Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Myocardial infarction wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Pericardial heart valves wikipedia , lookup
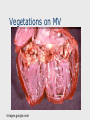
Echocardiography wikipedia , lookup
Jatene procedure wikipedia , lookup
Aortic stenosis wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Rheumatic fever wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Infective Endocarditis J.B. Handler, M.D. Physician Assistant Program University of New England 1 Abbreviations ABE- acute bacterial endocarditis SBE- subacute bacterial endocarditis IE- infectious endocarditis ASD- atrial septal defect VSD- ventricular septal defect PDA- patent ductus arteriosus AoV- aortic valve MVP- mitral valve prolapse TEE- transesophageal echocardiography TTE- transthoracic echocardiography PCN- penicillin HCM- hypertrophic cardiomyopathy AR- aortic regurgitation MR- mitral regurgitation TR- tricuspid regurgitation RV- right ventricle CABG- coronary artery bypass graft surgery 2 Key Terms Infective Endocarditis: Infection on a cardiac valve or an endocardial surface within the heart. Most cases are due to bacterial infection; fungal infections much less common. 3 Pathogenesis In >50% of cases, underlying valve abnormality (acquired or congenital) provides source of turbulent blood flow/jet effectstransient bacteremia (from procedure or surgery) colonizationinfection. Normal valve endocarditisbacteremia with virulent organism (like S aureas) infection. Example: IV drug abuser. 4 Common Underlying Lesions Rheumatic valve disease; bicuspid AoV; aortic stenosis/sclerosis/regurgitation; mitral stenosis/regurgitation/prolapse; hypertrophic CM. Most forms of congenital heart disease except ASD. 5 Common Underlying Lesions Many surgically corrected congenital cardiac lesions except ASD, VSD and PDA. CABG surgery and permanent pacemakers do not predispose to endocarditis. Prosthetic heart valves. 6 Bacteremia Portals of entry: skin, upper respiratory tract, oral cavity, GI (lower)/GU tracts. Commonly from procedures or surgery. Some dental work/cleaning/flossing & related procedures; procedures and surgeries involving upper respiratory, lower GI & GU tracts. Frequent exposure to random bacteremia from frequent brushing/flossing. Presence of indwelling catheters, esp. central lines. 7 Organisms S viridans, group D strep, Enterococcus faecalis, S aureas (most common organism). HACEK organisms: Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella Prosthetic valve endocarditis: Early (1st 2 mos): S aureas, S epidermitis, gram negative organisms and fungi Late: Streptococci & Staph (coag+ and -) 8 Involvement of Cardiac Valves Mitral and Aortic most commonly involved. Classic valve lesion is a vegetation: mass of platelets, fibrin, colonies of bacteria + few inflammatory cells; visible on 2D echocardiography TEE>TTE. RV endocarditis: Tricuspid ( 85% of cases) > pulmonic valve (15%) involved only in setting of IV drug abuse; organism usually S aureas. 9 Endocarditis Images.google.com Vegetations on MV Images.google.com Vegetation: 2- D Echo Images.google.com Clinical Findings Febrile illness often with with nonspecific symptoms at onset. Fever usually elevated, often 38 degrees C, night sweats, arthralgias, myalgias, weight loss. Duration days to weeks. Infectious emboli to brain, kidneys, joints, skin, lungs, mensenteric circulation & bowels: stroke, flank pain, arthritis, cough/dyspnea, abscesses, organ infarction, abd pain. New or changing regurgitant heart murmurs may be present. 13 Clinical Findings Peripheral lesions from micro emboli: Petechiae (palate, conjunctiva) Subungal (“splinter”) hemorrhages Immunologic lesions: Osler’s nodes: painful, raised lesions of fingers/toes Janeway lesions: painless lesions of palms or soles Roth spots: exudative lesions in the retina 14 Immunologic Lesions Osler’s Nodes Images.google.com Janeway Lesions Immunologic Lesions Roth Spots Images.google.com Varying Presentations Staph aureas and other more virulent organisms: acute course with rapidly progressive, destructive infection (ABE); acute febrile illness, early embolization, valvular destruction and insufficiency. Viridans streptococci, enterococcus: sub-acute course (weeks); systemic and peripheral manifestations predominate; valvular destruction gradual. 17 Diagnostic Studies Blood cultures: essential to the diagnosis and treatment; must draw 3 sets, 1 hr apart; before considering empiric antibiotics. Echocardiography: TEE 90% sensitive in localizing involved valve. TTE- 60% s. Pathognomonic finding is a vegetation. Leukocytosis, anemia or hematuria depending on infecting organism, embolization and immune response. 18 Dx of Endocarditis: Modified Duke Criteria Major: 2+ BC’s with typical organism Abnormal echo for vegetation or similar New regurgitant murmur Minor: Predisposing condition: valve abn; IV drug use Fever 38 degrees Vascular phenomenon: systemic emboli, infarction; cutaneous hemorrhage Immunologic lesion + BC not meeting above criterion 19 Dx of Endocarditis: Modified Duke Criteria Definite Dx: 2 major criteria 1 major +3 minor criteria 5 minor criteria Possible Dx: 1 major +1 minor criteria 3 minor criteria 20 Permanent Damage Heart: AR, MR, TR, often severe due to destruction of valves. Heart failure often a result of left sided valvular regurgitation (AR,MR). Emboli to brainstrokes Emboli elsewhere: kidneys, lungs, joints, bowels, other. 21 Prevention Procedures likely to cause transient bacteremia can lead to endocarditis; prophylactic Rx with antibiotics beforehand can be protectivelimited applications (below). Procedures: see slide #7 above Significant change in recommendations made in 2007. In past most forms of valve disease warranted Abx prophylaxis before procedure; now very limited. 22 Current Indications for Antibiotic Prophylaxis Prosthetic heart valve Prior episode of endocarditis Unrepaired or incompletely repaired complex cyanotic congenital heart disease Completely repaired cong ht disease with prosthetic material: for 1st 6 mos. post repair Repaired cong heart defect with residual defect at the site of prosthetic patch/device. Cardiac transplant patient with valvular disease Ref: http://www.ada.org/prof/resources/topics/infective_endocarditis_guidelines.pdf 23 Antibiotic Prophylaxis Other valvular lesions, whether congenital or acquired, do not require endocarditis prophylaxis before bacteremia associated procedures. Risk of getting endocarditis out-weighed by risk of side effect or reaction to the antibiotic. 24 Antibiotic Prophylaxis Antibiotic prophylaxis (dental work): oral amoxicillin 2 grams 30 to 60” before procedure. Alternatives: cephalexin, clindamycin, azithromycin or clarithromycin. See current: chap 33 table 33-5. 25 Treatment of Endocarditis Should be based on organism identified by blood cultures. Example- S viridans: Penicillin G 2-3 million units every 4 hours x 4 wks. If add gentamycin 1mg/kg IV q8 hrs to PCN, course is shortened to 2 wks. Empiric Rx if needed while awaiting BC results: Vancomycin + Ceftriaxone, both IV. 26