? • Can I meet the patient’s expectations Differential Diagnosis: Benign Migratory Glossitis © Photos: Dr. Jerry Bouquot, The Maxillofacial Center, Morgantown, West Virginia Differential Diagnosis: Atrophic Glossitis (Smooth Tongue) Loss of filiform papillae, pallor of dorsum in iron deficiency © Photo: Dr. Jerry Bouquot, The Maxillofacial Center, Morgantown, West Virginia Burning Mouth Assessment • • • • Physical examination and history AS INDICATED: CBC w differential and metabolic panel B12, folate, serum iron Burning Mouth - Treatment • Secondary - treat the underlying disorder: irritation, infection, hematologic disorder, objective xerostomia, etc. Burning Mouth: Treatment • PRIMARY (i.e. - neurogenous) Cognitive behavioral therapy Topical medications Systemic medications • Behavioral Interventions Cognitive behavioral therapy • Topical Therapy clonazepam lidocaine capsaicin • Systemic Therapy nortriptyline, amitriptyline (tricyclic antidepressants) paroxetine, sertraline (SSRIs) Amisulpride, Levosulpride (atypical antipsychotic agents) clonazepam (benzodiazepine) gabapentin (anticonvulsant) alpha-lipoic acid (antioxidant) capsaicin Summary • Greater prevalence in females, in post-menopausal ages. • Identification of cause and associated risk factors may help in identification of effective tx strategies. • Alternatively, symptoms could be treated according to underlying neurophysiological mechanisms. • There is increasing evidence suggesting alterations in the PNS or CNS, specific to taste or nociceptive pathways. Thank you!