Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Periodontal disease wikipedia , lookup
Kawasaki disease wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Behçet's disease wikipedia , lookup
Infection control wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Neuromyelitis optica wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
Pathophysiology of multiple sclerosis wikipedia , lookup
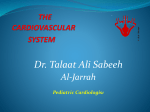
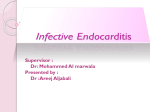
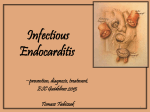
Infective Endocarditis Senior Oral Medicine Chapter 2 August 27, 2009 Susan Settle, D.D.S. Infective Endocarditis • A microbial infection of the endothelial surface of the heart or valves • Usually is near congenital or acquired cardiac defects • Designated by the causative organism • Also classified as NVE or PVE Etiology • Usually Bacterial – Staphylococcus aureus Endocarditis – Streptococcus viridans Endocarditis – Actinobacillus actinomycetemcomitans Endocarditis • Sometimes Fungal – Candida albicans Endocarditis Etiology • Streptococci most common cause (35-60%) – Mostly viridans group • Staphylococci about 30-40 and gaining – S. aureus most common cause in IVDU’s – Incidence increasing in hospital-acquired infections Epidemiology • Incidence <1% Of General Population Epidemiology • Population Groups At Greater Risk: – Rheumatic Fever History – Hemodialysis – Previous History Of Endocarditis – Patients With Prosthetic Valves – IV Drug Users (30% Risk Within 2 Years) Predisposing Conditions • • • • • • Mitral valve prolapse Aortic valve disease Congenital heart disease Prosthetic valve Intravenous drug use No identifiable cause in 25-47% Epidemiology • • • • More Common In Men Median Age 50 Years Acute Cases Increasing Streptococcal Cases Slightly; Fungal And Gram Negative Cases Increasing Epidemiology • Incidence Increases With Age, Probably Due To Increased Cardiac Disease And Decreased Immunity • Prosthetic Heart Valve Infections Are Increasing Dentistry And Endocarditis • Streptococcus viridans: Usual Etiologic Agent • Usually Is Not Acute (Subacute) – (That Is Why It Is Referred To As “SBE”) • Incubation Period Approximately Two Weeks Epidemiology • Mitral Valve Prolapse: Only 1/4 Of MVP Patients Have Mitral Insufficiency (Regurgitation Or Murmur) - This Results In The Very Slight Increased Risk For Endocarditis MVP • Mitral valve prolapse accounts for 25-30% of adult cases of native valve endocarditis • MVP is now the most common underlying condition among patients who develop infective endocarditis Aortic Valve Disease Accounts for 1230% of IE cases Epidemiology • Fenfluramine (Pondimin) And Dexfenfluramine (Redux) Were Reported To Cause Cardiac Valvular Damage When Used For 4 Or More Months • Premedication No Longer Indicated Epidemiology • Vena Cava Filters Or Umbrella Stents Placed To Catch Blood Clots Have Not Demonstrated Increased Risks 3 Types Of Endocarditis Lesions • Cardiac Lesions • Embolic Lesions: Friable Cardiac Lesions That Break Away • General Lesions Cardiac Lesions • • • • Usually Valvular Most Often Mitral Valve May Cover The Entire Valve Mass Of Platelets, Fibrin And Bacteria • Sterile Vegetations May Occur In 50% Of Lupus Patients Sites of Endocarditis Involvement Embolic Lesions • Osler’s Nodes: Are Small, Painful Petechiae In Extremities Janeway Lesions • Pathognomonic of IE • Non-tender dermal abscesses Splinter Hemorrhages Late-appearing symptom in endocarditis These represent damage to capillaries May also appear due to nail trauma General Lesions • • • • • • • • Enlarged Spleen Arthritis Clubbing Of Fingers Cardiac Failure Conduction Abnormalities Stroke Psychiatric Disease Renal Failure Mortality • Overall Rate About 40% • Death Usually Due To Heart Failure Resulting From Valve Dysfunction • Highest Death Rate Is In Early Prosthetic Valve Endocarditis Classic Triad - But May Not Always Be Present 1. Fever 2. Positive Blood Culture 3. Heart Murmur • Sometimes Insidious Onset • “Flu-Like” Symptoms Lab Findings • • • • +Culture In 95% Of BE Strep viridans Most Commonly Causes SBE Staph aureus Most Commonly Causes ABE Electrocardiography: Will Determine If Infection Progresses To Myocardium Lab Findings • Echocardiography - As Important As A Positive Blood Culture Are Results Which Show Vegetations, Abscesses, Etc. Major Diagnostic Criteria • Positive Blood Culture • Echocardiogram Findings Of Endocardial Involvement • New Valvular Regurgitation Minor Diagnostic Criteria • • • • • • • Predisposing Heart Conditions IV Drug Use Vascular Emboli Osler Nodes Aneurysm Roth Spots Of The Eye Splinter Hemorrhages Treatment • Treat It Early! • Culture • Use Bactericidal Agents –PCN G; Cefatriaxone; PCN G + Gentamicin; Nafcillin; Vancomycin Treatment • Use Adequate Dosage • Parenteral Route • Sufficient Duration: 4-6 Weeks Or Longer Dental Management • Prevention In Susceptible Patients: An Academic Issue • Very Few Cases Related In Time To Dental/Medical Procedures – Incidence Has Been Estimated To Be 100-200 Patients Susceptible To BE In A Dental Practice With 2,000 Patients Antibiotic Prophylaxis • Regimen Designed For Alphahemolytic Strep (S. viridans) • No Clinical Trials Available To Show This Works! (Actually Prevents BE In Humans) • 25-50% Hospital Antibiotic Usage Is For Prophylaxis Antibiotic Prophylaxis • Complications: Resistant Bacteria, Toxicity, Allergies, Suprainfections, Costs • Will Not Prevent All Cases Antibiotic Prophylaxis • Allergy Morbidity Is Higher Than Endocarditis (Allergy To Premed) – 400-800 PCN Deaths Per Year • Effective For Patients With Prosthetic Valves And Previous Endocarditis History American Heart Association Guidelines • Not Intended To Be A Standard Of Care • Not A Substitute For Clinical Judgment • Must Be Considered If You Receive A Medical Opinion That Conflicts With The Guidelines (You Are Responsible For The Outcome Of Your Patient’s Dental Treatment) American Heart Association Guidelines • First Recommendations Were In 1955 • Can Still Develop Endocarditis Even When Using Guidelines Prophylaxis Myths • Most Cases Of BE Of Oral Origin Are Caused By Dental Procedures • AHA Regimens Give Almost Total Protection Against Endocarditis After Dental Procedures Prophylaxis Myths • If A Patient Is Taking Antibiotics For An Infection Before The Dental Procedure, You Do Not Need To Change The Patient To Another Antibiotic Before The Dental Procedure Prophylaxis Myths • The Risk Of Endocarditis Is Greater Than The Risk Of Toxic Effects Of The Antibiotic 2007 AHA Recommendations Prophylaxis Indicated For The Following Groups Of Patients: • Those with a previous history of endocarditis • Those with prosthetic cardiac valves • Post-heart transplant patients with valvulopathy • Those with certain congenital types of heart disease Congenital Heart Disease Indications for Prophylaxis • Unrepaired cyanotic CHD, including those patients with palliative shunts & conduits • Completely repaired CHD with prosthetic material or device placed by surgery or catheter during the first 6 months after the procedure • Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device, which inhibits endothelialization Dental Procedures For Which Prophylaxis Is Recommended • All procedures involving manipulation of gingival tissue or the periapical region of teeth or perforation of oral mucosa • Excluded procedures: – Routine anesthetic injections through noninfected tissue – Radiographs – Placement of removable prosthodontic or orthodontic appliances – Adjustment of orthodontic appliances – Shedding of primary teeth and bleeding from trauma to lips or oral mucosa Nonvalvular Cardiovascular Devices • Such as coronary artery stents, hemodialysis grafts • Routine antibiotic prophylaxis for dental procedures is not recommended • However, prophylaxis is recommended if an abscess is going to be incised & drained, • Or, if there is leakage present after the device is placed Not In This Presentation! • • • • Know Antibiotics in AHA Regimen Know Dosages of These Antibiotics Know The Regimen Remember To Wait 9-14 Days Between Premed Appointments To Avoid Antibiotic Resistance Development • If Patient Is On A “Regimen” Antibiotic Switch To Another Drug In The Regimen