Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
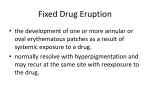
Go Back to the Top Chapter To Order, Visit the Purchasing Page for Details Drug-Induced Skin Reactions and GVHD 10 Skin and mucocutaneous lesions induced by a drug or by its metabolites are called drug eruptions. Some cutaneous drug reactions present a specific morphological pattern. However, most drug eruptions can present the appearance of any cutaneous lesion. It is necessary for dermatologists to take a detailed patient’s history of medication use as well as a medical history. It is clinically important to differentiate drug-induced skin reactions from viral rash and graft-versus-host disease (GVHD); this differentiation is sometimes difficult. A. Drug-induced skin reactions 10 Outline ● Drug-induced skin reaction or drug eruption is a general term for eruptions in the skin and mucosa induced by a drug or its metabolites. ● Drug-induced skin reactions show various morphologies. Clinical images are available in hardcopy only. a b c d e f g General information Maculopapular or morbilliform eruptions may be the most common of all cutaneous drug reactions. It is also known that cutaneous drug reactions present the specific morphological patterns. (Figs. 10.1-1 and 10.1-2). In diagnosing skin diseases, it is essential to consider drugs as a possible cause of any eruption, because drug eruptions can take the form of any skin lesion. Drug eruptions may be accompanied by general symptoms including fatigue, porgansq j h i k l disfunction m nof the internal o fever, lymph node enlargement, such as liver, kidneys or bone marrow, hypotension and shock. Classification, Pathogenesis Drug eruptions are roughly divided into immunologic and nonimmunologic. The pathogenesis is unclear in some cases. The eruptions are often classified by their clinical features (Table 10.1, Figs. 10.2-1 and 10.2-2). Clinical images are available in hardcopy only. Treatment It is essential to discontinue the causative medication. In serious cases, such as anaphylactic shock, systemic management using steroids in large doses including antihistamines, epinephrines, and steroids in large doses, including by pulse therapy. a b c d e f g h Fig. 10.1-1 Drug-induced skin reaction. a: Diffuse edematous erythema on the back. Each eruption is an erythema multiforme-like erythema of 1 cm to 2 cm in diameter that gradually enlarged and tended to coalesce. b: Edematous itchy erythema coalesced into a large plaque. i a. p by q j Classification ofmdrugn eruptions k l o pathogenesis (Table 10.2) r 1. Immunologic drug reactions A drug or the complex of a drug and a serum protein becomes 126 r 127 A. Drug-induced skin reactions Table 10.1 Drug-induced skin reactions and their typical causative drugs. Type of eruption in druginduced reactions Causative drugs Maculopapular Iohexol, iomeprol, ampicillin, amoxicillin, carbamazepine, mexiletine, tiopronin Photosensitive Sparfloxacin, fleroxacin, lomefloxacin , piroxicam, ampiroxicam, griseofulvin, mequitazine, ketoprofen Fixed-drug eruption Allylisopropylacetyl urea, mefenamic acid, ethenzamide, barbital, minocycline, sulfamethoxazole, piroxicam, fluorouracil Erythema multiforme Iohexol, carbamazepine, amoxicillin, tiopronin, phenytoin, diltiazem, mexiletine Lichenoid Tiopronin, captopril, interferon a, cyanamide, oxatomide Urticarial Cefaclor, minocycline, iohexol, aspirin, cetraxate, mefenamic acid Toxic epidermal necrolysis (TEN) Cefzonam, penicillin, phenobarbital, chlormezanone, carbamazepine, methazolamide, acetaminophen, allopurinol, diclofenac Stevens-Johnson syndrome Penicillin, chlorpromazine, sulfamethoxazole, sodium aurothiomalate, phenytoin Erythrodermic Carbamazepine, sodium aurothiomalate, cyanamide, allopurinol, ampicillin Vesiculo-bullous D-penicillamine, tiopronin, captopril, bucillamine, alacepril Eczematous Penicillin, chlorpromazine, chlorthiazide, promethazine Purpuric Sodium aurothiomalate, sulfamethoxazole, penicillin, aspirin antigenic, causing a drug eruption that results from immunological processes. That is, a drug eruption occurs in specific individuals whose antibodies and lymphocytes react against specific antigens. Although type I, II, III, and IV hypersensitivities are thought to cause drug eruptions (Coombs and Gell classification), the details of the pathogeneses are unknown. IgE mediated type I allergy: Within 2 hours after exposure to an antigen (e.g., penicillin or some NSAIDs), urticaria or anaphylactic shock occurs. Type II allergy: Complements are activated by an antigenic drug that connects with tissues, resulting in hemolytic anemia and thrombocytopenia. It is observed in some cases of purpura-like eruptions. Immune complex-associated type III allergy: Immune complex deposits in tissues, causing disorders. Vasculitic eruptions are thought to be caused by this mechanism. Type IV allergy: A delayed hypersensitivity reaction is induced by T cells that have been sensitized to drug antigens. It isa knownb that many types of drug eruptions, such eczema-like eruptions, are produced by type IV allergy or by T-cell mechanisms that resemble type IV allergy. Clinical images are available in hardcopy only. c d e f g h i j i j k Clinical images are available in hardcopy only. 2. Non-immunologic drug-induced skin reactions Drug-induced skin reactions without an immunologic pathogenesis may affect anyone, regardless of whetherathere has b beenc sensitization.The pathogenesis of drug-induced skin reactions can also be classified pharmacokinetically. Pharmacologic effects: Drug-induced skin reactions may be produced by essential pharmacological action of the drug. Hair loss 10 d e f g h Fig. 10.1-2 Drug-induced skin reaction. c: Drug-induced erythema enlarged and coalesced to form erythroderma. d: Drug eruption caused by tegafur. 128 10 Drug-Induced Skin Reactions and GVHD Table 10.2 Drug-induced skin reactions classified by mechanism. Immunologic Type I hypersensitivity (via IgE antibodies; acute onset within 2 hours after drug intake) Type II hypersensitivity (eruption caused by thrombocytopenia and hemolysis resulting from complement activation) Type III hypersensitivity (immunocomplex deposition in skin components) Type IV hypersensitivity (reactions caused by activated T cells) Clinical images are available in hardcopy only. Non-immunologic Pharmacological effects Accumulation Drug interaction Patient-specific conditions a b c d e f g 10 Clinical images are available in hardcopy only. a b c d e f g h h i j k l m n o p q caused by anticancer agents and exfoliation in palms and soles caused by retinoids are examples. Accumulation: A drug accumulates in the skin or mucous membranes from prolonged use (arsenic melanoderma and argyria are examples of accumulation disorders). Drug interaction: One drug may inhibit another drug’s metabolism or excretion, or it may influence protein binding, leading to the same symptoms as those in drug overdose. Specific condition of patients: Inherited enzyme deficiency may p j i k l m reaction n o cause drug reactions; excessive occurs against a qminuter amount of drug (intolerance). An unexpected action of the drug is caused (idiosyncrasy). b. Classification of drug eruptions by characteristic skin features Although maculopapular eruption (multiple edematous erythema on the extremities and trunk) are the most common; drug-induced skin reactions can appear as any kind of cutaneous lesion (Table 10.1). When seeing patients with any types of eruption, dermatologists should always carefully consider the possibility of precedent drug reactions. Clinical images are available in hardcopy only. c. Methods of identifying the causative drug b c d e f g h i Fig. 10.2-1 Various types of drug-induced skin reaction. a, b: Erythema multiforme-like. Although uniformly colored erythematous plaques are mainly seen, newly formed erythema is seen at the periphery, some parts of which show the targetlike appearance that characterizes erythema multiforme. c: Purpuric. Dark red macules up to 1 cm in diameter are observed. These do not disappear by diascopy pressure, which indicates that the eruption is purpura. History is taken on drug-induced skin reactions and on exacerp j k remission l n influenced o r bation or ofmeruptions by useqor discontinuation of a drug. If the eruption is suspected to be drug-induced reactions, tests listed below are conducted for identification (Chapter 5). ①Skin test (scratch test, prick test, intradermal test) ②Patch test ③Drug lymphocyte stimulation test (DLST) ④Rechallenge test (absolutely contrainidicated in severe forms of drug reactions) r 129 A. Drug-induced skin reactions d. Specific types of drug-induced skin reactions 1. Fixed drug eruption (FDE) Definition Fixed drug eruptions (FDEs) are eruptions that recur at the same site each time the same drug is administered. They frequently occur at mucocutaneous junctions. Clinical features FDEs frequently occur at mucocutaneous junctions, such as in the perioral area, lips and genitalia, and in the extremities. They are characterized by a single or a few sharply demarcated red or purple patches (Fig. 10.3), with a diameter of 1 cm to 10 cm. Multiple patches may also occur. They may appear as blistering or erosion. Itching and pain are common. The lesions appear seva b of thec eral minutes to several hours after the administration causative drug. They heal in 2 to 5 weeks, leaving pigmentation. If the same drug was administered repeatedly, the dark brown pigmentation intensifies from inflammation in the basal layer, and subsequent melanin deposition in the dermis (post-imflammatory pigmentation). Clinical images are available in hardcopy only. 10 d Pathogenesis FDEs are caused by the activation of cytotoxic T lymphocytes in the basal layer by drugs. Common causative drugs are NSAIDs, tetracyclines, sulfa drugs, phenacetin, hypnogenics and food additives. e f g h i j k k l Clinical images are available in hardcopy only. Diagnosis FDEs are diagnosed by detailed history-taking on drugs and the course of the eruptions. A patch test performed on the site where an eruption has occurred is positive with high frequency; it is diagnostically meaningful. Treatment a The causative drug should be discontinued. b c d 2. Adverse drug reactions in skin that can result in death There are several specific clinical types of drug-induced skin reactions that may lead to death. Toxic epidermal necrolysis (TEN) has the highest mortality (30-35%); Stevens-Johnson syndrome and transitional forms correspond to the same syndrome, but with less extensive skin detachment and a lower mortality (515%). Hypersensitivity syndrome, sometimes called drug-induced e f g h i j Fig. 10.2-2 Various types of drug eruption. d, e: Urticarial drug eruptions. Edematous erythema resembling urticaria is seen on the trunk and palms. Generalized bullous fixed drug eruption MEMO Blistering may be present in some fixed drug eruptions, and it may spread on the whole body surface, becoming severe. Generalized bullous fixed drug eruption may be categorized with toxic epidermal necrolysis (TEN), which is described in the following section. 130 10 Drug-Induced Skin Reactions and GVHD Clinical images are available in hardcopy only. a b c d Clinical images are available in hardcopy only. a e b f c g d h e i f j g k h l i m j n k o l p m q n r Clinical images are available in hardcopy only. 10 b Clinical images are available in hardcopy only. c d ae bf cg Clinical images are available in hardcopy only. dh ei af j gk b h cl dim ejn kfo glp m hq ni r oj Fig. 10.3 Fixed drug eruption (FDE). a: Early FDE on the right eyelid. Early lesions are edematous erythema without pigmentation. b: FDE on the abdomen. Repeated intake of the causative drug results in a severely pigmented FDE lesion. c, d: FDE on the thigh. The center of the lesion shows characteristic pigmentation caused by chronic inflammation. The periphery is erythematous, which suggests recent intake of the causative drug. e: FDE on the interdigital area. Erythema and bullous lesions are seen. hypersensitivity syndrome (DIHS) or drug reaction with eosinophilia and systemic symptoms (DRESS), has a mortality of about 10% or less. Clinical images are available in hardcopy only. 1) Toxic epidermal necrolysis (TEN) Synonym: Lyell’s syndrome Clinical images are available in hardcopy only. Fig. 10.4-1 Toxic epidermal necrolysis (TEN). Clinical features, Classification Toxic epidermal necrolysis (TEN) is one of the severest drug eruptions. It is accompanied by fever, and erythema and blistering on the whole body surface. It leads to marked epidermal necrosis and exfoliation (Figs. 10.4-1 and 10.4-2). It is closely related to Stevens-Johnson syndrome (SJS) (Fig. 10.5). TEN is classified into several types according to the clinical course. TEN developing from SJS: Most cases of TEN develop from SJS. Vaguely outlined, small, dark red edematous erythema sparsely appear on the whole body and gradually spread. They subsequently increase and form blisters and erosion. Typical primary lesions are characterized by so-called target lesions with dusky centers. Severe erosion develops in the oral mucosa, and systemic symptoms such as fever and fatigue are seen. SJS is characterized by the transformation of erythema into blistering p k o 131 A. Drug-induced skin reactions fixed drug eruption (FDE) generalized FDE TEN SJS EM Clinical images are available in hardcopy only. Fig. 10.5 The pathogenic association of fixed drug eruption (FDE), toxic epidermal necrolysis (TEN), Stevens-Johnson syndrome (SJS) and erythema multiforme (EM). and erosion with dark red patches at the periphery (Chapter 9). Rapid extensive type: This is the type that Lyell first reported. Two to 3 days after intake of the causative drug, erythroderma and extensive erosions occur on the whole body surface without preceding macules, and the skin exfoliates easily; it is similar to a large burn (second-degree). This type accounts for several percent of all TEN cases (Fig. 10.6). Fig. 10.4-2 Toxic epidermal necrolysis (TEN). 10 Pathogenesis It is widely accepted that the cellular functions of cytotoxic T cells are abnormally enhanced by certain drugs, including sulfa drugs, penicillin, barbituric acids, aspirins, pyrazolone drugs, and anticonvulsants, and epidermal necrosis and subepidermal separation occurs as a result. Fas-Fas ligands, which induce apoptosis in epidermal cells, are thought be involved in the occurrence of TEN. Treatment Use of the causative drug should be discontinued immediately. Systemic glucocorticosteroids in high doses, including pulse therapy, are widely known to be useful in the early stages of TEN, but not in the late stage of the disease course. Intensive care with topical treatment and body fluid management similar to the patients with burns are essential. Plasma exchange may be conducted, and large doses of immunoglobulins may also be applied. The causative drug must not be readministered. Clinical images are available in hardcopy only. a 2) Drug-induced hypersensitivity syndrome b c d e f g h h i Clinical images are available in hardcopy only. Synonyms: Drug hypersensitivity syndrome, Drug reaction with eosinophilia and systemic symptoms (DRESS) There is still controversy on the naming of this newly proposed concept of the disease condition, but each different disease namea may indicate the same or similar condition which is induced by drug. Drug-induced hypersensitivity syndrome (DIHS) is proposed by a group of Japanese dermatologists which holds that skin lesions are caused by a combination of drug allergy and reactivated latent viral infection, specifically human herpes virus 6 (HHV 6) infection. Two to 6 weeks after administration of a specific drug, fever b c d e f g Fig. 10.6 Diffuse erythematous toxic epidermal necrolysis (Lyell's syndrome). a: The causative drugs here are antituberculosis drugs, which were used for tuberculosis associated with AIDS. Generalized shedding of the epidermis on the whole body is seen. The dermis is pink where the skin exfoliates. b: Severe erosions and ulcers in the oral region. 132 10 Drug-Induced Skin Reactions and GVHD Table 10.3 Diagnostic criteria for drug-induced hypersensitivity syndrome (DIHS). Clinical images are available in hardcopy only. 1. Maculopapular rash develops more than 3 weeks after starting a certain drugs. 2. Lymphadenopathy 3. Fever (>38˚C) 4. Leukocytosis (>10 × 109/L) a. Atypical lymphocytosis b. Eosinophilia 5. Hepatitis (ALT >100 U/L) 6. HHV-6 reactivation The diagnosis is confirmed by the presence of five of the six criteria above. (Shiohara T, Inaoka M, Kano Y. Drug-induced hypersensitivity syndrome (DIHS): a reaction induced by a complex interplay among herpes viruses and antiviral and antidrug immune responses. Allergology International 2006; 55: 1-8). 10 Clinical images are available in hardcopy only. Fig. 10.7 Drug-induced hypersensitivity syndrome (DIHS). and generalized maculopapular erythema occurs (Fig. 10.7), which results in erythroderma in some cases. Enlargement of superficial lymph nodes, liver dysfunction and hematological abnormalities (leukocytosis, appearance of atypical lymphocytes, increase of eosinophils) occur. There is also a report that suggests the involvement of cytomegalovirus and human herpes virus (HHV7) in DIHS. The diagnostic criteria are listed in Table 10.3 (also refer to Chapter 23 for viral infections). Drug reaction with eosinophilia and systemic symptoms (DRESS) is thought to be the same or similar syndrome, which is mainly used by European dermatologists group. The important point is that dermatologists should be aware of these systemic drug-induced reactions in association with marked eruption, and that routine laboratory examination is necessary when a drug eruption is suspected. The treatements include systemic corticosteroid and termination of the causative drug. B. GVHD and viral eruptions 1. Graft-versus-host disease (GVHD) Outline ● After bone marrow transplantation, other organ transplantation or transfusion, donor lymphocytes are stimulated by major and/or minor histocompatibility locus antigens and subsequently target host tissues for cytotoxic damage. ● The skin, intestinal tract and liver are the main affected organs. ● In acute GVHD, erythematous macules occurs on the palms and spread over the whole body. In chronic GVHD, lichen-planus-like and scleroderma-like eruptions are found. 133 B. GVHD and viral eruptions Definition, Pathogenesis When donor-derived blood cells circulate in the patient’s skin after transplantation, the immunocompetent donor, T cells, may recognize the foreign hosts histocompatibility locus antigens (HLA). Subsequently, an immune reaction against the host’s organs occurs. It may also be caused by general blood transfusions. Classification As shown in Table 10.4, graft-versus-host disease (GVHD) is categorized by the onset. The skin, digestive tract and liver are the main organs affected, and the symptoms are mainly seen in those organs. Post-transfusion GVHD occurs about 10 days after a transfusion and has a poor prognosis. Congenital GVHD occurs after birth, and intractable dermatitis, diarrhea, opportunistic infections, and disturbance in growth are caused by lymphocytes transferred from the mother. Clinical features Acute GVHD: In most cases, 10 to 30 days after a graft, edematous erythema appears on the extremities and trunk. It may be accompanied by slight itching. In severe cases, the eruptions coalesce and may develop into erythroderma, blistering or erosion (Figs. 10.8-1 and 10.8-2). Symptoms of acute GVHD may remain longer even after the first 100 days or more after transplantation, as a result of recent improvements in immunosuppressive drugs. Chronic GVHD: This includes lichenoid forms and sclerodermoid forms. The lichenoid forms multiple purplish-red plaques resembling lichen planus, and the sclerodermoid forms sclerotic lesions resembling scleroderma. The severity of GVHD is classified according to the severity of the skin lesions and other organ disorders (Table 10.5). a Clinical images are available in hardcopy only. a b c d e f g h 10 Clinical images are available in hardcopy only. b c d e f g h i i j Pathology GVHD pathologically presents a lichenoid reaction. Intradermal lymphocyte infiltration, necrosis of the epidermal cells, and Table 10.4 Classification of graft-versus-host disease (GVHD). Type of GVHD Duration after transplantation/ transfusion Symptoms Fever, diarrhea, erythrodermic skin eruption, pulmonary edema, heart failure Hyperacute 7 to 14 days Acute a b Up to 100 days Triad (fever, diarrhea and liver dysfunction). Poorly demarcated erythema seen on the face and palmoplantar area. In severe cases, TEN and erythroderma. Chronic More than 100 Various skin lesions like those in collagen diseases and lichen planus. Liver dysfuncdays tion, oral symptoms, ocular symptoms. Transfusion- About 10 days associated Clinical images are available in hardcopy only. Resemble those of hyperacute GVHD. Prognosis is poor. c d e f g h Fig. 10.8-1 Acute graft-versus-host disease (GVHD). a: Diffuse erythema on the back after bone marrow transplantation. Differential diagnosis from drug eruption is almost impossible clinically. b, c: Severe acute GVHD. Severe exfoliation similar to toxic epidermal necrolysis is seen. 134 10 Drug-Induced Skin Reactions and GVHD Table 10.5 Clinical staging and grading of GVHD. Clinical images are available in hardcopy only. c d e f g h i j k Gut findings 1 Maculopapular rash on <25% of body surface 2 to 3 Diarrhea 500 to 1000 mL/d or persistent nausea 2 Maculopapular rash on 25% to 50% of body surface 3 to 6 Diarrhea 1000 to 1500 mL/d 3 Generalized erythroderma 6 to 15 Diarrhea >1500 mL/d 4 Desquamation and bullae >15 Overall Grade 10 Liver findings (mg/dL bilirubin) Skin findings Stage Severe abdominal pain or ileus Stage Skin Liver Gut Functional impairment 0 (None) 0 0 0 0 I (Mild) 1 to 2 0 0 0 II (Moderate) 1 to 3 1 1 1 l m III (Severe) IV (Life-threatening) n3 2 to 2oto 3 2 to 4 2 to 4 p2 to 3 q 2 to 4 r 2 3 (Adapted from; http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=cmed6.table. 17337). vacuolar degeneration of the basal cell layer are found (Chapter 2). The number of Langerhans cells decreases. Differential diagnosis GVHD needs to be differentiated from drug-induced skin reactions, eruptions of peripheral lymphocyte recovery accompanying a graft (generally 10 to 14 days after transplant), and viral infections. Clinical images are available in hardcopy only. d e f g h i j k Fig. 10.8-2 Acute graft-versus-host disease (GVHD). d, e: Diffuse small erythema coalesce into red plaques. Treatment Immunosuppressants (cyclosporine, tacrolimus, azathioprine, cyclophosphamide) and steroids are administered orally, Posttransfusion GVHD can be prevented by irradiating the blood to p q l m n o r be transfused. 2. Viral eruption When maculopapular erythema appear abruptly on the whole body of a febrile patient who has been adiministered NSAIDs or any other medicine for that condition, a drug reation or a viral infection are the two most likely diagnoses. In those cases, differentiation between drug-induced eruption and viral eruption is often difficult, even with thorough examination. Drug-induced hypersensitivity syndrome (DIHS) is thought to be caused by causative drug as well as re-activation of latent viral infection. Refer to Chapter 23 for details on viral infections. Go Back to the Top To Order, Visit the Purchasing Page for Details