Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
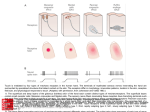
OMM3 #2 Wed, Aug 6, 2003 2-3pm Chad McCormick Dr. McGill Page 1 of 7 I. General a. Definitions i. PAIN: (IASP) Unpleasant sensory and emotional experience associated with potential or actual tissue damage ii. PAIN: a conscious experience which may be influenced by alterations in somatosensory processing following injury as well as psychosocial factors. iii. SUFFERING: a state of severe distress associated with events that threaten the intactness of the individual b. SCOPE OF THE PROBLEM i. Nine in ten have pain at least once a month ii. 15% have severe pain iii. Majority of us will suffer disabling pain iv. 2 million in US disabled with back pain v. COST: 80 billion dollars a year vi. 58% of chronic pain patients are depressed vii. Most pain RX is by the patient or primary care physician viii. 50% have an anxiety disorder II. Mechanisms of Pain a. PROCESS OF PAIN i. TRANSDUCTION 1. Noxious Stimuli translated into impulses 2. Three types of fibers a. A-beta i. Large diameter non-nociceptive ii. Touch, moving stimuli b. A-delta i. Small diameter, fast nociceptors ii. Produce sharp pain iii. Pain not reduced by morphine c. C OMM3 #2 Wed, Aug 6, 2003 2-3pm Page 2 of 7 i. Small diameter, unmyelinated ii. Slow nociceptors (up to 1 minute) iii. Non-specific iv. no localized pain v. pain relieved by morphine 3. Up to 50% of A-Delta and C fibers are “silent” 4. Chemical mediators a. Potassium b. Serotonin c. Bradykinin d. Histamine e. Prostaglandins f. Leukotrienes g. Substance P ii. TRANSMISSION 1. Propagation throughout the nervous system (From dorsal horn to cortex) 2. Encoding of a generator potential into an impulse train 3. Varies with afferent type and conditions 4. Involves nociceptor fibers (non-linear) 5. Neurotransmitters a. Exitatory Amino Acids i. AMPA, NMDA receptors b. Monoamines Noradrenaline i. Alpha1 receptors c. Monoamines Dopamine i. D- 1,5 receptors d. Monoamines 5-Hydroxytryptamine OMM3 #2 Wed, Aug 6, 2003 2-3pm Page 3 of 7 i. 5HT2,7 receptors iii. MODULATION 1. Nociceptive transmission modified through neural influences 2. Descending pathways can alter or inhibit 3. Transmission Modified Through a. Inhibitory Amino Acids i. GABA-a and GABA-b receptors b. Monoamines Noradrenaline i. Alpha2 receptors c. Monoamines Dopamine i. D-2,3,4 receptors d. Monoamines 5-Hydroxytryptamine i. 5HT1 e. Monoamines Opioids i. MU, DELTA, KAPPA, ORLI iv. PERCEPTION 1. Interacts with unique psychology of individuals to create the final experience of “pain” 2. Reticular system 3. Somatosensory cortex 4. Limbic system (emotions) III. Pathways a. Gating Mechanism (seen in the power points) i. touch sensation overcomes pain sensation due to gate being turned on and off ii. diagrams in powerpoints have been excluded for space and time conservation OMM3 #2 Wed, Aug 6, 2003 2-3pm Page 4 of 7 IV. V. THREE DIMENSIONS OF PAIN a. Sensory-discriminative b. Affective-motivational c. Evaluative NEUROMATRIX MODEL a. Neuromatrix i. Large widespread network of neurons between the thalamus and cortex, and between the cortex and limbic system. The distribution and synaptic links are determined genetically and later sculpted by sensory inputs. b. c. d. VI. VII. Body-self neuromatrix (Neurosignature) i. A characteristic pattern implanted by the patterns of repeated cyclic processing and synthesis of nerve impulses throughout the neuromatrix Sentient neural hub i. The area of the brain in which the stream of nerve impulses is converted into a continuously changing stream of awareness and may also activate muscle movement. New Conceptual Nervous System Components i. The body-self neuromatrix ii. Cyclic processing and synthesis in which the neurosignature is produced iii. The sentient neural hub (SNH) which converts the flow of neurosignatures into the flow of awareness. iv. Activation of an action neuromatrix to provide the pattern of movements to bring about the desired goal. CONVERGENCE a. Both specialized and “network” components b. Lamina I Spino-thalamo-cortical pathway c. i. Specialized neural system Lamina V Integrative, intensity-related TAKEAWAY POINTS a. Pain is a highly complex phenomenon involving multiple structures and psychophysiological processes with constant counterbalancing of facilitative and inhibitory processes. b. VIII. OMM3 #2 Wed, Aug 6, 2003 2-3pm Page 5 of 7 Just one manifestation of the mind-body's hemeostasis system (AD Craig, Specificity and Integration in Central Pain Pathways, 10th World Congress on Pain, 2002) How does Pain change from Acute to Subacute? a. SENSITIZATION i. Peripheral 1. Inflammation mediators sensitize nociceptor endings 2. Will now respond to weak stimuli i.e. Touch, soreness and aching of deep tissues ii. Central 1. Abnormal amplification 2. Amplifies signals from low threshold A-beta fibers 3. Noxious stimuli can produce primary and secondary hyperalgesia b. State: Normal Transmission i. Stimulus Low High ii. Afferent A-Beta A-Delta/C iii. Sensation c. d. Innocuous Pain iv. Syndrome Physiological Sensibility v. Change Normal Transmission State: Suppressed i. Stimulus High ii. Afferent A-Delta/C iii. Sensation Innocuous iv. Syndrome Hyposensibility v. Change Reduced Exitation vi. Increased Inhibition State: Sensitized (transient) i. Stimulus Low High ii. Afferent A-Beta A-Delta/C iii. Sensation Allodynia Hyperalgesia iv. Syndrome Hypersensible Inflammatory v. vi. Change Neuropathic Increased Reduced vii. e. exitation OMM3 #2 Wed, Aug 6, 2003 2-3pm Page 6 of 7 inhibition State: Reorganized+ (persistent) i. Stimulus Low High ii. Afferent A-Beta A-Delta/C iii. Sensation Allodynia Hyperalgesia iv. Syndrome Peripheral Central v. neuropathic neuropathic vi. pain pain vii. Change Structural Reoganization Experience of subacute pain i. Variable unpleasantness ii. Movement activates sensitized receptors iii. Feeling of weakness, somnolence, exhaustion iv. Emotions: fear, anger, helpless, embarrassment, remorse v. Expectation the storm will pass Properly Used Drugs and Pre-emptive Analgesia May Help to Prevent subacute Pain f. IX. How Does Subacute Pain Become Chronic Pain? a. Gradual process (6 months or less) b. Not directly tied to late neurophysiological changes c. Varies by condition, physical status, and age d. X. XI. i. i.e., low risk with appendectomy, but 50% of thoracotomy patients Behavior a major contributor i. Inactivity ii. Abnormal posture and gait trigger added physical disorders e. Emotional changes f. Dependency on medications g. Preoccupation with pain h. Social support system i. Pain may become “centralized : changes in CNS anatomy and physiology Diagnostic Phase : Comprehensive evaluation essential a. History b. Physical Examination c. Psychological/Behavioral Evaluation d. Appropriate diagnostic tests MEASUREMENT OF PAIN Required by JCAOH Guidelines OMM3 #2 Wed, Aug 6, 2003 2-3pm Page 7 of 7 a. GOOD NEWS: SIMPLE IS BEST i. Visual Analog Scale VISUAL ANALOG PAIN SCALE 0___________________________100 Place a mark on the line representing your pain level ii. Faces Scale (Not included) XII. TREATMENT a. Acute management b. Invasive procedures c. Analgesics d. The best treatment for chronic pain is prevention through good acute pain management.