Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Eradication of infectious diseases wikipedia , lookup
Marburg virus disease wikipedia , lookup
Oesophagostomum wikipedia , lookup
Gastroenteritis wikipedia , lookup
Onchocerciasis wikipedia , lookup
Leptospirosis wikipedia , lookup
Chagas disease wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Leishmaniasis wikipedia , lookup
Schistosomiasis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
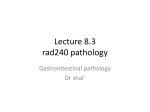
13 Stomach and Proximal Duodenum: Inflammatory and Miscellaneous Disorders Chapter Outline CLASSIFICATION OF GASTRITIS AND GASTROPATHY Current Classification of Gastritis GASTRITIS Distinctive (Specific) Types of Gastropathies Reactive (Predominant Epithelial) Changes Reactive gastropathy Toxic gastropathy Reactive Changes with Erosions in Helicobacter—One or Two Diseases? Distinction of Reactive Changes from Dysplasia Reactive changes in intestinal metaplasia Alcoholic gastropathy Caustic-induced injury Graft versus host disease Chemotherapy and radiation Ischemia Predominantly Vascular Changes Gastric antral vascular ectasia Portal hypertension (congestive gastropathy) Hemorrhagic gastropathy (“gastritis”) and “Curling’s ulcer” Distinctive (Specific) Types of Gastritis Infections A H. pylori infection Histology of H. pylori–associated gastritis H. pylori diagnosis Noninvasive methods Invasive methods Atrophic gastritis and gastric atrophy Staging gastric atrophy Disorders associated with H. pylori gastritis Gastroduodenal erosions and ulcers (“peptic ulcers”) Pathogenetic factors Epidemiology Atypical clinical presentations Endoscopic appearance of peptic erosions and ulcers “PEPTIC DISEASES” OF THE DUODENAL BULB AND THE PROXIMAL DUODENUM Pathogenesis and Clinical Features of Duodenitis Duodenal ulcer Clinical features Pathology of Duodenitis and Duodenal Erosions and Ulcer Gross pathology Histology Differential diagnosis of duodenitis Healing and healed ulcers Complications of gastroduodenal ulcers Treatment The role of the pathologist and clinical implications Autoimmune Gastritis Pathogenesis Subtypes of autoimmune gastritis (AIG) and their etiology Clinical features Pathology LYMPHOCYTIC GASTRITIS Morphologic Separation of Etiologies GRANULOMATOUS GASTRITIS CARDITIS NON–H. PYLORI BACTERIAL INFECTIONS Non–H. pylori Helicobacter Species (NHPH)/“Helicobacter heilmannii” Gastric disease associated with non–H. pylori Helicobacter species/“Helicobacter heilmannii” Diagnosis Tuberculosis Syphilis Enterococcal Gastritis Phlegmonous and Emphysematous Gastritis VIRAL INFECTIONS Cytomegalovirus Infection (HHV-5) Herpes Viruses (HHV-1,2) Epstein–Barr Virus (EBV—HHV-4) Other HHV Viruses Other Viruses FUNGAL INFECTIONS Candida albicans Histoplasmosis Mucormycosis (Zygomycosis) Aspergillosis PARASITES AND NEMATODES Cryptosporidium Anisakiasis Other Parasites and Nematodes OTHER GASTRITIDES Clinical features Endoscopic features Histologic features Eosinophilic Gastritis Eosinophilic gastritis as part of gastric involvement in eosinophilic gastroenteritis Differential diagnosis Collagenous Gastritis Diffuse collagenous gastroenterocolitis Gastric Malakoplakia Drug- and Chemotherapy-induced Gastritis HYPERTROPHIC GASTROPATHIES AND MÉNÉTRIER’S DISEASE Primary/Idiopathic Ménétrier’s Disease Clinical Presentation Pathology of Primary Ménétrier’s Disease Carcinoma Complicating Ménétrier’s Disease Secondary Ménétrier’s Disease HYPERTROPHIC GASTROPATHYASSOCIATED WITH PROTEIN LOSS Cytomegalovirus-associated Hypertrophic Gastropathy Hypertrophic Lymphocytic Gastritis Helicobacter pylori–associated Hypertrophic Gastritis HIV-associated Hypertrophic Gastritis Large Gastric Folds Associated with Other Conditions Other Types of Large Gastric Folds DISTINCTIVE ENDOSCOPIC ENTITIEs MISCELLANEOUS DISORDERS OF THE STOMACH Gastric Calcinosis Gastric Glandular Siderosis Approach to the Interpretation of Gastric Biopsies Surface epithelium HISTOLOGY 570 Riddell_Chap13.indd 570 2/15/2014 1:45:43 PM Chapter 13 Stomach and Proximal Duodenum: Inflammatory and Miscellaneous Disorders CLASSIFICATION OF GASTRITIS AND GASTROPATHY Though no classification of gastritis satisfies everyone, the overall goal of any classification is to help clear thinking and be clinically useful. Inevitably much of the early thinking regarding gastritis was centered on “peptic ulcer disease” (PUD). Ignorance regarding the role of both Helicobacter and medications gave rise to theories that were to some extent flawed, yet they still dominate traditional teaching. Gastritis was considered physiologic and intestinal metaplasia an aging phenomenon. We also need to recall that 1.Gastritis originally meant “redness”—which now is usually associated with a gastropathy rather than gastritis; conversely, most histologic gastritis has a normal endoscopic appearance. 2.Many disorders that are characterized by abnormal endoscopy also have a typical biopsy appearance. From a classification viewpoint are these best considered from an endoscopic or histologic viewpoint? Most classifications can only be viewed from one vantage point. 3.From a clinical viewpoint, “ulcers” have played a major role in gastric disease because of the symptoms with which they or their complications are associated (pain, bleeding, perforation, and obstruction/ stenosis). However, the term “peptic ulcer disease” has been in common parlance for decades, with the implication that this is associated with acid, the “proof” being that symptoms are markedly ameliorated with therapy, whether antacids, H2-receptor antagonists, or proton pump inhibitors (PPIs). In the early 1980s, it was ultimately shown that some ulcer disease, especially in the duodenum, was related to Helicobacter pylori, so that its eradication virtually guaranteed that duodenal ulcer, the archetypal peptic ulcer, would not recur. Thus PUD changed from being primarily acid related to primarily bacterial, or a combination of both. 4. Nonsteroidal anti-inflammatory drugs (NSAIDs), aspirin (acetylsalicylic acid—ASA), and other medications now play a huge role in gastric pathology. While the introduction of NSAIDs around 1970 was a major step forward therapeutically, it came at a price that included numerous gastrointestinal (GI) side effects. Prior to this time, ASA had been “the” analgesic and antipyretic of choice. Bayer introduced ASA in the market around 1900, and within a decade or two this “wonderdrug” was present in virtually every household in the more developed countries, and used widely for numerous ailments—colds, coughs, headaches, migraines, and all arthritides. Yet the erosive, ulcerative, and bleeding Riddell_Chap13.indd 571 571 diathesis associated with this drug was not widely appreciated. In retrospect, from about 1900 on, many “peptic ulcers” may well have been as much ASA associated as Helicobacter associated, and this association even creeps, almost inadvertently, into case reports back in the 1950s.1 So while we typically think of “peptic ulcer disease” historically as unrecognized Helicobacter infection, ASA was very likely a major contributor. This continued until acetaminophen/paracetamol/Tylenol came into the market in to the 1960s. Further, it is now well recognized that, especially in the very young2,3 and elderly,4 not only that NSAIDs are likely “the” culprit irrespective of the presence of H. pylori, but that the risk of complications such as bleeding (and therefore the erosions and ulcers that bleed) can be largely prevented using PPIs. Thus, historically, the disease we consider to be “peptic ulcer disease” may have been as much NSAID/ASA associated as Helicobacter associated, especially in the presence of abundant acid. 5.Historically, alcohol, which not only has a social role in many societies but is also an analgesic in large doses, has been around much longer than any other gastric damaging agent except for Helicobacter, and produces histologic changes similar to NSAIDs (i.e., a chemical/reactive gastropathy). From around 1900 on when aspirin became available, the big three, became Helicobacter, alcohol, and ASA, and from 1970 on, NSAIDs was added to these. 6.The notion of “peptic ulcer disease” and “no acid— no ulcer” is therefore likely true in that in the major causes of gastroduodenal erosions and ulcers, namely, Helicobacter and NSAIDs/ASA, and other medications or chemicals, especially alcohol, the presence of acid facilitated the development of injury caused by these agents. Although the nature of the interaction of these common causes of peptic ulcer is still unclear, it would make most sense if, when antral-predominant H. pylori is present, that the risk of NSAID/ASA and alcohol-induced damage was increased, but that when the organism spread proximally, resulting in a decrease in acid output, that there may well be a degree of protection from NSAID/ASA, and possibly alcohol-associated damage (Table 13-1). Current Classification of Gastritis Chapter 13 Until the early 1970s, chronic gastritis was classified into three main varieties (superficial, atrophic, and hypertrophic) as suggested by Schindler in 19395 (Table 13-2). Wood as well as Schindler later concluded that chronic hypertrophic gastritis is a variation of normal mucosal function.6,7 Thus, chronic gastritis was classified as superficial or atrophic. Whitehead’s classification was the first to understand the importance of noting location, and grading 2/15/2014 1:45:44 PM 572 Lewin, Weinstein, and Riddell’s Gastrointestinal Pathology and Its Clinical Implications Table 13-1 ABC Classification of Gastritis Autoimmune Bacterial Chemical Drug-associated/ Iatrogenic Eosinophilic Focal Granulomatous Hypertrophic (big folds) Idiopathic Juvenile (pediatric) Lymphocytic Multifocal intestinal metaplasia with/ without atrophic front Pernicious anemia Bugs including post-Rx effects: Helicobacter pylori Enterococcus Syphilis Bile reflux NSAIDs/ASA Anti-platelet medications Chemotherapy/GVHD Iron Alcohol Eosinophilic gastritis/ gastroenteritis Food allergies, medications Crohn’s disease Tuberculosis Sarcoid Crohn’s disease Foreign body Helicobacter pylori “Ménétrier’s disease” Lymphocytic gastritis Eosinophilic gastritis Gastric varices Gastritis cystica profunda Lymphoma (MALT) Gastric adenocarcinoma Helicobacter pylori gastritis (lymphocytic), CMV Zollinger–Ellison syndrome Multiple polyps/polyposis Follicular with H. pylori, CMV Helicobacter pylori, celiac disease Chronic erosive (varioliform) gastritis In atrophic gastritis, isolated Modified from Wyatt JI, Dixon MF. Chronic gastritis—a pathogenetic approach. J Pathol. 1988;154(2):113–124. the depth and degree of inflammation and the presence or absence of both intestinal and pseudopyloric metaplasia, separating them from atrophic changes8 (Table 13-2). This really formed the basis of all subsequent morphologic classifications of gastritis. In 1973, Strickland and Mackay classified gastritis based on detecting parietal cell (PC) antibodies, clarifying the etiology of autoimmune gastritis (AIG) (type A) despite the fact that these can develop in Helicobacter infected patients. It is associated with atrophic changes in body and fundic (oxyntic) mucosa. Antral predominant gastritis was type B. Glass and Pitchumon added type AB into Strickland–Mackay classification to encompass cases that did not fit type A or type B, essentially pangastritis. Riddell_Chap13.indd 572 With the rediscovery of H. pylori (originally Campylobacter pylori) by Warren and Marshall in the early 1980s,9 it became clear that H. pylori is a principal component of most gastritides. In 1988, two classification systems emerged. That by Wyatt and Dixon incorporated reactive gastropathy (then called chemical gastritis/gastropathy) as the “C” of the ABC classification system, A being autoimmune and B being bacterial (=Helicobacter but, at that time, C. pylori).10 The same year, Correa proposed classifying gastritis based on clinical and etiopathogenetic information. He classified chronic gastritis into superficial gastritis, diffuse antral gastritis (DAG), usually Helicobacter associated and related to duodenal ulcer disease, diffuse corporal atrophic gastritis (autoimmune), and multifocal atrophic gastritis (MAG—considered to be “environmental”). MAG was related to intestinal-type adenocarcinoma and gastric ulcer, and intestinal metaplasia in the antrum and body.11 Diffuse corporal atrophic gastritis was often related to AIG and pernicious anemia, with inflammation and atrophy in the corpus and relative sparing of the antrum11,12 (Fig. 13-1). The Sydney system is the basis of most contemporary classifications of gastritis. Proposed by a group of European pathologists and clinicians (World Congress of Gastroenterology, Sydney, August 1990),12 it recommended incorporating the topography of gastric mucosal changes with the immunology and microbiology of the disease. The classification depends on separate assessment of the antrum and corpus by taking a minimum of two biopsies from the anterior and posterior walls of the respective gastric compartments as well as any specific lesions identified. An important feature is a standard three-tier grade of mild, moderate, and severe applicable to a selected number of morphologic variables. As a broad guideline, each successive grade represents an increment in severity of about one-third. Graded variables included inflammation (acute and chronic), atrophy, metaplasia, and density of H. pylori. The Sydney system also expanded previous classifications by adding a variety of other “special forms” of gastritides (collagenous, eosinophilic, granulomatous, lymphocytic, etc.). The Sydney classification was updated in 1994,13 which expanded the section on specific entities (special forms) and includes a 4-point visual analog (equivalent to none, mild, moderate, and severe) to aid with morphologic grading of inflammation and atrophy.13 Gastric atrophy is loss of normal glands, often with replacement by an epithelium that could be either native or metaplastic (Table 13-3). The score is an average from each region’s biopsies. Antral atrophy was the average score for atrophy from all antral biopsies and corpus atrophy (the average score for atrophy from all corpus biopsies).13 The updated Sydney classification depends on the separate assessment of the 2/15/2014 1:45:44 PM Chapter 13 Stomach and Proximal Duodenum: Inflammatory and Miscellaneous Disorders 573 Table 13-2 Gastritis Classification “Historical Prospective” YEAR, AUTHOR CLASSIFICATION 1942, Schindler Gastritis Superficial Atrophic Hypertrophic (later dropped as Schindler and others concluded hypertrophy is normal function variation) Mucosa type Gastritis grade Metaplasia Pyloric Superficial Body Quiescent Pseudopyloric Cardiac Active Transitional Atrophic (used synonymous with deep Intestinal inflammation). Indeterminate Mild (quiescent or active) Moderate (quiescent or active) Severe (quiescent or active) Type A or autoimmune gastric atrophy of pernicious anemia Type B—nonautoimmune (pyloro-cardial extension type in connection with PUD (Kimura, 1972181) Type A (autoimmune) Type B (antrum) Type AB (cases that did not fit Type A or Type B) Morphologic Mechanistic Synonyms Not atrophic Superficial Initial stage of other types? Simple? Diffuse antral (DAG) Hypersecretory? Antral Psychosomatic? Type B Infectious? (C. pylori) Atrophic Postgastrectomy Reflux Chemical Diffuse corporal Autoimmune Type A Multifocal Dietary? Environmental Type B Type AB Pangastritis 1972, Whitehead et al.8 1973, Strickland and Mackay828 1976, Glass and Pitchumoni modification of Strickland and Mackay829 1988, Correa11 GASTRITIS Figure 13-1. Prototypes of gastritis pattern predict disease outcome. In practice, all tend to have some degree of both antral and corpus inflammation. Top left: Duodenal ulcer (DU) patients have antral predominant inflammation with little corpus inflammation. Bottom left: Pangastritis is seen in gastric ulcer (GU) patients. Corpus mucosa is inflamed and often extends into the specialized mucosa but still tends to be antral predominant. Top right: Pangastritis with atrophy is seen in patients with the intestinal type of gastric adenocarcinoma (CA). Bottom right: Corpus-predominant gastritis is usually seen in AIG or end-stage Helicobacter infection. Riddell_Chap13.indd 573 Gastritis (in its broadest sense) and its complications account for millions of doctors’ office visits each year. Symptoms are often associated with acute changes or complications described as mild upper abdominal discomfort, indigestion, heartburn, coated tongue, foul breath, and bad taste to more ominous symptoms such as loss of appetite, nausea, vomiting blood or coffee-ground material, diarrhea, and dark stools. Most patients with chronic gastritis have no symptoms. Even so, these symptoms are not specific and include broad differentials such as H. pylori infection, other infections, bile reflux, inflammatory Chapter 13 antrum and corpus. It needs a minimum of two biopsies from the lesser and greater curvature of the respective gastric compartments as well as the incisura and any specific lesions identified (Fig. 13-2).13 On all occasions accurate grading depends on correctly oriented full-thickness mucosal biopsies. In practice, other than for academic studies, grading is rarely required. 2/15/2014 1:45:45 PM 574 Lewin, Weinstein, and Riddell’s Gastrointestinal Pathology and Its Clinical Implications Table 13-3 Gastritis Classification “Sydney System” 1996, Updated Sydney13 GASTRITIS TYPE ETIOLOGY SYNONYMS Non-atrophic Helicobacter pylori ? Other factors Superficial Diffuse antral, Chronic atrophic Interstitial—follicular Hypersecretory Type B Autoimmunity Type A Diffuse corporal Pernicious-anaemia associated Type B Type AB Environmental Metaplastic Atrophic Autoimmune Multifocal Special forms Chemical Radiation Lymphocytic Noninfectious granulomatous Eosinophilic Other infectious gastritis Helicobacter pylori Dietary ? Environmental Chemical irritation: Bile NSAIDs/Antiplatelet Other medications Radiation injury Idiopathic? Immune mechanism Gluten Drug (ticlopidine) ? H. pylori Crohn’s disease Sarcoidosis Wegener’s granulomatosis and other vasculitides Idiopathic Food sensitivity, drugs, Churg-Straus Bacteria (other than H. pylori) Viruses Fungi Parasites Reactive, Reflux NSAID Type C Varioliform (endoscopic) Celiac disease–associated Isolated granulomatous Allergic Phlegmonous bowel disease (IBD), and side effects of medications (Table 13-4). As treatment depends on the cause, it is important to know the cause for appropriate management. Occasionally, it may be necessary to list possible etiologies for gastric inflammation, rather that reporting “nonspecific chronic inflammation”—which is an unnecessarily complex term as all inflammation is “nonspecific,” so these words can always be omitted from reports without deleterious effect. If it is specific, the cause (e.g., Helicobacter) should be stated. Distinctive (Specific) Types of Gastropathies Figure 13-2. The updated Sydney biopsy protocol requires a minimum of two biopsies from the lesser and greater curvature of the respective gastric compartments as well as the incisura and any specific lesions identified. This identifies all of the patterns of gastritis illustrated in Figure 13-1, as well as estimating the extent of atrophy present, which often starts at the incisura/angulus (IA), affects the antrum (A1, A2), and then extends proximally to the oxyntic zone (B1, B2), so that, as antral inflammation extends proximally, biopsy site B1 is first affected, and B2 is the last site affected. Riddell_Chap13.indd 574 Gastropathies are biopsies in which epithelial (noninflammatory) changes predominate. The mucosa is often mucin depleted, causing it to appear red endoscopically (invariably interpreted by endoscopists as “gastritis” rather than areas of redness). They include biopsies with primary epithelial reactive changes (such as chemical/reflux (bile) gastropathy, chemotherapy effect) and a smaller subset of biopsies with predominant vascular pathology (such as gastric antral 2/15/2014 1:45:45 PM Chapter 13 Stomach and Proximal Duodenum: Inflammatory and Miscellaneous Disorders 575 Table 13-4 Classification by Predominant Histologic Change SUBCATEGORY Gastropathy (predominantly noninflammatory) Predominant epithelial changes Predominant vascular pathology Gastritis (predominant inflammatory) Infectious Noninfectious Endoscopic gastropathies Part of systemic involvement Distinctive macroscopic (endoscopic) appearance with appropriate histology (a) Medications/reflux (bile) gastropathy (b) Alcoholic gastropathy (c) Caustic-induced injury (d) GVHD (e) Radiation/chemotherapy (f) Ischemia (a) GAVE (b) Portal hypertension (c) Hemorrhagic/shock gastropathy 1. Bacterial (a) Helicobacter pylori bacterial infection (autoimmune gastritis, lymphocytic gastritis, granulomatous gastritis, carditis) (b) NHPH infections—“H. heilmanii” Other bacteria—TB, syphilis, phlegmonous and emphysematous gastritis 2. Viral (CMV, Herpes) 3. Fungal (Candida, histoplasma, mucormycosis, Aspergillosis) 4. Parasitic (Cryptosporidium, Anisadikosis, other parasites, and nematodes) 1. IBD (endoscopic, histologic features, clinical implication) 2. Eosinophilic gastroenteritis 1. GVHD 2. Vasculitis (including Churg–Strauss) 1. Erosive and hemorrhagic Varioliform gastritis Watermelon stomach (GAVE) Portal gastropathy Hemorrhagic gastritis/gastropathy 2. Nonerosive Nodular gastritis, children Atrophic front, adults 3. Distinctive hypertrophic gastropathy vascular ectasia [GAVE], portal hypertension gastropathy, Dieulafoy, and hemorrhagic/shock) (Table 13-4). Graft versus host disease (GVHD) is usually normal endoscopically. Reactive (Predominant Epithelial) Changes eactive (chemical/reflux-associated) gastropathy R is a reaction to noninfectious irritants. This can be due to protracted exposure to bile and pancreatic juice (especially postgastric surgery14). The most infamous of irritants are NSAIDs, which include overthe-counter drugs such as aspirin and ibuprofen, and many prescription medicines. Other medications— such as bisphosphonates used for osteopenia, iron pills and irritants in food such as capsaicin in peppers and chilies and alcohol—can all cause this lesion.15 These irritants usually cause no clinical problems when taken for the short term, although endoscopic damage can be seen even with short-term use. However, regular (or e xcessive) use can lead to a more severe gastropathy as well as erosions and ulcers. With the increasing use of aspirin and other NSAIDs, Riddell_Chap13.indd 575 and decreasing prevalence of H elicobacter, chemical/ reactive gastropathy is increasingly seen in gastric biopsies, and may co-exist. Anti-platelet mediations also cause similar injury. Pathogenesis: Aspirin is the best-studied NSAID, the mechanism of injury is inhibition of prostaglandin synthesis by inhibiting cyclooxygenase (COX) 1 and 2.16 Aspirin also changes the ability of the mucosa to maintain a pH gradient causing gastric acid back-diffusion with resultant mucosal injury.16 Further, its anticoagulant properties increase the risk of bleeding once erosions or ulcers are present. Conversely, some other NSAIDs have antiplatelet properties but do not possess this therapeutic anticoagulant effect. NSAIDs produce mucosal injury by both local and systemic effects.16 Newer NSAIDs are predominantly COX-2 inhibitors, which make them less likely to cause gastric injury and the risk of gastric (or duodenal) injury is reduced, but not abolished. A variety of antiplatelet medications are increasingly being implicated causing similar injury. Histology: The histology of reactive gastropathies has both an acute and a chronic phase, although Chapter 13 CATEGORY 2/15/2014 1:45:45 PM